Causes of chronic abdominal pain
Study/case series/case report
Number of patients studied
Outcome
Time interval follow-up
Complications
Mesenteric ischemia
Ceballos et al. [26]
1
8 to 0 VAS
1 year
None
Esophageal dysmotility
Jackson and Simpson [27]
1
9 to 3 VAS
>2 years
Two lead fractures
Irritable bowel syndrome
Krames and Mousad [29]
1
9-10 to 2-3 VAS
6 months
None
Chronic pancreatitis
Khan et al. [32]
5
Average 4.9 VAS decrease, >50 % opioid use decrease
>1 year
Lead migration
Familial Mediterranean fever
Kapur et al. [34]
2
8 to 5 VAS
1 year
None
10 to 1 VAS
3 months
Gastroparesis
Tiede et al. [28]
2
8 to 3 VAS
3 months
Lead migration
9 to 2 VAS
Chronic pancreatitis
Kapural and Rakic [31]
1
6 to 1 VAS
3 months
None
150 mg MSO4 to 0
Chronic pancreatitis
Kim et al. [33]
1
10 to 5 VAS
14 months
None
Chronic pancreatitis, abdominal adhesions, gastroparesis, mesenteric ischemia, postgastric bypass pain
Kapural et al. [30]
35
VAS from 8.2 to 3.8
1 year
Infection (n = 3)
MSO4 from 119 to 38 mg
Lead migration (n = 1)
Chronic pancreatitis, postsurgical intraabdominal adhesion, gastroparesis
Kapural et al. [35]
70
VAS from 8 to 2.49
Average 84 weeks
Infection and Lead migration (n = 8)
MSO4 from 158 to 36 mg
Chronic pancreatitis
Kapural et al. [37]
30
VAS from 8 to 3.6
1 year
Infection (n = 2)
MSO4 from 165 to 48.6 mg
Lead migration (n = 1)
Chronic pancreatitis
Al-Mahrouqi et al. [41]
1
680 mg to 510 mg MSO4 with “effective pain control”
9 months
None
Irritable bowel syndrome
Rana et al. [38]
1
VAS from 8-10 to 3
1 year
None
Mesenteric ischemia
Caruso et al. [39]
1
VAS from 8 to 2
1 month
Pocket infection
Bannayan–Riley–Ruvalcaba syndrome
Yakovlev and Resch[40]
1
VAS from 6 to 0
6 months
None
The first case report on SCS for the treatment of abdominal pain described a 78-year-old male with chronic, unrelieved severe postprandial pain caused by mesenteric ischemia. The patient experienced complete pain relief after SCS lead was placed in the epidural space at the T6 vertebral level and stimulation initiated [26]. A case report dealing with irritable bowel syndrome (IBS) described a female patient who suffered from 11 to 14 diarrheal episodes per day and extreme pain from IBS. After placement of a thoracic SCS system, the patient immediately became diarrhea free. However, her initial reduction in pain relief was not sustained [29, Table 1].
Khan et al. [32] described five successful cases of pain relief in patients with nonalcoholic pancreatitis who were trialed with both single and dual leads placed at the T5–T7 vertebral level in the posterior epidural space (Fig. 19.1). This report was followed by several others describing improvements in pain and function in patients with severe chronic pancreatitis [30–33] (see Table 19.1). Tiede and associates [28] described improvements in pain scores of patients with gastroparesis, and Jackson and Simpson [27] reported improved pain control and swallowing in a patient with a rather complicated history of esophageal problems.
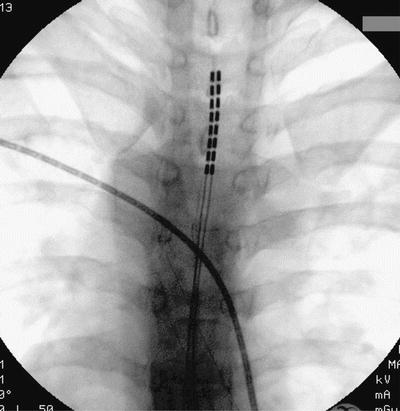
Fig. 19.1
Properly positioned two octrode leads shown here during fluoroscopic anterior–posterior (AP) radiograph of thoracic spine. Leads placed in posterior epidural space with tip of the leads reaching T5 is the most frequent lead positioning when used for the SCS in painful gastrointestinal disorders
A more recently published report describes two cases of familial Mediterranean fever (FMF) in which intermittent painful abdominal attacks responded positively to SCS at the T8–T9 and T7–T8 vertebral levels respectively [34].
Despite initial enthusiasm for a novel modality of treatment for severe abdominal pain, interpreting such limited published experience was further complicated by the fact that there was considerable variability in patient selection, lead positioning, and type of hardware used in these reports. Consequently, it has remained unclear whether a reasonable fraction of patients may have long-term benefit from stimulation.
More recently, a larger clinical retrospective review using SCS for treatment of chronic abdominal pain has been published [30] studied 35 patients and provided long-term (1 year) clinical follow-up data. Consistent with most technical descriptions in previous reports, SCS lead tips were positioned at T5 (n = 11; Figs. 19.1 and 19.2) or T6 (n = 10) height within the epidural space. Thirty patients (86 %) reported at least 50 % pain relief on completion of the trial (Fig. 19.3). Among 28 patients who received permanent implant, 19 were followed for at least 1 year. Their visual analog scale (VAS) pain scores remained low (3.8 ± 1.9 cm; p < 0.001) at 1 year, as did opioid use of 138.3 ± 134 to 38 ± 48 mg morphine equivalents (Fig. 19.4). This report for the first time suggested that SCS may provide consistent long-term improvements and be a useful therapeutic option for patients with severe visceral abdominal pain. A national survey was conducted to develop a consensus on patient selection and technical aspects of SCS for abdominal visceral pain, where 76 case reports were collected [35]. This brief survey confirmed that SCS for abdominal visceral pain is still rarely used, despite a possibility of high therapeutic success rates. Causes for this include very few studies describing the basic mechanisms of neuromodulation for longstanding visceral pain, comfort levels by the physicians, and issues with coverage of such treatment by payers. The technical aspects of SCS for the treatment of abdominal visceral pain seem to be uniform among physicians who use such technology across the United States and are also consistent with our larger retrospective study described previously [30, 35]. In most patients, the SCS leads were positioned with their tips at the level of the T5 (26 patients; Fig. 19.2) or T6 vertebral body (15 patients). Pain relief exceeded 50 % in 66 of 70 patients reported. VAS pain scores before an implant were 8 ± 1.9 cm, whereas after the implant they were 2.49 ± 1.9 cm. Opioid use before an implant was 158 ± 160 mg; at the last office visit after the implant, it was 36 ± 49 mg. The weakness of this survey was that the subgroup of responding physicians may not adequately represent the population of all of the physicians who trialed SCS for chronic visceral abdominal pain but rather those who had largely positive results. However, the goal of the survey was to examine technical aspects of SCS for chronic abdominal pain, and not the efficacy of spinal cord stimulation [35].
 Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
 Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
 Peripheral Nerve Stimulation for Chronic Abdominal Pain
Peripheral Nerve Stimulation for Chronic Abdominal Pain
 The Epidemiology of Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain



Related posts:
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Peripheral Nerve Stimulation for Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain
Full access? Get Clinical Tree
