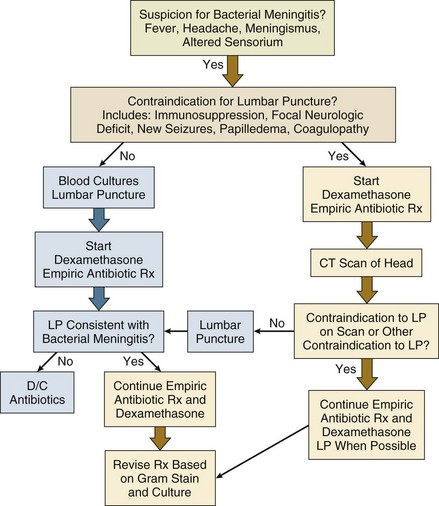
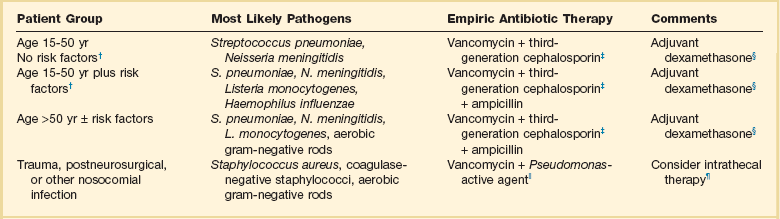
54 OVERWHELMING INFECTIONS OF THE CENTRAL NERVOUS SYSTEM FULMINANT ENDOVASCULAR INFECTIONS Staphylococcus aureus Bacteremia Staphylococcal Toxic Shock Syndrome Streptococcal Toxic Shock Syndrome Clostridial Toxic Shock Syndrome SERIOUS SKIN AND SKIN STRUCTURE INFECTIONS SERIOUS GASTROINTESTINAL AND INTRA-ABDOMINAL INFECTIONS LIFE-THREATENING INFECTIONS OF THE HEAD AND NECK SERIOUS VECTOR-BORNE INFECTIONS POTENTIAL AGENTS OF BIOTERRORISM The annual incidence of bacterial meningitis in individuals older than 16 years of age in developed countries has been steadily decreasing and was estimated at less than 2 cases per 100,000 in the United States in 2006-2007.1–3 In recent studies from the United States and the Netherlands, the predominant organisms in microbiologically confirmed cases of bacterial meningitis in adolescents and adults were Streptococcus pneumoniae (45-60%), Neisseria meningitidis (15-30%), Haemophilus influenzae (7%), and Listeria monocytogenes (5%),2–4 with no pathogen identified in approximately 10% of cases.1,2 Streptococcus agalactiae (group B β-hemolytic streptococcus) has also recently emerged as an important cause of meningitis in adults, causing over 5% of cases of microbiologically defined episodes in the United States from 1998 to 2007. In some studies, rates of culture-negative cases were as high as 25%.5 Important recent changes in microbiologic causes of bacterial meningitis reflect the impact of current vaccination strategies. These changes include the marked reduction in cases of of H. influenzae meningitis in both children and adults, and the introduction of the conjugated pediatric pneumococcal vaccine that has resulted in decreased rates of invasive childhood pneumococcal disease in children and adults.3,6 A new meningococcal vaccine, which has the potential to diminish the rates of meningococcal disease in high-risk populations, has also been approved for use in adolescents and high-risk adult populations.7 Another important trend is the increase in prevalence of nosocomial meningitis.4 The microbiology of nosocomial meningitis differs from that of community-acquired cases, including higher rates of staphylococcal infection and infection due to a variety of aerobic gram-negative organisms. The major route of acquisition of bacterial meningitis follows colonization of the nasopharynx with subsequent hematogenous spread and invasion of cerebrospinal fluid (CSF). Less frequently, infection occurs from hematogenous dissemination from distant sites or from other localized intracranial focal infections including sinusitis, mastoiditis, or otitis, or it is secondary to trauma or neurosurgery. In addition to trauma and contiguous focal infectious processes facilitating invasion of the CSF by bacteria, there is a wide variety of immunologic deficits that result in impaired clearance of encapsulated organisms. These include organism-specific deficits such as terminal complement deficiencies predisposing to meningococcal disease, as well as more general deficits such as immunoglobulin deficiencies, splenectomy, alcoholism, cirrhosis, diabetes mellitus, and human immunodeficiency virus (HIV) infection.2,4 Patients with defects leading to impaired cell-mediated immunity including advanced age and general debility, as well as hematologic malignancies, chemotherapy, and use of tumor necrosis factor (TNF)-β inhibitors, are predisposed to Listeria infection.8 The presenting symptoms of bacterial meningitis include fever, headache, stiff neck, and altered sensorium. In the recent large series of 696 cases from the Netherlands, 95% had at least two of these four symptoms, although only 44% had all of the classic triad of headache, fever, and stiff neck.2 Other important presenting symptoms in this cohort included nausea in 74%, focal neurologic deficits in one third of cases, and Glasgow Coma Score of less than 8 in 14% of cases.2 Rash, especially a petechial or purpural rash that may be an important clue for the diagnosis of meningococcal meningitis, was seen in 26%.2 Presenting symptoms alone without CSF findings or microbiologic data cannot adequately distinguish between bacterial meningitis and viral or other aseptic meningitis. However, certain features are more suggestive of bacterial rather than viral origin including winter versus summer onset, rapid progression of disease, presentation in shock, and presence of another focal site of bacterial infection such as sinusitis, otitis, or pneumonia. In addition to viruses, other nonbacterial infections including cryptococcosis, tuberculous meningitis, rickettsial diseases, Lyme disease, and syphilis are in the differential diagnoses of acute bacterial meningitis. The early management of suspected bacterial meningitis requires careful coordination and appropriate sequencing of the procedures necessary for establishing the diagnosis (lumbar puncture and imaging studies) and the interventions necessary for optimal treatment (antibiotics and dexamethasone). Rapid initiation of therapy leads to improved outcomes but may decrease specific microbiologic yield on CSF analysis.1,5 Similarly, although lumbar puncture can usually be performed safely without any imaging studies, computed tomography (CT) scan may be required to minimize the risk of this procedure, leading to potential delays in institution of antimicrobial therapy.9 Recent reviews and published practice guidelines have tried to place these competing urgencies in perspective, using data culled from multiple recent prospective studies and randomized trials.1,5 One algorithm for early management