▪ PATHOPHYSIOLOGY AND DIAGNOSIS
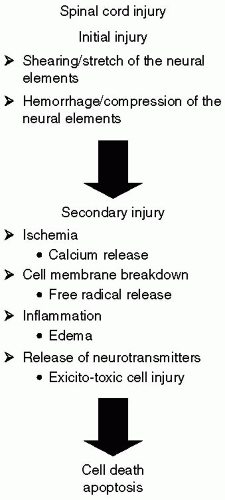
In a patient with trauma, failure to identify preoperative cervical instability may result in devastating neurologic
injury. Complete spinal cord transection at a high cervical level (C1) results in pentaplegia: Paralysis of the lower cranial nerves, the diaphragm, and loss of sensation and motor function of all four extremities. Quadriplegia refers to injuries at C3-C5, which results in the loss of sensation and motor function of all four extremities, as well as impairment of the diaphragm, while the cranial nerves and sensation to the face and neck and accessory muscles of the neck are spared. Tetraplegia refers to injuries involving C5 and C6, in which diaphragmatic function is retained as well as some movement of the upper extremity, but there is a total loss of function of the lower extremities. Paraplegia refers to injuries below T1, resulting in loss of function of the lower extremities.
14Incomplete SCI syndromes are listed in
Table 28.1. Of these, the central cord syndrome is the most common. These patients frequently require surgery, either for spinal stability or an associated injury, presenting the anesthesiologist with the quandary of managing a patient with a potential cervical spine injury. Because of the potential for catastrophic neurologic injury, nearly every blunt trauma victim is routinely subjected to a plain film radiographic cervical spine series. A complete series must minimally include a lateral cross-table cervical spine, an anterior-posterior view, and an open-mouth odontoid view. The occipitocervical junction and all seven cervical vertebrae, including the C7-T1 junction, must be viewed.
To better delineate those emergency department patients who may be at low risk for cervical spine injury, Hoffman et al. embarked upon the National Emergency X-Radiography Utilization Study (NEXUS) in an attempt to better define those patients requiring radiographic cervical spine evaluation.
15 More than 34,000 patients were enrolled at 21 medical centers across the United States.
16 The NEXUS low-risk criteria (see
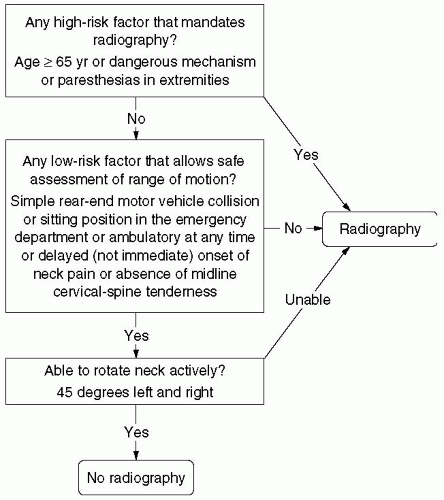
Table 28.2) were found to be 99.6% sensitive and 12.9% specific for cervical spine injury. In addition, Stiell et al. formulated the Canadian Cervical Spine Rule (see
Fig. 28.2) which encompasses criteria similar to the NEXUS low risk criteria and additionally requires the patient to rotate his head.
17 This large, multicenter study of 8,283 patients yielded a sensitivity of 99.4% and specificity of 45.1%. Although a contentious debate as to the superiority of one criterion versus the other continues, both studies suggest that many patients are needlessly radiographed, and that many cervical spines may be “cleared” in the emergency department based on clinical factors.
Unfortunately, radiographic examination of the spine may not detect an uncommon SCI. Hendey et al. evaluated the data provided by the NEXUS study to better determine the incidence of SCIWORA.
18 SCIWORA is defined as SCI demonstrated by MRI when complete and adequate cervical spine plain radiographs revealed no injury. A total of 34,069 patients were entered into the NEXUS database; 818 (2.4%) had cervical spine injury. Twenty-seven (0.08%) were patients with SCIWORA with a variety of MRI findings (see
Table 28.3). Of note, all 27 patients were found to have at least one documented clinical finding which did not meet the low-risk NEXUS criteria, and all were evaluated with plain radiograph films upon initial presentation.
The NEXUS study revealed a typical distribution of cervical fractures (C2 23.9%, C6 20.25%, C7 19.08%, C5 14.98%) and subluxations (C5-6 25.11%, C6-7 23.77%, C4-5 16.96%) (15). Of most importance is the recognition of those fractures that result in an unstable neck (see
Table 28.4), as those patients are at greatest risk of suffering permanent neurologic injury. In summary, trauma patients, particularly those who do not meet the NEXUS or Canadian low-risk criteria, should be treated as if they have an unstable spine.
Figures 28.3 and
28.4 are the radiographs of a trauma patient who sustained a C6-7 subluxation, resulting in quadriplegia. Although the plain radiograph clearly demonstrates the C6-7 subluxation, the computed tomography (CT) reconstruction presents fine detail of the bony architecture.
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree