CHAPTER 131
Shoulder Dislocation
Presentation
The patient arrives holding one arm with the opposite hand, complaining of severe pain, stating that his “shoulder is out,” unable to move it without increasing the pain. Often, the patient had had the arm lifted horizontally to the side (“quarterback position”) when it was leveraged posteriorly, causing the dislocation. Recurrent dislocations may be the result of relatively minor forces, such as those produced when reaching into the back seat of a car from the driver’s seat or rolling over while asleep.
The deltopectoral groove may show a bulge (caused by the dislocated head of the humerus), and the acromion appears to be prominent laterally, with an emptiness beneath the acromion where the humeral head should be (Figure 131-1).
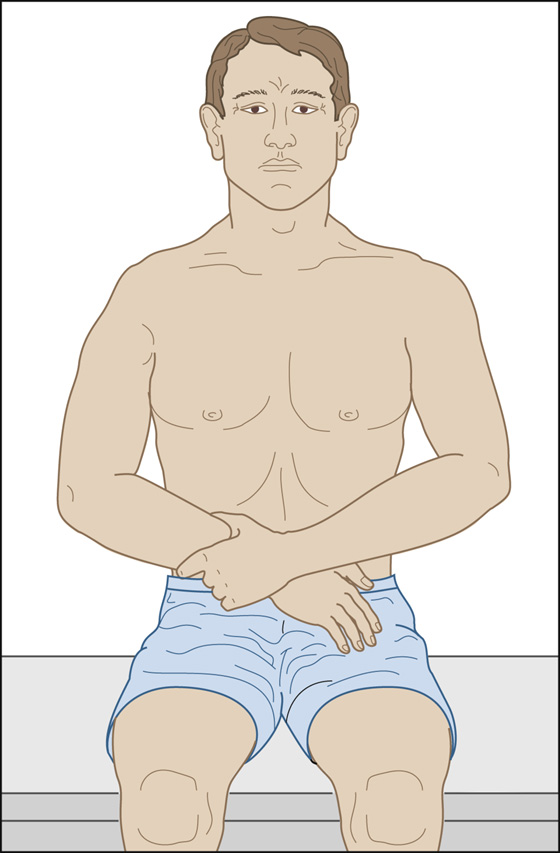
Figure 131-1 Shoulder dislocation with loss of the normal deltoid bulge. (Adapted from Ruiz E, Cicero JJ: Emergency management of skeletal injuries. St Louis, 1995, Mosby.)
Ninety percent of shoulder dislocations are anterior, as just described. Most of the others are posterior and are usually caused by a seizure, with patients complaining only of shoulder pain. Inferior dislocations (luxatio erecta) are rare and occur with the arm above the head at the time of injury. The patient presents with the forearm elevated to the level of the forehead and reports, “I can’t put my arm down.” Neurovascular injury and fracture often accompany these unusual dislocations.
What To Do:
 Quickly examine the patient to rule out neurologic or vascular deficits. Test and record the sensation over the deltoid to establish whether there is an injury to the axillary nerve (approximately 1% incidence).
Quickly examine the patient to rule out neurologic or vascular deficits. Test and record the sensation over the deltoid to establish whether there is an injury to the axillary nerve (approximately 1% incidence).
 Provide analgesia when necessary; IV narcotics may be needed.
Provide analgesia when necessary; IV narcotics may be needed.
 An alternative is the use of intra-articular lidocaine. After preparing the skin with povidone-iodine, using a 1½-inch, 20-gauge needle, inject 20 mL of 1% lidocaine 2 cm inferiorly and directly lateral to the acromion, in the lateral sulcus left by the absent humeral head.
An alternative is the use of intra-articular lidocaine. After preparing the skin with povidone-iodine, using a 1½-inch, 20-gauge needle, inject 20 mL of 1% lidocaine 2 cm inferiorly and directly lateral to the acromion, in the lateral sulcus left by the absent humeral head.
 Often, analgesics are not needed. If the clinician can gain the patient’s trust, apply gentle, stabilizing traction to the patient’s affected arm.
Often, analgesics are not needed. If the clinician can gain the patient’s trust, apply gentle, stabilizing traction to the patient’s affected arm.