of bacterial meningitis is shown in Figure 54.1. The primary tenet of these algorithms is that the initiation of treatment assumes highest priority and thus any delay in performing a lumbar puncture because of the need for imaging or because of other patient-specific contraindications should not delay the administration of antibiotic therapy. Brain herniation is a feared but rare complication of lumbar puncture when performed for diagnosis of suspected meningitis in patients with elevated intracranial pressure.10 One recent study of a cohort of 301 patients with suspected bacterial meningitis described the relative safety of lumbar puncture without CT scanning in patients without specific clinical contraindications.9 Proposed criteria for performing imaging prior to lumbar puncture include new-onset seizures, prior CNS disease, immunocompromised state, papilledema, focal neurologic deficits, or moderate to severe impairment of consciousness.5 Only approximately 45% of patients with bacterial meningitis will have criteria for neuroimaging prior to lumbar puncture, although it remains standard practice in many hospitals for all patients with suspected meningitis to undergo imaging first.1,5 The main purpose of early imaging is to find evidence of brain shift and both noncontrast CT and magnetic resonance imaging (MRI) can be used for this purpose. Considerations for the optimal imaging modality may be different when imaging tests are done to manage subsequent complications of meningitis or to better define space-occupying lesions. Other specific contraindications to lumbar puncture include coagulopathies and presence of local processeses overlying the lumbar puncture site such as stasis ulcers, burns, or cellulitis. The diagnosis of bacterial meningitis relies heavily on analysis of CSF parameters including opening pressure, cell count, protein, glucose, and Gram stain and culture. Typically, patients with bacterial meningitis have elevated opening pressures of 200 to 500 mm H2O, including 40% with opening pressure greater than 400 mm in one recent cohort.2,5 White blood cell (WBC) counts may range from 100 to 10,000 cells/mm3, most commonly in the 1000 to 5000 range; very low CSF WBC counts are associated with a worse prognosis.4,5 Usually there is a polymorphonuclear (PMN) cell predominance of 80% or greater, although up to 10% will have a lymphocytic predominance, particularly early on. CSF-to-serum glucose ratios are less than 0.4, and CSF protein levels are nearly always increased.5 In a study comparing cohorts of patients with bacterial and viral meningitis, CSF glucose ratios of less than 0.31, total WBC counts of greater than 2000, and total PMN cell counts of greater than 1180 have been predictive of bacterial rather than viral meningitis.11 Other studies have suggested that protein values of greater than 0.5 g/L and WBC counts greater than 100 are also independently predictive of bacterial meningitis.12 Gram stains are positive in 60% to 90% of cases of bacterial meningitis, and results on Gram stain are reported to be 97% specific as to cause.5 Yield of Gram stain is higher on specimens concentrated by Cytospin centrifuge. Highest diagnostic yield from Gram staining is for S. pneumoniae meningitis; Gram stains in Listeria meningitis are positive in only one third of cases because of the lower inoculum of bacteria in the CSF. Clinicians should also be aware that preliminary “stat” Gram stains done during off-hours are more likely to be misinterpreted; thus, stains should always be reviewed by trained clinical microbiologists before modifying therapy based on a Gram stain report. In untreated patients, cultures will ultimately be positive in up to 90% of cases. Initiation of antibiotic therapy prior to lumbar puncture will not significantly alter cell count, protein, glucose, and even Gram stain results but will decrease CSF culture yield by up to 20%.5,12 Blood cultures should be performed in all patients with suspected bacterial meningitis prior to initiation of antibiotics, even if the lumbar puncture is delayed. Additional CSF and blood tests have been used to confirm a diagnosis of bacterial meningitis or help distinguish bacterial from viral disease. Latex agglutination tests for bacterial antigens, although initially reported to have good sensitivity and specificity for diagnosis of specific bacterial meningitis pathogens, have more recently been shown to contribute little to the management of most patients with suspected meningitis.12 Polymerase chain reaction (PCR) of CSF for bacterial deoxyribonucleic acid (DNA) may be useful to confirm an etiologic diagnosis in culture-negative cases, especially those with prior antibiotic therapy, but is not routinely available in most hospitals. Elevated serum C-reactive protein (CRP) levels (>20 mg/L) and elevated serum procalcitonin (>0.5 ng/mL) are not specific for bacterial meningitis but had high predictive value in distinguishing between cohorts of children with bacterial and viral meningitis.12 The level of soluble triggering receptor on myeloid cells in CSF has also been reported to distinguish between bacterial and viral meningitis.12 Additional CSF studies may be useful for diagnosis of other specific infections such as CSF cryptococcal antigen and Venereal Disease Research Laboratory (VDRL) slide test. Initial antibiotic therapy for suspected bacterial meningitis is most commonly initiated in the absence of culture and even Gram stain data. Initial empiric therapy must include agents active against the most likely pathogens based on the patient’s age and underlying illnesses and modified for other specific risk factors