Glen P. Greenough, Brooke G. Judd
Sleep Disorders
Sleep disorders are associated with major functional impairments, including loss of productivity, work-related and vehicular accidents, social impairment, and cognitive and mood disturbances, as well as morbidity and mortality as a result of cardiovascular, endocrine, and immune disturbances. Given the significance of these disorders, it is incumbent on primary care providers to recognize the symptoms of sleep disorders, to make accurate diagnoses, to initiate sound referrals, and to develop successful treatment plans in collaboration with sleep medicine specialists.
In this chapter, an overview of normal sleep is presented along with a description of the most common disorders of sleep. The most recent edition of the International Classification of Sleep Disorders1 (ICSD) organizes the conditions into seven major categories: insomnias, sleep-related breathing disorders, central disorders of hypersomnolence (excessive sleepiness not related to other sleep disorders), circadian rhythm sleep-wake disorders, sleep-related movement disorders, parasomnias (abnormal behaviors or events arising from sleep), and other sleep disorders. These categories, which are largely symptom based (e.g., insomnia or hypersomnias), serve as a guide to obtaining a detailed history and initiating essential diagnostic procedures.
From a practical standpoint, fundamental assessment of sleep, which should be part of any complete patient history, can begin with three basic questions: How are you sleeping at night? Are you excessively sleepy during the daytime? Are there any unusual events or problems with your sleep, especially heavy snoring? More detailed aspects of assessment are included in individual sections within this chapter.
Normal Sleep
Definition and Physiology
Sleep is an active, dynamic physiologic process. Normal human sleep consists of two major states of consciousness: non–rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep. NREM sleep is further divided into three stages from lightest (N1) to deepest (N3, also referred to as slow-wave or delta sleep). These stages unfold in a predictable, repeated cycle. In young adults, NREM sleep occupies about 75% of the night and REM the remaining 25%. Delta sleep is most prominent in young children and gradually diminishes through the life cycle. REM sleep (or its ontogenetic precursor) is seen in very high percentages in neonates and infants but diminishes rapidly in the first years of life and remains fixed at about 25% thereafter. Normal total sleep time varies considerably with age.2 Although young children require longer sleep times, total sleep time begins to decline by the second decade, remains relatively stable from the third decade through the fifth decade, and falls off more dramatically after the age of 70 years. It remains unclear to what extent the decline in nocturnal sleep in older individuals is a function of diminished sleep need as opposed to decreased ability to sleep. Time to fall asleep (sleep latency) and wake time after sleep onset are increased in older adults, as is daytime napping, although much of this may be related to factors that often accompany aging as opposed to the aging process itself.
NREM sleep is associated with a decline in respirations, heart rate, and blood pressure; muscle relaxation; and diminished cognitive activity. Sleep starts (sudden muscle contractions involving part or all of the body) may occur during wake-sleep transitions. REM sleep is marked by pronounced changes in physiology, including skeletal muscle atonia; increased variability in heart rate, blood pressure, respiration, and autonomic function; REM; and heightened cognitive activity associated with dreaming. Ventilatory drive to hypoxia and hypercapnia is decreased during NREM sleep and reaches its lowest point in REM sleep.
Current theories of sleep regulation focus on the two-process model.3 This model suggests that sleep is regulated by two factors: homeostatic sleep drive, which increases progressively during wake time; and circadian wake drive, which is based on the oscillating 24-hour rhythm of the major circadian clock, located in the suprachiasmatic nucleus of the hypothalamus. Thus, the timing and amount of sleep are influenced by complex interactions between the biologic rhythms and the length of time since the last sleep period. Average human circadian cycles naturally run slightly longer than 24 hours (about 24.2 hours) but are reset daily (entrained) to a 24-hour rhythm by a variety of environmental cues, the most important of which is exposure to light. Sleep-wake rhythms are normally synchronized with myriad other clock-regulated physiologic functions, including endocrine-metabolic, immune, and cardiovascular.
Insomnia and Nonrestorative Sleep
Definition and Epidemiology
Current epidemiologic data indicate that about 30% to 35% of individuals in Western society report at least occasional insomnia.4 Multiple studies place the prevalence of chronic insomnia at about 10%.4 Insomnia is a complex condition that may represent a final common pathway with numerous contributing factors. Acute or transient insomnia (days to a few weeks) is an almost universal problem that is typically related to an acute stress or time zone shift (i.e., jet lag) and is usually self-resolving. Good sleep hygiene and, for some patients, short-term sleep medications are usually adequate. A potential complication of short-term insomnia is that some patients will begin to exhibit cognitions and behaviors that establish a foundation for development of a chronic insomnia problem.
Pathophysiology
A widely accepted model of chronic insomnia suggests that it is a function of predisposing, precipitating, and perpetuating factors. Little is known about predisposing biologic or psychological factors, although it does seem clear that certain persons are at greater risk than others for the development of a chronic insomnia problem. Precipitating factors (which are sometimes referred to as causes of chronic insomnia) are identified in Box 227-1 and are discussed in greater detail later.
