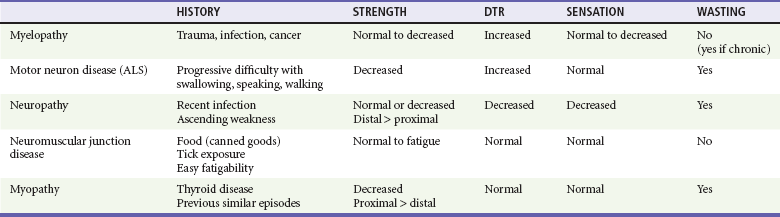
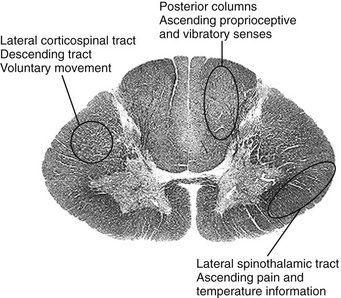
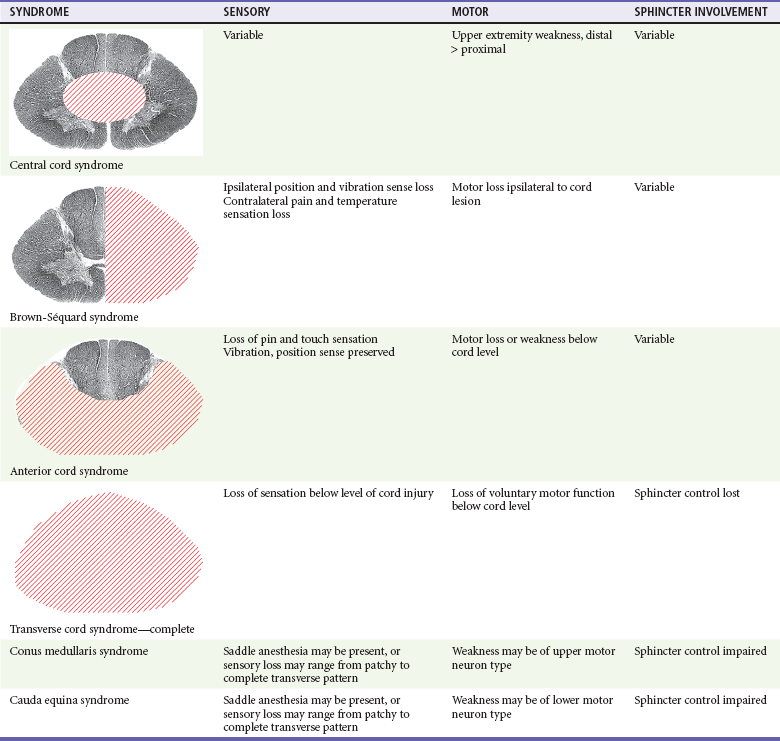
Chapter 106 This chapter generally is concerned with nontraumatic processes affecting the spinal cord and its vascular supply as well as processes compressing the spinal cord. Spinal cord trauma is discussed in Chapter 43. For clinical purposes, neuroanatomy of the spinal cord may be greatly simplified, as depicted in Figure 106-1. Major ascending sensory tracts are represented on the right side of the figure, with motor tracts on the left side. The posterior columns carry afferent ascending proprioceptive and vibratory information on the ipsilateral side of the cord to the area stimulated; decussation of these fibers occurs in the medulla so that contralateral cortical representation is consistent. The lateral spinothalamic tract conveys afferent information about pain and temperature in a portion of the lateral column of white matter. (Tracts are named with the point of origin first; the spinothalamic tract, for example, arises in the spinal cord and travels to the thalamus.) The tract is laminated so that sacral fibers are represented most laterally. Crossing of fibers from this tract occurs near the level of entry of the spinal nerve; a cord lesion affecting only one lateral spinothalamic tract results in decreased or absent pain and temperature perception below the level of injury on the contralateral side of the body. Complete spinal cord lesions may be manifested as either acute or subacute pathologic processes. A complete spinal cord lesion is defined as a total loss of sensory, autonomic, and voluntary motor innervation distal to the spinal cord level of injury. Reflex responses mediated at the spinal level, such as muscle stretch (deep tendon) reflexes, may persist, although they also may be absent or abnormal. Autonomic dysfunction may be manifested acutely with hypotension (neurogenic shock) or priapism. The most common cause of the complete transverse cord syndrome is trauma, although this anatomic syndrome is nonspecific as to etiology.1,2 Other causes of acute complete cord syndrome include infarction, hemorrhage, and entities causing extrinsic compression. In patients with acute complete transverse syndromes that persist for more than 24 hours, functional recovery does not occur in 99%.3,4 Any evidence of preserved cord function below the level of injury denotes a partial rather than a complete lesion. Signs such as persistent perineal sensation (sacral sparing), reflex rectal sphincter tone or voluntary rectal sphincter contraction, and even slight voluntary toe movement suggest a partial cord lesion, which usually carries a better prognosis than a complete lesion.1 Spinal shock refers to the loss of muscle tone and reflexes with complete cord syndrome during the acute phase of injury. The intensity of the spinal shock increases with affected spinal cord level.5 Spinal shock typically lasts less than 24 hours but has been reported occasionally to last days to weeks.5,6 A marker of spinal shock is loss of the bulbocavernosus reflex, which is a normal cord-mediated reflex that may be preserved in complete cord lesions. The bulbocavernosus reflex involves involuntary reflex contraction of the anal sphincter in response to a squeeze of the glans penis or a tug on the Foley catheter. The termination of the spinal shock phase of injury is heralded by the return of the bulbocavernosus reflex; increased muscle tone and hyperreflexia follow later.1,5,6 Incomplete spinal lesions are characterized by preservation of function of various portions of the spinal cord. Of all incomplete spinal lesions, most can be classified generally as one of three clinical syndromes: central cord syndrome, Brown-Séquard syndrome, or anterior cord syndrome (Table 106-1). Central cord syndrome, first described by Schneider and colleagues in 1954, is the most prevalent of the partial cord syndromes.7,8 Because of the anatomic organization of the spinal cord, a central cord injury is characterized by bilateral motor paresis; upper extremities are affected to a greater degree than lower extremities, and distal muscle groups are affected to a greater degree than proximal muscle groups. Sensory impairment and bladder dysfunction are variable features. At times, burning dysesthesias in the upper extremities may be the dominant feature.9 Central cord injury affects the central gray matter and the central portions of the corticospinal and spinothalamic tracts. It is caused most often by a hyperextension injury; the postulated mechanism is squeezing or pinching of the spinal cord anteriorly and posteriorly by inward bulging of the ligamentum flavum. The most common cause of such injuries is a fall, followed in frequency by a motor vehicle crash.7,8 The result is contusion to the spinal cord, with the central portion being most affected. This