such as nosocomial acquisition (Table 54.1). Treatment regimens must take into account local rates of antimicrobial resistance, particularly rates of high-level resistance to penicillin and third-generation cephalosporins in S. pneumoniae. Standard regimens include vancomycin administered at doses targeted to achieve adequate CSF levels (serum troughs of 15 to 20 µg/mL) and a third-generation cephalosporin, either ceftriaxone or cefotaxime. In areas with increased rates of resistance to third-generation cephalosporins, rifampin may be added. When there is risk for Listeria infection based on age greater than 50 or on other specific risk factors such as alcoholism or altered immunity, high-dose ampicillin is included in the treatment regimen. For patients with nosocomial or postprocedure-related infections, cefotaxime or ceftriaxone may be changed to an agent with improved activity against nosocomial gram-negative organisms including Pseudomonas aeruginosa. Initial empiric therapy is modified on the basis of identification and susceptibility data of isolated pathogens. Standard recommended treatment durations are 7 days for meningococcal disease and H. influenzae, 10 to 14 days for S. pneumoniae, and 21 or more days for Listeria.1,5 Table 54.1 Treatment of Bacterial Meningitis in Adults* *Patients older than 15 years of age. †Risk factors: altered immunity including human immunodeficiency virus (HIV) infection and alcoholism. ‡Third-generation cephalosporin: ceftriaxone or cefotaxime; for highly penicillin-allergic patients an alternative would be aztreonam or a fluoroquinolone. §Evidence for benefit of adjuvant dexamethasone is limited. Consider addition of rifampin in settings with high rates of cephalosporin resistance. ||Includes cefepime or ceftazidime; alternatives include aztreonam, meropenem, and ciprofloxacin. ¶For multiresistant organisms or catheter-related infections. Most recent experience is with aminoglycosides or polymyxins. Modified with permission from van de Beek D, de Gans J, Tunkel AR, et al: Community-acquired bacterial meningitis in adults. N Engl J Med 2006;354:44-53; and Tunkel AR, Hartman BJ, Kaplan SL, et al: Practice guidelines for the management of bacterial meningitis. Clin Infect Dis 2004;39:1267-1284. Studies in high-income countries have demonstrated the benefits of adjuvant dexamethasone in decreasing mortality rates and neurologic sequelae in patients with bacterial meningitis, and adjuvant steroids are now part of meningitis practice guidelines in the United States and Europe.5,13,14 In one large, randomized, placebo-controlled trial of 301 adults with suspected bacterial meningitis and cloudy CSF, adjuvant dexamethasone decreased mortality rates from 15% to 7% and decreased unfavorable outcomes from 25% to 15%.13 Benefits of corticosteroids were most evident in those with pneumococcal infection and those with a moderately impaired level of consciousness; patients with meningococcal disease had generally better outcomes with or without corticosteroids. More recent trials from resource-limited settings including Malawi and Vietnam have failed to confirm the benefits of adjuvant steroids, even in those with documented pneumococcal infection, calling into question the generalizability of use of steroids in all settings.12,14 A recent meta-analysis was unable to clearly demonstrate benefits or harm with use of adjuvant corticosteroids.14 If steroids are to be used, the standard regimen based on published and animal studies is 10 mg of dexamethasone every 6 hours for 4 days and initiated prior to or concurrent with the first dose of antibiotics.1,5 Any benefit of steroids initiated after onset of antibiotic therapy is unknown. Patients with suspected or confirmed meningococcal meningitis should be placed in isolation to prevent nosocomial transmission via respiratory droplets for the first 24 hours of therapy. Meningococcal prophylaxis is indicated for household and other close contacts of meningococcal cases including first responders. Conversely, patients with Gram stains and clinical presentations consistent with nonmeningococcal disease should also be quickly identified, to eliminate unnecessary use of meningococcal prophylaxis. Patients with bacterial meningitis often require ICU monitoring either for complications evident at the time of presentation or for observation for complications that may subsequently develop during their course. Criteria for admission to an ICU have been proposed (Table 54.2)1 and include sepsis and septic shock, respiratory compromise or pulmonary infiltrates, those with high risk of brain herniation, moderately impaired and deteriorating level of consciousness, new or evolving neurologic deficits, and presence of seizures. Some authorities feel that all patients with bacterial meningitis may benefit from intensive monitoring early on for presence of new neurologic signs or subtle seizures and for effective control of agitation.15 Patients with generally good outcomes can be defined early in their course on the basis of age, Glasgow Coma Score, APACHE II score, absence of focal neurologic abnormalities, and favorable laboratory features, but these stratification schemes will still fail to identify some patients with more complicated courses.2,16 Table 54.2 Indications for Intensive Care Unit (ICU) Monitoring and Management for Bacterial Meningitis EEG, electroencephalogram; ICP, intracranial pressure. Modified with permission from van de Beek D, de Gans J, Tunkel AR, et al: Community-acquired bacterial meningitis in adults. N Engl J Med 2006;354:44-53. Major complications that occur during the course of bacterial meningitis have