A unifying concept in the pathophysiology of chronic insomnia is that of hyperarousal.5 Data indicate that patients with this condition exhibit evidence of both physiologic and cognitive hyperarousal, in the form of increased 24-hour metabolic rate, increased temperature, muscle tension, sleep electroencephalogram frequency, overactivity of the hypothalamic-pituitary-adrenal axis, and cognitive activity. It remains unclear how this hyperarousal develops, although preliminary data suggest that it is, at least in part, acquired and is amenable to change with therapeutic interventions such as cognitive behavioral treatment.
Clinical Presentation
Psychiatric disorders, especially major depression, are the most common precipitating factors. Generalized anxiety, panic, and post-traumatic stress disorders are also associated with elevated rates of insomnia. Substance abuse or dependence, including alcohol, sedative-hypnotics, stimulants, and opiates, frequently manifests with insomnia, which may persist even after discontinuation of the substance. Excessive use of caffeine or even moderate use later in the day may also be problematic.
Circadian disorders, especially shift work and delayed sleep-wake phase disorder, are commonly associated with sleep complaints. Significant percentages of night shift workers experience abnormal sleep, with reduced total sleep times and poor quality of sleep. This pattern does not tend to improve during long periods of night work for most shift workers. As a result of circadian misalignment and sleep disturbances, shift workers are at increased risk for a number of medical disorders (ulcer disease, breast cancer among female shift workers, and cardiovascular disease) as well as accidents. Delayed sleep-wake phase disorder occurs most commonly in adolescents and younger adults and is characterized by an inability to sleep at normal clock times, with normal sleep onset occurring late (e.g., 4 AM), and subsequent inability to arise at conventional times (e.g., noon awakening). Sleep is otherwise restorative and normal, but the schedule is clearly inconsistent with meeting of normal school or work times. Advanced sleep-wake phase disorder is a less common circadian rhythm disorder, with normal sleep quantity and quality occurring early in the 24-hour day (e.g., 7 PM to 3 AM). It appears to be most common in older adults.
Medical conditions and medications may contribute to sleep disturbance. Among the most common are those associated with nocturnal pain, chronic lung disease, end-stage organ failure, endocrine disorders and other metabolic conditions, and especially neurodegenerative diseases. Likewise, many medications may aggravate sleep, most notably steroids, methylxanthines, some antihypertensives, stimulants, and certain antidepressant medications.
Other physiologic sleep disorders may result in an insomnia problem. The patient with restless legs syndrome (RLS) reports distressing, “creepy-crawly” sensations in the legs or, less commonly, arms. The sensation is associated with an irresistible urge to move the extremities. The sensations may interfere with sleep onset. RLS is often associated with periodic limb movements (PLMs), which are characterized by repetitive, periodic (every 20 to 40 seconds) limb movements, often resulting in arousals that the sleeper is unaware of (much as in obstructive sleep apnea [OSA]). RLS is discussed in greater detail in the section on movement disorders.
Although OSA is most often associated with complaints of daytime sleepiness rather than with insomnia, these patients may have clinically significant complaints of insomnia. This association may be more prevalent among women with OSA. Therefore OSA must also be considered in the differential diagnosis, particularly in obese patients and those with heavy snoring.
The essential features of chronic insomnia according to the ICSD-3 are frequent and persistent difficulty initiating or maintaining sleep with a daytime consequence. An important subtype of chronic insomnia is psychophysiologic insomnia (PPI), a conditioned arousal in response to efforts to sleep and negative expectations regarding the ability to sleep. Individuals with PPI may be able to sleep better when they are not trying to fall asleep or in settings other than their own bedroom. Symptoms may include difficulty getting to sleep as well as trouble returning to sleep after awakening. This type of insomnia exists commonly as a disorder in its own right. However, the hyperarousal and negative conditioning that occur in this disorder are frequent complicating factors in insomnia that is associated with the numerous precipitating factors described earlier. Often, when an initial precipitating factor (e.g., a major depression, acute stress, or medical illness) resolves, it is these conditioned psychophysiologic elements that serve as the perpetuating factors noted earlier in this chapter.
Diagnostics
The essential element in the evaluation of an insomnia complaint is the history. The nature of the onset, course, complications, and treatments of the condition must be elicited in detail. Sleep-wake schedule, including napping, is critical to assessment. Sleep logs, usually conducted for 1 or 2 weeks, can be a helpful adjunct to history. The log should contain the following information for each night: time of getting into bed, time lights are actually turned out (e.g., after television, reading), estimate of sleep latency (time to fall asleep after lights out), estimate of the number of awakenings and total awake time across the night, time of final awakening, and time of actual arising. Evidence of other sleep-related symptoms (e.g., snoring and observed pauses in breathing, limb movement or restless legs, nightmares, behavioral disturbances, headaches, pain, gastroesophageal reflux) must be sought from the patient and, whenever possible, the bed partner. Daytime consequences, particularly evidence of significant sleepiness, should be assessed. Medical, neurologic, and psychiatric evaluations as well as pertinent physical examination and appropriate laboratory procedures are essential.