injury often occurs in elders with degenerative arthritis and spinal stenosis in the cervical area but may affect any patient with cervical canal narrowing of any etiology (e.g., congenital narrow canal as seen in achondroplasia or canal narrowing from disk protrusion or tumor). The prognosis with central cord syndrome depends on the degree of injury at presentation and the patient’s age.10,11 In patients younger than 50 years, more than 80% regain bladder continence, and approximately 90% return to ambulatory status. In patients older than 50 years, only 30% regain bladder function, and approximately 50% regain the ability to ambulate.11 Brown-Séquard syndrome, first described in 1846 by the one physician for whom it is named,12 is the result of an anatomic or functional hemisection of the spinal cord. Usually associated with penetrating injuries,13 Brown-Séquard syndrome also may be seen with compressive or intrinsic lesions. The syndrome has been reported in association with spinal cord tumors, spinal epidural hematoma, vascular malformations, cervical spondylosis, degenerative disk disease, herpes zoster myelitis, and radiation injury and as a complication of spinal instrumentation.13,14 The syndrome in its pure form is characterized by ipsilateral loss of motor function and proprioception or vibration, with contralateral loss of pain and temperature sensation below the spinal cord level of injury. Because fibers associated with the lateral spinothalamic tract ascend or descend one or two spinal cord segments before crossing to the contralateral side, ipsilateral anesthesia (pain and temperature modalities) may be noted one or two segments above the lesion, although this observation is variable. Most patients with Brown-Séquard syndrome incur only partial sensory and motor impairment, and the classic pattern is not seen.11,13,15 Brown-Séquard syndrome carries the best prognosis of any of the incomplete spinal cord syndromes. Fully 80 to 90% of patients with Brown-Séquard syndrome regain bowel and bladder function, 75% regain ambulatory status, and 70% become independent in their activities of daily living.11 Anterior cord syndrome is characterized by loss of motor function, pinprick, and light touch below the level of the lesion with preservation of posterior column modalities, including some touch, position, or vibratory sensation. Although most reported cases of anterior spinal syndrome follow aortic surgery,16 the syndrome also may occur after severe hypotension, infection, myocardial infarction, vasospasm from drug reaction, and aortic angiography.17 The anatomic lesion may be caused by a cervical hyperflexion injury resulting in a cord contusion or by protrusion of bone fragments or herniated cervical disk material into the spinal canal. Rarely, it is produced by laceration or thrombosis of the anterior spinal artery or a major radicular feeding vessel.11 Patients present with characteristic mixed motor and sensory neurologic findings as noted before. Functional recovery varies; most improvement occurs during the first 24 hours, but little improvement is expected thereafter.4 Although anterior cord lesions from ischemia usually are incomplete, patients without motor function at 30 days have little or no likelihood of regaining any motor function by 1 year.16,18 Overall, only 10 to 20% of patients with this entity regain some muscle function, and even in this group, there is little power or coordination.11 The separation of conus medullaris and cauda equina lesions in clinical practice is difficult because the clinical features of the disorders overlap. In addition, a combined lesion may occur that masks clear clinical symptoms or signs of either an upper or a lower motor neuron type of injury. The conus medullaris is the terminal end of the spinal cord, located at approximately the L1 level in adults. The conus medullaris syndrome may involve disturbances of urination (usually from a denervated, autonomic bladder that is manifested clinically with overflow incontinence) and sphincter impairment or sexual dysfunction. Sensory involvement may affect the sacral and coccygeal segments, resulting in saddle anesthesia. Pure lesions of the conus medullaris are rare.19 Upper motor neuron signs, such as increased motor tone and abnormal reflexes, may be present, but their absence does not exclude the syndrome. The conus medullaris syndrome can be caused by central disk herniation, neoplasm, trauma, or vascular insufficiency. Because the conus is such a small structure, with lumbar and sacral segments represented in a small area, a lesion usually causes bilateral symptoms. This finding may help distinguish lesions of the conus from lesions of the cauda equina, which often are unilateral.19 The cauda equina (Latin for “horse’s tail”) is the name given to the lumbar and sacral nerve roots that continue on within the dural sac