been summarized by van de Beek and colleagues1,2,12 and include deteriorating level of consciousness, which may be caused by development of meningoencephalitis (15% to 20% of cases), seizures (15% to 23%), brain edema (6% to 10%), and hydrocephalus (3% to 8%). Mannitol, hyperventilation, repeated lumbar punctures, prophylactic lumbar drainage, prophylactic ventriculostomy, and other modalities have all been proposed for management of increasing intracranial pressure. Increased pressure is associated with worse prognosis, but no single approach for treatment has been confirmed to be effective in all cases.1,17 Patients with severely increased pressure with impending herniation may require ventriculostomy with continuous CSF pressure monitoring. All patients should be monitored for seizures including nonfocal seizures that may only manifest as worsening level of consciousness, but routine use of prophylactic antiepileptic medication is not currently recommended.1,5 Focal neurologic deficits early in the course of meningitis are most often caused by cerebrovascular complications or arteritis secondary to inflammation or less commonly to venous infarcts. The most common late neurologic complication is hearing loss, described in up to 20% of patients overall and in up to 34% of those with pneumococcal meningitis.1,2 The incidence of hearing loss may be decreased in dexamethasone-treated patients.13 Subdural empyema, brain abscess, and hemorrhage are all rare but potentially catastrophic complications of bacterial meningitis. Repeat lumbar punctures are no longer routinely performed in patients with bacterial meningitis who are improving but are indicated in patients with worsening or suboptimal clinical response at 48 hours.5 Repeat CSF analysis is also indicated in patients with more resistant organisms such as highly cephalosporin-resistant S. pneumoniae, especially when treated with dexamethasone, because steroids may decrease antibiotic penetration into the CSF and delay sterilization.18 Repeat imaging by MRI or enhanced CT scan should be performed in patients with clinical deterioration or persistent decreased level of consciousness to assess for the complications listed earlier. Overall mortality rates for bacterial meningitis are reported to be approximately 20% but vary by organism, and an additional 14% will have moderate or major neurologic sequelae.1 Prognosis for meningococcal meningitis is better than for pneumococcal infection. Late neuropsychiatric cognitive effects are seen in up to 10% of cases of bacterial meningitis. The other major CNS infectious syndrome besides bacterial meningitis that may present with fever, headache, altered sensorium, and meningeal signs is acute encephalitis, which is most commonly viral. Although there is significant overlap between clinical presentations of patients with bacterial meningitis and viral encephalitis, the presentation of viral encephalitis is dominated by evidence of parenchymal brain dysfunction including moderate to severely impaired sensorium, delirium, psychosis, focal neurologic findings, and seizures.19,20 The presence of meningismus is more variable, but most patients will have some evidence of meningeal enhancement on imaging and inflammatory cells in CSF. A large number of viruses can cause encephalitis, but management strategies focus on the most common causes and those most likely to respond to specific interventions, particularly encephalitis caused by herpes simplex virus (HSV).19–22 Other important causes with worldwide distribution include other herpesviruses including varicella-zoster virus; Epstein-Barr virus; and cytomegalovirus (CMV), especially in immunocompromised patients.19,20,21 Influenza virus, mumps, measles, and enteroviruses such as enterovirus 71 are also important causes of acute viral encephalitis worldwide. Acute HIV infection can also occasionally present as a potentially treatable cause of fulminant meningoencephalitis.21 Acute presentations of progressive multifocal leukoencephaly caused by JC virus are also increasingly reported in HIV-infected and other immunocompromised patients.23 In addition to those viruses seen worldwide, there are a variety of vector-borne viruses with regional and seasonal distributions.19,21 Important pathogens include eastern, western, and Venezuelan equine encephalitides; Japanese B encephalitis; St. Louis encephalitis; La Crosse encephalitis; and Nipah encephalomyelitis. Recently, West Nile encephalitis emerged as a major pathogen in the United States. West Nile first appeared in New York City in 1999, but cases are now distributed throughout the country, demonstrating the potentially unpredictable and dramatic spread of emerging vector-borne pathogens.24,25 Rabies, although extremely rare in developed countries, also needs to be considered in the differential diagnosis of fulminant encephalitis, both for its epidemiologic implications and because of recent reports of survival for patients with this previously universally fatal infection with aggressive ICU management protocols.26 In addition to viral infections, many atypical bacteria, fungi, and protozoal organisms can present as acute meningoencephalitis.19 Particularly important to consider early in the differential diagnosis are infections that may respond to specific antimicrobial therapy including rickettsial diseases such as Rocky Mountain spotted fever (RMSF) and meningoencephalitis from spirochetal infections including neurosyphilis and Lyme disease.27,28 Important clues to these diseases include epidemiologic history and associated clinical features such as rash. Data from the California Encephalitis Project, in