 Reduction should be performed promptly. Obtaining radiographs may be unnecessary and may serve only to delay this procedure. There is no need to obtain radiographs when you feel confident about your clinical diagnosis and there was a relatively atraumatic mechanism of injury (especially when there is a history of a previous shoulder dislocation).
Reduction should be performed promptly. Obtaining radiographs may be unnecessary and may serve only to delay this procedure. There is no need to obtain radiographs when you feel confident about your clinical diagnosis and there was a relatively atraumatic mechanism of injury (especially when there is a history of a previous shoulder dislocation).
 Radiographs should be obtained in patients older than 40 years of age and when significant trauma is involved, such as from a fall from a height or a motor vehicle collision.
Radiographs should be obtained in patients older than 40 years of age and when significant trauma is involved, such as from a fall from a height or a motor vehicle collision.
 Keep in mind that with the exception of proximal humeral fractures, fractures are not contraindications to reduction.
Keep in mind that with the exception of proximal humeral fractures, fractures are not contraindications to reduction.
 If the patient is relatively comfortable and cooperative, you can begin reducing the shoulder without first starting an IV for administering analgesics. Muscle spasm is the main obstacle, and gentle and gradual maneuvers are always more likely to be successful than high-force rapid movement techniques, which are more likely to cause complications.
If the patient is relatively comfortable and cooperative, you can begin reducing the shoulder without first starting an IV for administering analgesics. Muscle spasm is the main obstacle, and gentle and gradual maneuvers are always more likely to be successful than high-force rapid movement techniques, which are more likely to cause complications.
 Patients who cannot relax because of pain should be given either intra-articular lidocaine or procedural sedation and analgesia (PSA) (see Appendix E).
Patients who cannot relax because of pain should be given either intra-articular lidocaine or procedural sedation and analgesia (PSA) (see Appendix E).
 Positioning is more important than strength for relocation. Several techniques can be employed successfully. If one does not work, try another.
Positioning is more important than strength for relocation. Several techniques can be employed successfully. If one does not work, try another.
 With all techniques, gain the patient’s confidence by holding the arm securely, asking him to relax. Tell him that there will not be any sudden movements and that if any pain occurs, you will stop and let him get comfortable before starting again. Then, in a very calm and gentle manner, ask the patient to let his muscles go loose so that his shoulder can stretch out “like taffy.” This may need to be said repeatedly.
With all techniques, gain the patient’s confidence by holding the arm securely, asking him to relax. Tell him that there will not be any sudden movements and that if any pain occurs, you will stop and let him get comfortable before starting again. Then, in a very calm and gentle manner, ask the patient to let his muscles go loose so that his shoulder can stretch out “like taffy.” This may need to be said repeatedly.

 Using a modified Hennepin technique with the elbow flexed at 90 degrees, apply steady traction at the distal humerus. Pull inferiorly and, at the same time, externally rotate the forearm very, very slowly. If the patient complains of pain, stop rotating, allow him to relax, and let the shoulder muscles stretch while traction is maintained along the humerus. Resume external rotation when he is comfortable again. Using this method, full external rotation alone will reduce most anterior shoulder dislocations (Figure 131-2, A).
Using a modified Hennepin technique with the elbow flexed at 90 degrees, apply steady traction at the distal humerus. Pull inferiorly and, at the same time, externally rotate the forearm very, very slowly. If the patient complains of pain, stop rotating, allow him to relax, and let the shoulder muscles stretch while traction is maintained along the humerus. Resume external rotation when he is comfortable again. Using this method, full external rotation alone will reduce most anterior shoulder dislocations (Figure 131-2, A).
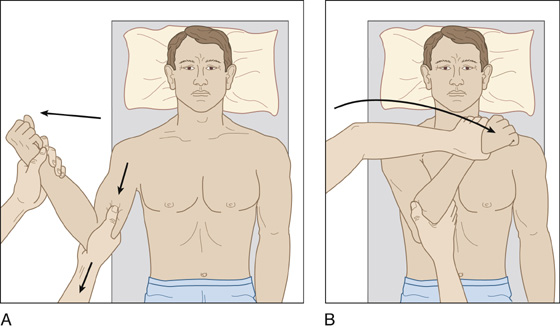
Figure 131-2 A, Slow and gentle external rotation technique. B, Slow and gentle adduction followed by gradual internal rotation will reduce the majority of dislocations that do not respond to external rotation alone. (Adapted from Ruiz E, Cicero JJ: Emergency management of skeletal injuries. St Louis, 1995, Mosby.)