caudal to the conus medullaris. Not a true “cord syndrome,” cauda equina syndrome represents dysfunction at the level of nerve roots, but the anatomic clustering of nerve roots within the lumbar dural sac allows injury to several nerve roots to occur simultaneously. The etiologic lesion in the cauda equina syndrome usually is a midline rupture of an intervertebral disk, most commonly at the L4-5 level. Tumors and other compressive masses also may cause the syndrome. As in the conus medullaris syndrome, patients generally present with progressive symptoms of fecal or urinary incontinence, impotence, distal motor weakness, and sensory loss in a saddle distribution. Muscle stretch reflexes also may be reduced. Urinary retention is the most consistent finding, with a sensitivity of 90%.20 Low back pain may or may not be present. 0. No firing of the muscle is present. 1. The muscle fires but is unable to move the intended part. 2. The muscle is able to move the intended part with gravity eliminated. 3. The muscle is able to move the intended part against gravity. 4. The muscle is able to move the intended part, but not at full strength. Muscle stretch (deep tendon) reflexes may be tested rapidly at the bedside. Responses are graded on a scale of 0 to 4+, with 2 being normal. Hyperactive reflexes suggest upper motor neuron disease (affecting the neurons or their outflow from the brain or spinal cord), as do sustained clonus and Babinski’s sign. The absence of these reflex changes does not constitute evidence that a myelopathy is not present. In fact, one small series noted a low incidence of extensor plantar responses as well as a lack of hyperreflexia in patients presenting to the ED with acute or progressive cord compression or myelopathies.21 Reflexes also may be diminished or absent when sensation is lost or when spinal shock is present. Diseases of muscles or neuromuscular junctions also may decrease reflexes. In acute cord injury, reflexes may be diminished in the acute phase. The bulbocavernosus reflex may be helpful in this assessment. The prime principle in management of spinal cord dysfunction is to consider and exclude potentially treatable clinical conditions. The clinical assessment of spinal cord dysfunction is limited to detection of weakness, sensory alterations, sphincter dysfunction, and perhaps reflex abnormalities. There may be pain in the back, depending on the pathologic process, but generally it is not helpful in formulating a list of considerations for the differential diagnosis. Because potential functional loss and impact on quality of life are great, the detection of a process for which some intervention is possible assumes great importance. A likely diagnosis of spinal cord infarction may be entertained, but the pursuit of a treatable process, such as spinal cord compression from an epidural hematoma, should be seriously considered.22 This discovery process may involve specialty consultation or studies that may not be readily available in all settings, such as MRI. As a general rule, liberal use of consultation and imaging is recommended when the possibility of spinal cord dysfunction is considered. The history may suggest a specific cause and will guide the tempo of investigation. The caveat is that spinal cord diseases may mimic many other disease processes, and neither the history nor physical examination may allow diagnosis until appreciable neurologic dysfunction has developed. The picture of a complete transverse spinal cord syndrome with paraplegia, sensory loss at a clear anatomic level, and sphincter dysfunction cannot be fully simulated by other anatomic lesions. Incomplete or evolving spinal cord syndromes may be imitated by other disease processes. It is always prudent to focus the differential diagnosis on anatomic considerations—the classic “where is the lesion?” approach (Table 106-2). Progressive lower extremity weakness and sensory alteration may represent cord dysfunction but could reflect an intracranial vertex mass with bilateral cortical dysfunction. Ataxia may be a finding in cerebellar disease but also has rarely been reported as an isolated finding with spinal cord compression. Another example is rapidly progressive paralysis in a patient with areflexia and quadriplegia; ascending paralysis (Landry-Guillain-Barré syndrome) at times may mimic an acute cord lesion. Table 106-2 Clinical Characteristics of Neuromuscular Diseases ALS, amyotrophic lateral sclerosis; DTR, deep tendon reflex.
Spinal Cord Disorders
Perspective
Principles of Disease
Classification of Spinal Cord Syndromes
Complete (Transverse) Spinal Cord Syndrome
Incomplete Spinal Cord Lesions
Central Cord Syndrome
Brown-Séquard Syndrome
Anterior Cord Syndrome
Conus Medullaris and Cauda Equina Syndromes
Clinical Features
Physical Examination
Motor Function
Reflexes
Differential Considerations





Full access? Get Clinical Tree


