Chapter 34 Soft tissue infection present as the primary cause requiring critical care but also can be present as a complication after injury, surgical procedures or other interventions. These infections can involve the skin, subcutaneous tissue and can extend to other tissues with extension into adjacent tissue planes. The spectrum of patients presenting with infection as the primary cause covers a broad area of different types of presentation and severity. The most severe is necrotizing soft tissue infection (NSTI) a rapidly progressive infection that may affect the skin, subcutaneous tissue and muscle with necrosis. Associated systemic sepsis may require critical care. In this chapter, the etiology, pathophysiology of these infections as well as principles of management are presented to guide the intensivist in understanding, diagnosing and participating in the care of these patients in conjunction with the soft tissue specialist surgeon and infectious disease expert as part of the care team. Soft tissue infection is common and a non-life threatening form may be seen in patients in the critical care setting. Any break in the skin barrier offers the portal of entry for bacteria. Surgical procedures are associated with a 5% infection complication rate. However, many are localized and will be managed in a non-critical care setting following the principles of antibiotics, drainage and immobilization. Similarly, other form of infection such as those following trauma will be managed using the same principles. A variety of factors contribute to the incidence such as the type of trauma, the severity, contamination, age and patient associated risk factors. Some of these patients will be in a critical care setting related to their initial trauma when the infection develops. Guidelines are present to help the management of different types of trauma, emphasizing the surgical management and to help minimize the development of infection as well as to facilitate treatment of different types. Procedures to drain collections are very important and should be performed as soon as the collections are identified. More invasive infection, implying the development of systemic signs such as fever and chills are previously would be admitted to hospital. Many of these patients are now managed with appropriate drainage, initial wound management in an ambulatory setting and subsequently with intravenous antibiotics and appropriate wound management in a home care setting. Severe infection, however, implying additional systemic findings such as tachycardia, persistent elevated temperature, and confusion and associated laboratory abnormalities requiring critical care support is less common. The most alarming is a severe primary form of NSTI. There are about 1,000 cases per year in the United States. The mortality rate can be as high as 25% and the outcome is related to the timing of diagnosis and intervention.1 When soft tissue infection is associated with generalized organ failure, as in NSTF, mortality rate is as high as 70%. It is generally agreed that bacterial invasion of the subcutaneous tissues occurs either through external trauma or direct spread from a perforated viscus (most commonly colon or rectum) or urogenital organ. Bacteria then spread through subcutaneous planes producing endo- and exotoxins that cause tissue ischemia, liquefactive necrosis, and often systemic illness.3–4 Skin necrosis is secondary to vascular occlusion and because of the rich collateral vascular networks within the skin, the overlying skin changes usually does not reflect the magnitude of the underlying tissue necrosis.3 In addition, superficial nerves in the subcutaneous planes can be affected by the ischemic changes, which eventually lead to decrease sensation in the area. Infection can spread as fast as 1 inch per hour depending on the virulence of the bacteria and the host immunity.18 A variety of risk factors are associated with NSTF and these are listed in Table 1. Table 1. Risk factors for soft tissue infection.
Soft Tissue Infection in Critical Care
Sami Alissa, Nawaf Al-Otaibi and James Mahoney
Overview
Incidence
Pathophysiology
| Host factors | Wound factors |
Alcohol abuse | Blunt or penetrating injury |
Peripheral vascular disease | Devitalized tissue |
Liver disease | Foreign body |
Renal calculi or failure | Inadequate debridement |
Incarcerated hernias | Gross contamination |
Odontogenic infection strep throat | Compound fractures |
Drug abuser | Burns |
Old age | |
Obesity | |
Smoking | |
Immunocompromised states, such as diabetes mellitus, and malignancy |
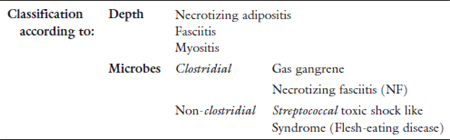
Table 2. Classification of soft tissue infection.
Note: Modified from Sarani.3
Classification
NSTI can be classified according to depth of tissue involvement, anatomical area involved, or microbiology. The most popular classification is the one based on microbes. These are summarized in Table 2.