 If the shoulder joint is not felt or seen to reduce, slowly and gently adduct the humerus while maintaining traction and external rotation until the humerus is against the anterior chest wall, and then very slowly internally rotate the forearm until it meets the anterior chest. Most shoulder dislocations can be reduced comfortably this way, often without the use of any analgesics (Figure 131-2, B).
If the shoulder joint is not felt or seen to reduce, slowly and gently adduct the humerus while maintaining traction and external rotation until the humerus is against the anterior chest wall, and then very slowly internally rotate the forearm until it meets the anterior chest. Most shoulder dislocations can be reduced comfortably this way, often without the use of any analgesics (Figure 131-2, B).
 Scapular rotation is an alternative technique that can be used when the lateral border of the scapula can be palpated. Reduction is accomplished by scapular manipulation. With the patient sitting up, have an assistant face the patient and gently lift the outstretched wrist of the affected arm until it is horizontal. The assistant then places the palm of his free hand against the midclavicular area of the injured shoulder as counterbalance and then gently but firmly pulls the patient’s arm toward himself while applying slight external rotation to the humerus. At the same time, manipulate the scapula by pushing the inferior tip medially and dorsally using both thumbs, while stabilizing the superior aspect of the scapula with the upper hand (Figure 131-3).
Scapular rotation is an alternative technique that can be used when the lateral border of the scapula can be palpated. Reduction is accomplished by scapular manipulation. With the patient sitting up, have an assistant face the patient and gently lift the outstretched wrist of the affected arm until it is horizontal. The assistant then places the palm of his free hand against the midclavicular area of the injured shoulder as counterbalance and then gently but firmly pulls the patient’s arm toward himself while applying slight external rotation to the humerus. At the same time, manipulate the scapula by pushing the inferior tip medially and dorsally using both thumbs, while stabilizing the superior aspect of the scapula with the upper hand (Figure 131-3).
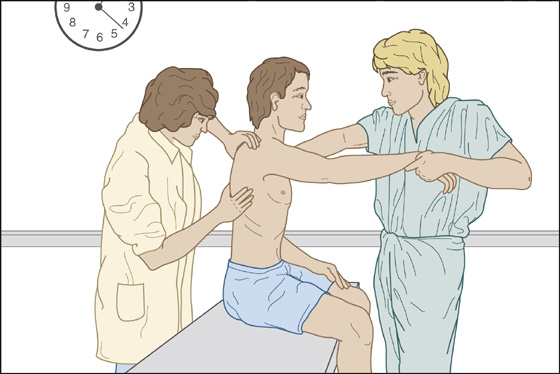
Figure 131-3 Scapular rotation technique.
 This technique can be modified by placing the patient in the prone position with the affected arm hanging dependent over the side of the examination table. Downward traction is applied to the arm with the same slight external rotation of the humerus, and scapular rotation is performed in the same manner as noted earlier.
This technique can be modified by placing the patient in the prone position with the affected arm hanging dependent over the side of the examination table. Downward traction is applied to the arm with the same slight external rotation of the humerus, and scapular rotation is performed in the same manner as noted earlier.
 The Spaso technique for reducing anterior shoulder dislocations is simple, requires minimal force, and can be performed by a single clinician. With the patient supine, the clinician grasps the wrist or distal forearm of the affected extremity, very slowly lifts the arm vertically, and, with application of gentle traction, rotates the humerus slightly externally until a “clunk” is felt, indicating a successful reduction.
The Spaso technique for reducing anterior shoulder dislocations is simple, requires minimal force, and can be performed by a single clinician. With the patient supine, the clinician grasps the wrist or distal forearm of the affected extremity, very slowly lifts the arm vertically, and, with application of gentle traction, rotates the humerus slightly externally until a “clunk” is felt, indicating a successful reduction.
 The Cunningham technique is reported to be painless and fast, using only proper positioning and massage to accomplish reduction. Seat the patient comfortably, as upright as possible, with shoulders relaxed. Supporting the affected arm, slowly and gently move the humerus into full adduction. Gently massage the trapezius and deltoids; this helps to relax the patient and reassures that the doctor is not going to do anything painful.