which cases of suspected infectious encephalitis underwent an aggressive evaluation for a variety of infectious agents, suggest that the cause of at least 50% to 60% of cases of presumed infectious encephalitis remains undefined, and in 10% a noninfectious diagnosis was ultimately established.29 Herpes simplex encephalitis is the most common sporadic cause of serious viral meningoencephalitis, causing 3% to 10% of cases of infectious encephalitis in adults and with an estimated frequency of about 1000 to 2000 cases per year in the United States.21,22,29 Ninety percent of cases are caused by HSV type 1, usually occurring in adults as reactivation disease and not primary infection; HSV type 2 commonly causes aseptic meningitis but much less commonly presents as fulminant encephalitis.22,30 Herpes encephalitis is an acute necrotizing process, typically causing hemorrhagic necrosis with particular predilection for the frontotemporal lobes and cingulated gyrus. Mortality rates are up to 70% in untreated cases, with 95% of those surviving having serious neurologic sequelae.21,22 Cases of herpes encephalitis beyond the neonatal period occur throughout life, but the highest case rates occur in younger individuals (younger than 20 years old) and in adults older than age 50 (half of cases). Presentation may include a prodromal viral syndrome in 50% of cases, followed by a generally rapid onset of headache, confusion, and altered level of consciousness. Meningismus, focal neurologic findings, and seizures are also common.20–22 In one series of patients with encephalitis, of which 37% were caused by HSV, focal CNS disease was much more likely than diffuse CNS disease to be caused by HSV.31 The approach to cases of suspected herpes encephalitis, as well as other viral or unknown encephalitides, includes early initiation of antiviral therapy and concurrent rapid clinical evaluation that includes imaging, CSF studies, and electroencephalogram (EEG) to establish a diagnosis.19,20,22 MRI is considered the imaging modality of choice. MRI is positive in more than 90% of cases, often showing changes of edema and necrosis in the medial temporal lobes, insular cortex, and cingulate gyrus as soon as 2 to 3 days into the illness.32 EEGs will be abnormal in nearly all cases, but early findings may be nonspecific and the characteristic periodic lateralizing epileptiform discharges may not be seen until later in the course.22 CSF findings include low- to moderate-grade lymphocytic pleocytosis in 85% and elevated protein in 80%; elevated red blood cell count and mildly decreased glucose are common but not universal, and cell counts may be completely normal in 8%.22,30 Likelihood of HSV encephalitis is extremely low with CSF WBC count of fewer than 5 cells/mm3 and protein levels of less than 50 mg/dL.33 The International Herpes Management Forum has issued guidelines for confirmation of the diagnosis and for treatment.22 PCR of CSF for HSV DNA has replaced brain biopsy as the diagnostic method of choice for HSV encephalitis. Based on data from two trials comparing PCR with the gold standard of brain biopsy, sensitivity of PCR was 98% and specificity was 94% for diagnosing HSV encephalitis; the negative predictive value of PCR on CSF obtained more than 72 hours into the course of illness was close to 100% for excluding HSV.22,34,35 PCR has also expanded understanding of the range of clinical presentations of HSV encephalitis including recognition of less severe cases.31 Viral culture has low sensitivity in older children and adults and is not recommended, and CSF and serum antibody studies have little role in the diagnosis.19,22 Treatment should be initiated on the basis of clinical suspicion pending PCR results using high-dose intravenous (IV) acyclovir at doses of 10 mg/kg every 8 hours and continued for 14 to 21 days, or until PCR results are available or an alternative diagnosis is established. Extrapolating from results in neonates, a positive CSF PCR for HSV at the end of treatment may be an indication to prolong therapy, especially if clinical response has been suboptimal.19 In the 12 years since it first appeared in the Western hemisphere, West Nile virus (WNV) has become a major infectious cause of invasive neurologic disease throughout the United States, with more than 1000 cases from 40 states reported in 2010.24,36 WNV is a mosquito-borne arbovirus affecting birds, mammals, and humans. Of human cases, 80% are asymptomatic and most of the remainder have West Nile fever, but 1% will develop neuroinvasive disease manifesting as meningitis, encephalitis, or a polio-like flaccid paralysis syndrome.24,25 Risk of encephalitis increases with age or with immunosuppression, particularly organ transplantation, and manifestations can range from mild disorientation to coma and death.24 Parkinson-like tremors are also commonly reported. The flaccid paralysis syndrome, caused by viral infection of anterior horn cells, may have abrupt onset and patients may require prolonged ventilatory support. The fatality rate is 9% for WNV neuroinvasive syndromes, and survivors may have prolonged symptoms. In some patients, flaccid paralysis has not resolved after 1 to 2 years.24 CSF findings of WNV are similar to those of other viral infections with lymphocytic pleocytosis predominating. Neuroimaging may be normal, but some scans may demonstrate abnormal signal in the basal ganglia, thalamus, and other deep brain structures or abnormal signal in anterior horn cells of the spinal cord.25,37 Diagnosis is confirmed by the finding of WNV-specific IgM antibodies in CSF and serum or by nucleic acid–based PCR of CSF, serum, or other fluids.19,24 