Polysomnography (PSG), overnight sleep recording, contributes little to the diagnosis of most insomnia presentations and is usually reserved for those cases in which demonstrable physiologic disturbances are suspected, typically breathing disorders, hypersomnias, and some parasomnias. PSG may also be appropriate for patients with treatment-refractory insomnia.
Management
The management of insomnia begins with careful identification of the contributing factors. Treatment is tailored based on those factors. When clear precipitating causes are present (e.g., major depression or RLS), specific therapies appropriate to those factors must be instituted (e.g., antidepressant medication or dopamine agonists for RLS). Attention must also be directed to substances or medications that may be disturbing sleep. Sleep hygiene education is an essential component for management of any insomnia problem but is typically not sufficient treatment in its own right.
Treatment of circadian rhythm sleep disorders is often complex and in many cases is best administered by sleep medicine specialists. Bright light therapy and melatonin have demonstrated therapeutic benefit in certain patients with sleep-wake schedule disorders. Chronotherapy (planned behavioral adjustments of schedule) involving progressive phase delay has also been used for patients with delayed sleep phase disorder.
3. The benzodiazepine receptor agonists and ramelteon have comparable efficacy and, like the benzodiazepines themselves, differ primarily with respect to the clinical duration of action. Although hypnotic medications have been indicated only for short-term use until recently, emerging data have demonstrated safe and effective long-term use of some benzodiazepine receptor agonists, without dosage escalation or evidence of dependency in controlled settings.6 However, a clear algorithm for long-term use of pharmacologic therapies and the interaction of these therapies with nonpharmacologic approaches has yet to be elucidated.
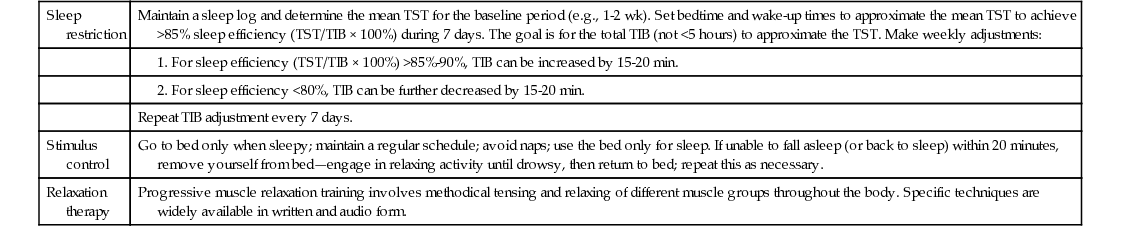
4. Cognitive behavioral therapy for chronic insomnia (CBT-I), particularly PPI, is brief and produces sustained benefit.7 Compared with short-term courses of medication, CBT-I produces durable improvement, whereas improvements seen with time-limited courses of hypnotics tend to dissipate rapidly after drug discontinuation. Behavioral therapies include sleep restriction therapy, stimulus control, and relaxation training (Table 227-1). These therapies are often combined on a case-by-case basis. The common component of the most successful therapeutic approaches is marked reduction of the time spent in bed awake. In addition to the behavioral components, successful CBT regimens also include cognitive restructuring to identify and to alter the distorted cognitions that are often so much a part of the fabric of insomnia.
TABLE 227-1
Common Behavioral Therapies for Chronic Insomnia
| Sleep restriction | Maintain a sleep log and determine the mean TST for the baseline period (e.g., 1-2 wk). Set bedtime and wake-up times to approximate the mean TST to achieve >85% sleep efficiency (TST/TIB × 100%) during 7 days. The goal is for the total TIB (not <5 hours) to approximate the TST. Make weekly adjustments: |
1. For sleep efficiency (TST/TIB × 100%) >85%-90%, TIB can be increased by 15-20 min. | |
2. For sleep efficiency <80%, TIB can be further decreased by 15-20 min. | |
| Repeat TIB adjustment every 7 days. | |
| Stimulus control | Go to bed only when sleepy; maintain a regular schedule; avoid naps; use the bed only for sleep. If unable to fall asleep (or back to sleep) within 20 minutes, remove yourself from bed—engage in relaxing activity until drowsy, then return to bed; repeat this as necessary. |
| Relaxation therapy | Progressive muscle relaxation training involves methodical tensing and relaxing of different muscle groups throughout the body. Specific techniques are widely available in written and audio form. |
Life Span Considerations
Advanced sleep phase syndrome, which may lead to sleep maintenance issues, is most common in older adult populations.
Complications
Insomnia is associated with mood disorder.
Indications for Referral and Hospitalization
Patients with insomnia that is persistent and causing impairment in daytime activities should be referred to a sleep specialist.
Related posts:





Full access? Get Clinical Tree