Clostridial Infections (Gas gangrene): These are caused by Clostridial species, which are gram positive, spore forming, and anaerobic bacteria. These bacteria are found in the human body as gastrointestinal flora (C. septicum) and in the soil (C. perfringens). Severe soft tissue infection associated with clostridia is associated with three clinical scenarios. The most common scenario is direct contamination of a traumatic wound. Other presentations can involve postoperative wound infection especially gastrointestinal and biliary surgery as well as a secondary infection, in the setting of colonic malignancies. The incubation period varies from hours to days with death reported as early as 12 hours following the development of clinical infection. It can have a fulminant rapidly progressive course of infection with spread of infection and necrosis as fast as 1 inch/hour. The common and important isolated organism is C. perfringens, which is known for its lethal exotoxins. It produces an Alpha toxin; a lecithinase which destroys cell membranes: Theta toxin; a hemolysin also a cardiotoxin: Kappa toxin; a collagenase: Mu toxin; a hyaluronidase which facilitates spread as well as Nu toxin a deoxyribonuclease. The classic presentation is severe pain disproportionate to physical findings often early within several days of the traumatic event, followed by edema and bronze skin discoloration. Hemorrhagic skin blebs associated with dermal necrosis, a brawny foul smelling seropurulent discharge can be seen. Early systemic signs include low-grade fever, tachycardia, fever, CNS findings (usually lethargy and indifference), with rapid progression to cardiovascular collapse and multi-organ failure. Palpable wound crepitus may not present till late (if at all). When associated with traumatic injury, examination of all wounds whether traumatic or associated with surgical findings is very important, as these are usually the portals of entry for the infection.
Non-clostridial infections are classified into two groups, polymicrobial infection and monomicrobial infections (one organism) and are characterized in Table 3. Polymicrobial infections are more common and frequently aerobic and anaerobic organisms are cultured in the same wound. Polymicrobial infection usually develops more slowly, usually over days. The perineum, lower extremity (foot infections in diabetes) as well as postoperative wound sites are seen with this type of infection. Crepitus on palpation and gas in soft tissue on X-ray can be seen due to the presence of gas producing bacteria.
Monomicrobial infection has created considerable controversy with its diagnosis and treatment due to the rapidly progressive (<24 hours) presentation of a previously well person to someone with a life threatening infection in intensive care. They often require mutilating surgery and are at risk of limb loss. The usual organism associated with these severe infections is Group-A beta hemolytic streptococcus. However, in our experience Staphylococcus aureus and methicillin resistant Staphylococcus aureus (MRSA) infection can also present in a similar fashion. There may be a history of trauma to the area: However, this is not always present. The infection starts superficially and preferentially involves the deep fascia and in this plane can rapidly spread. Toxins produced by streptococcus bacteria include a hyaluronidase, which facilitates spread as well as exotoxins creating systemic toxicity. Infection with streptococcus has a unique virulent characteristic related to the bacterial surface proteins, M-1 and M-3. These M proteins help the bacteria to escape phagocytosis by neutrophils by increasing bacterial adherence to body tissues. In addition, streptococcal and staphylococcal exotoxins A and B damage the endothelium and cause loss of microvascular integrity resulting in tissue edema and impaired blood flow at the capillary level.3 Together M-proteins and some exotoxins exhibit “superantigen activity” which is responsible for a massive pro-inflammatory cytokine release, 2 to 3 orders of magnitude greater than that seen with an ordinary antigen which helps explain the overwhelming inflammatory response, septic shock and multiorgan failure seen in Streptococcal infection. There is clinical variation in the presentation with some patients demonstrating less in the way of systemic findings with significant local infection whereas others present early with life threatening findings (Streptococcal toxic shock syndrome). The Infection associated with Vibrio is related to marine exposure and although very serious, are less common.19
Table 3. Non-clostridial NSTI (Necrotizing Fasciitis or NF).
| Organism | Characteristic | |
| Type I | Polymicrobial | • Most common type of NTSI and responsible up to 75% or more of infections. Related posts:
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|