Treatment is primarily supportive; multiple interventions including ribavirin, interferon (INF)-α, immunoglobulin, and other agents have been reported in individual cases and case series, but there are currently no good outcome data to support the use of any specific therapy. Brain abscesses are focal infections of brain parenchyma, occurring from direct spread from local, contiguous infection (ear, sinuses, mastoid, bacterial meningitis); from hematogenous spread of infecting organisms from distant sites; or by direct inoculation from trauma or surgery.38,39 Modern imaging modalities have improved the initial management and follow-up care of patients with brain abscess, but it is less certain that this has significantly affected overall outcome. Presenting symptoms may be indistinguishable from those of other CNS infections, with fever, headache, and focal neurologic findings predominating.38–40 Seizures and decreased level of consciousness are also seen. Sepsis was noted in 18% of cases in one recent series.41 Duration of symptoms prior to presentation is typically much longer than that of bacterial meningitis or viral encephalitis. Microbiology reflects the source of the original infection and most commonly includes streptococci, staphylococci, oral anaerobes, and enteric gram-negative organisms, but multiple other bacterial, fungal, tuberculous, and atypical organisms can also be found.38–40 In areas of high HIV prevalence, opportunistic brain infections, especially toxoplasmosis, have become more prevalent than typical pyogenic abscesses, and knowledge of HIV status is crucial to initial management of suspected infectious mass lesions.42 The diagnosis of brain abscess is suggested by the clinical presentation and imaging findings by either CT or MRI showing enhancing parenchymal lesions, usually with surrounding inflammatory changes.38,39 Radiographic appearance may be indistinguishable from a malignant lesion. Management of suspected abscess includes either stereotactic aspiration or surgical drainage to both establish a microbiologic diagnosis and for primary treatment of the abscess. Smaller lesions (<1 cm) can be treated with antibiotics alone, but larger lesions will require either aspiration or open drainage.38,39 Recent studies have confirmed earlier findings that aspiration may result in lower mortality rates and less residual neurologic deficit than surgical resection.43 Duration of treatment is until resolution of the abscess on serial imaging studies. Unlike bacterial brain abscesses, toxoplasmosis lesions in patients with AIDS are usually multiple and may respond to empiric toxoplasmosis therapy without need for further invasive diagnostic procedures.42 Spinal epidural infections most commonly arise by contiguous spread of infection into the spinal canal as a complication of vertebral infections or, less commonly, as a complication of epidural procedures such as epidural injections or epidural catheterization.44–46 Vertebral infections result from hematogenous infection of vertebral bodies or disk space or by direct introduction of organisms from surgery or trauma. In addition to affecting the vertebral bodies and intervertebral disk spaces, vertebral osteomyelitis may expand into surrounding paravertebral soft tissues and spinal canal and even rarely into the medullary spinal cord. Paravertebral and epidural infections can rapidly progress, resulting in severe neurologic symptoms from compression of nerve roots or the spinal cord, or by infarction of the spinal cord from inflammation and vasculitis of vertebral arteries.45,47 Thus an aggressive diagnostic and therapeutic approach is necessary to prevent catastrophic consequences such as irreversible paraplegia and death. The incidence of spinal epidural infection from large retrospective reviews is reported as approximately 0.2 to 2 cases per 10,000 hospital admissions, but the frequency of this diagnosis may be increasing, perhaps because of improvements in radiographic diagnosis and increasing prevalence of risk factors.45 Incidence in adults increases with age older than 30 years; important predisposing factors include diabetes, injection drug use, alcoholism, immunosuppression, underlying spinal disorders, trauma, invasive procedures, and extraspinal sites of infection that cause significant bacteremia.45,46 Infections can occur at any level of the spinal cord, although most series report predominance of lumbar involvement. Approximately two thirds of infections are caused by Staphylococcus aureus including methicillin-resistant S. aureus (MRSA) with a variety of other gram-positive organisms (coagulase-negative staphylococci, viridans streptococci, β-hemolytic streptococci), as well as gram-negative organisms all reported in lesser numbers.44–46 Granulomatous infections including tuberculosis and brucellosis remain major causes of vertebral and epidural infection in many areas of the world.47 Approximately 10% of episodes are culture-negative.45 Presenting symptoms are extremely nonspecific and include back pain in more than 95% of cases and fever in two thirds of cases.44,45 Thirty percent of cases will present with evidence of early neurologic deficits such as muscle weakness, incontinence, or sensory deficits, and up to one third will have evidence of some paralysis on examination.44–46 Associated laboratory features include leukocytosis in two thirds of cases and elevated erythrocyte sedimentation rate (ESR) in nearly all cases. The most sensitive imaging modality is MRI with gadolinium, with reported sensitivity of greater than 95%, but most infections were also visualized on CT and unenhanced MRI.44,45 