Single Thoracic Paravertebral Block
A. Thoracic Paravertebral Block
Anna Uskova
Rita Merman
After negative aspiration, 5 ml of local anesthetic is injected at each level to be blocked.
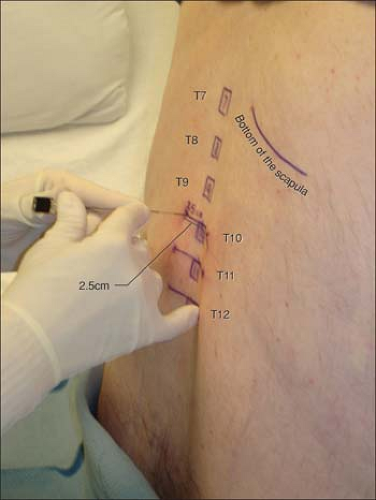 Figure 22-1. The Tuohy needle is placed perpendicular to the skin with bevel up and advanced up to 3 to 5 cm. |
Inferior angles of the scapulae are used to localize the spinous process of T7 vertebra.
Local anesthesia is performed with two passes of the needle: one perpendicular to the skin (the transverse process can be contacted in thinner patients), then pull the needle back, redirect it caudally, and inject more along the pass to the paravertebral space.
Do not deviate from the parasagittal plane to avoid medial spread and neuroaxial block (postdural puncture headache has been reported after a paravertebral block).
If the needle is redirected caudally and contacts the bone at a shallow distance, reinsert the needle 0.5 cm caudally. (First time was too cephalad and found the rib, instead of the transverse process.)
Too much resistance on injection suggests wrong needle position.
It is not uncommon to see hypotension/bradycardia episodes with this technique in sitting position. Safe practice requires minimal monitoring with noninvasive blood pressure cuff and pulse oxymeter, reliable intravenous access, and supplemental oxygen via nasal cannula. Glycopyrrolate 0.2 mg and ephedrine 50 mg should be always available for treatment. After the episode, extended vital signs monitoring and report to room nurse are recommended.Related posts:

Full access? Get Clinical Tree