Standard therapy previously included emergent surgical drainage of the abscess and systemic antibiotic therapy. However, over the past 2 decades there has been an emerging literature on more conservative medical management employing percutaneous aspiration and antibiotics without open surgical drainage.44–46 These reports have suggested that outcomes are similar or better (i.e., less neurologic sequelae) compared to surgery.44 No trials have directly compared treatment modalities, and retrospective analyses have not identified risk factors for worse outcomes with medical therapy alone. Indications for surgery include neurologic progression on treatment or lack of clinical response, thus those managed without surgery require careful monitoring.44,45 Surgery may also be the preferred treatment for those with more severe neurologic deficits on initial presentation, though these patients have worse outcomes overall regardless of treatment modality.44,45 Several large case series published since 2005 have addressed changes in the epidemiology of bacterial endocarditis over the past 2 decades.48,49 The annual incidence of endocarditis of 5 to 7 cases per 100,000 has not changed significantly over time.48 However, the International Collaboration on Endocarditis Prospective Cohort Study, a multicenter study of 1779 cases from 39 medical centers in 16 countries, has illustrated the recent changes in microbiology and clinical presentation of bacterial endocarditis.49 In this cohort, as well as other recent cohorts, S. aureus rather than viridans streptococci were the predominant pathogens and increasing numbers of cases were considered either nosocomially acquired or health care associated.49 S. aureus endocarditis is associated with a significantly higher mortality rate, higher rate of stroke and other systemic embolization, and higher rate of sustained bacteremia than endocarditis caused by other organisms.49–51 The increased antibiotic resistance in organisms causing endocarditis, especially the increasing rates of MRSA, are reflected in the recent guidelines for diagnosis, treatment, and management of complications of endocarditis from the American Heart Association.50 Other important recent epidemiologic trends are the decreased importance of congenital valvular and rheumatic disease as predispositions, the increasing age of cases, and the increased role of hemodialysis and indwelling cardiac devices such as pacemakers and implantable defibrillators as risk factors.49–52 Infectious endocarditis must be considered in the differential diagnosis of a broad range of clinical syndromes. Fever is the single most common presenting symptom, often accompanied by other constitutional symptoms of anorexia, weight loss, and fatigue. Onset may be acute or subacute with tendency toward more acute presentations with S. aureus infections. Signs and symptoms may be consequences of direct cardiac effects of infection including new or changing heart murmur, worsening congestive heart failure and valvular dysfunction, or onset of heart block from myocardial abscesses.50 The clinical presentation may also be dominated by systemic manifestations of emboli or immune complex disease including such findings as skin lesions, splenomegaly, glomerulonephritis, cerebrovascular events, and other acute vascular embolic events. Patients with acute, fulminant endocarditis, particularly S. aureus endocarditis, may present with concurrent cardiogenic and septic shock. Clinical criteria have been developed and prospectively evaluated for the diagnosis of infective endocarditis.53,54 The most current version of these, the Modified Duke Criteria for Diagnosis of Infective Endocarditis (Box 54.1), relies primarily on blood culture data and echocardiographic findings as the two major clinical criteria for diagnosis; additional minor clinical criteria (fever, underlying predisposition, embolic phenomena, immunologic phenomena) can also be used as supporting evidence for determining confirmed or suspected cases.54 Patients with endocarditis have sustained bacteremia; in the absence of prior antibiotic therapy the yield of at least one positive blood culture after three sets are drawn is greater than 90%, and typically multiple cultures are positive. Thus two to three separate sets of blood culture should always be obtained in suspected endocarditis prior to initiation of therapy. Culture-negative cases may be attributed to prior antimicrobial therapy or to infection caused by fastidious or difficult-to-cultivate organisms.50 Follow-up blood cultures are critical to document sterilization of blood and should be repeated frequently until negative. Echocardiography should be performed on all patients with suspected endocarditis.50,52 When possible, transesophageal echocardiography (TEE) is the preferred modality in adults. Sensitivity of TEE is reported to be as high as 95% for native valve infection compared with 60% to 75% for transthoracic echocardiography (TTE) and is significantly better than TTE for diagnosis of prosthetic valve infection and for detection of complications such as perivalvular abscess that may affect management.50 In children and uncomplicated adult cases, in which TTE is diagnostic, TEE may not be necessary. If initial studies are negative, TEE should be repeated in 7 to 10 days if clinical suspicion remains high.50 Embolic complications may occur at any time during the course of infective endocarditis with overall incidence of 20% to 50%; risk decreases but still remains significant after initiation of antimicrobial therapy, especially with larger vegetations, and remains high for up to 2 to 3 weeks.50,55,56 Risks for embolization include specific organisms, especially S. aureus, Candida, HACEK* organisms, and Abiotrophia; increased vegetation size (>10 mm) and mobility as determined by echocardiography; mitral versus aortic valve involvement; and anterior versus posterior location on the mitral valve.50 More than half of clinically manifesting emboli involve the CNS, most commonly in the middle cerebral artery distribution.50,55 In addition to emboli, other risks for a fatal outcome include congestive heart failure, abnormal mental status, comorbid conditions, higher APACHE score, and S. aureus infection.49–51 Congestive heart failure appears to have the highest association with death.49–51 Medical therapy (versus surgical therapy) was also associated with higher 6-month mortality rates in recent studies.51,52 The decision to perform emergent or urgent valvular surgery on patients with active endocarditis remains complex. Indications for surgery can be broadly classified into those related to management of heart failure, management of uncontrolled infection, and management of embolization, and decisions are also impacted by patient status and available surgical expertise. Traditional indications for surgery include refractory congestive heart failure; persistent infection despite optimal antimicrobial therapy; fungal or other difficult-to-treat organisms; one or more emboli during the first weeks of antimicrobial therapy; and valvular complications of dehiscence, perforation, fistula, and large perivalvular abscesses (Table 54.3).50 Vegetation size and location are also emerging as possible independent indications for surgery.50 The risk of infecting a new prosthetic valve during surgery for active endocarditis is only 2% to 3%; thus active infection is not a contraindication to surgery that is indicated for complications associated with high mortality rate.50 Reviews of recent studies have confirmed the decreased mortality rates of cohorts of patients who were managed with early surgical intervention, especially those with left-sided S. aureus endocarditis, though there are no randomized controlled trials completed that address this.50,52 The optimal surgical procedure and the role of more conservative procedures such as vegetation resection remain incompletely defined, though resection of vegetations is frequently done in isolated, refractory right-sided endocarditis. The majority of patients who survive an episode of left-sided endocarditis who are not operated on initially will ultimately require valve replacement within the next 15 years.50 Table 54.3 Possible Indications for Emergent or Urgent Surgical Intervention for Acute Infective Endocarditis TEE, transesophageal echocardiography.
Specific Infections with Critical Care Implications
Overwhelming Infections of the Central Nervous System
Acute Bacterial Meningitis
Epidemiology, Pathogenesis, Risk Factors, and Clinical Presentation
Diagnostic Strategies and Early Management of Suspected Bacterial Meningitis
Complications, ICU Monitoring, and Prognosis
Indication
ICU Management
Sepsis and shock
Hemodynamic support and monitoring, early goal-directed therapy
Pulmonary infiltrates or respiratory compromise
Airway management, monitoring of oxygenation, non-invasive or invasive ventilatory support
Glasgow Coma Scale score <10
Monitoring of examination; monitor for development of increased ICP, hydrocephalus, and seizures
Deteriorating level of consciousness
Monitoring of examination; monitor for development of increased ICP, hydrocephalus, and seizures
New or evolving neurologic deficits
Monitoring of examination; monitor for development of increased ICP, hydrocephalus, and seizures
Evidence of increased ICP
Consider intracranial pressure monitoring; osmotic diuretics
Acute hydrocephalus
Repeated lumbar puncture, lumbar drain, or ventriculostomy
Seizures
Continuous EEG monitoring, antiepileptic agents
Severe agitation
Careful sedation
Hyperglycemia
Maintain normoglycemic state with insulin therapy
Hyperpyrexia
Cooling modalities for fever >40° C
Encephalitis
West Nile Virus Encephalitis
Brain Abscess
Spinal Epidural Abscess
Fulminant Endovascular Infections
Acute Infective Endocarditis
Indication
Details/Comments
Clinical Indications
Refractory congestive heart failure
Most common single indication for surgery
Severe valvular decompensation
Usually acute mitral or aortic insufficiency but also valve obstruction. Less commonly, severe tricuspid regurgitation
Emboli and recurrent emboli
Especially with 1 or more events occurring during first 1 to 2 weeks of antimicrobial therapy
Persistent infection/sepsis
Persistent positive blood cultures after 7 days of optimal antibiotic treatment and no other source
Difficult-to-eradicate organisms
Fungal endocarditis, highly resistant bacteria; staphylococcal or gram-negative prosthetic valve endocarditis (controversial)
Extension of infection into myocardium
Evidence of new heart block, echocardiographic findings as listed below
Echocardiographic Indications
Evidence of valve decompensation
Dehiscence, rupture, perforation, fistula, perivalvular abscess
Vegetation characteristics
>10 mm in size, especially on anterior mitral valve and emboli; increase in size despite treatment; >15 mm in size on aortic, mitral, or prosthetic valve; >20 mm in size on tricuspid valve
Other Possible Indications
Complicated prosthetic valve infection
As defined by TEE findings; high failure rate for medical therapy alone
?Any left-sided Staphylococcus aureus infection
Early surgical management may be associated with lower mortality
Related posts:

Full access? Get Clinical Tree


Specific Infections with Critical Care Implications