The Cunningham technique is reported to be painless and fast, using only proper positioning and massage to accomplish reduction. Seat the patient comfortably, as upright as possible, with shoulders relaxed. Supporting the affected arm, slowly and gently move the humerus into full adduction. Gently massage the trapezius and deltoids; this helps to relax the patient and reassures that the doctor is not going to do anything painful.
 Then, move on to gently massaging the biceps at the midhumeral level. Ask the patient to shrug his shoulders, continuing the biceps massage. Wait for the patient to relax fully, and the humeral head will slip back into place. (Warn the patient that it may feel strange as this happens and not to fight against the movement [Figures 131-4 and 131-5].) If the patient cannot relax enough to cooperate, or the arm cannot be adducted, this approach will not work. Videos and detailed instructions can be found at www.shoulderdislocation.net.
Then, move on to gently massaging the biceps at the midhumeral level. Ask the patient to shrug his shoulders, continuing the biceps massage. Wait for the patient to relax fully, and the humeral head will slip back into place. (Warn the patient that it may feel strange as this happens and not to fight against the movement [Figures 131-4 and 131-5].) If the patient cannot relax enough to cooperate, or the arm cannot be adducted, this approach will not work. Videos and detailed instructions can be found at www.shoulderdislocation.net.

Figure 131-4 Dr. Neil Cunningham demonstrates his technique for reducing shoulder dislocations. Seat the patient comfortably, as upright as possible, with shoulders relaxed. Supporting the affected arm, slowly and gently move the humerus into full adduction. Then gently massage the trapezius and deltoids. (Adapted from Shaw G: Breaking news: believe it or not: painless reduction of dislocated shoulders. Emerg Med News 33:1, 28, 2011.)

Figure 131-5 In the second part of the technique, Dr. Cunningham demonstrates how to gently massage the biceps at the midhumeral level. The next step is to ask the patient to shrug her shoulders, continuing the biceps massage. Wait for the patient to fully relax, and the humeral head will slip back into place. (Adapted from Shaw G: Breaking news: believe it or not: painless reduction of dislocated shoulders. Emerg Med News 33:1, 28, 2011.)
 For difficult reductions where PSA is being used, the traditional traction against countertraction method can be employed. In this method, while the patient lies supine, the clinician grasps the patient’s affected arm by the wrist and applies traction at a 45-degree angle of abduction while an assistant provides countertraction by wrapping a sheet around the patient’s torso and pulls on it in the opposite direction.
For difficult reductions where PSA is being used, the traditional traction against countertraction method can be employed. In this method, while the patient lies supine, the clinician grasps the patient’s affected arm by the wrist and applies traction at a 45-degree angle of abduction while an assistant provides countertraction by wrapping a sheet around the patient’s torso and pulls on it in the opposite direction.
 Reexamine the shoulder after it is reduced. Neurovascular status should again be rechecked.
Reexamine the shoulder after it is reduced. Neurovascular status should again be rechecked.
 Postreduction films are only required if there is uncertainty regarding reduction or if fractures were noted on prereduction radiographs. No studies to date have shown a single postreduction fracture, given the use of more modern, gentler techniques of reduction.
Postreduction films are only required if there is uncertainty regarding reduction or if fractures were noted on prereduction radiographs. No studies to date have shown a single postreduction fracture, given the use of more modern, gentler techniques of reduction.
 When the patient is comfortable and limited range of motion has been restored, secure the reduction in a sling and a swathe around the arm and chest. (Although this represents standard postreduction treatment, a recent study suggests that no immobilization at all may actually be the treatment of choice.)
When the patient is comfortable and limited range of motion has been restored, secure the reduction in a sling and a swathe around the arm and chest. (Although this represents standard postreduction treatment, a recent study suggests that no immobilization at all may actually be the treatment of choice.)
 Discharge the patient once he is alert, with a prescription for analgesics as needed and an appointment for orthopedic follow-up in 1 week (sooner if any problem).
Discharge the patient once he is alert, with a prescription for analgesics as needed and an appointment for orthopedic follow-up in 1 week (sooner if any problem).
What Not To Do:
 Do not perform any reduction technique using high-force or rapid movements.
Do not perform any reduction technique using high-force or rapid movements.
 Do not use the forearm as a lever to force reduction and possibly fracture the neck of the humerus.
Do not use the forearm as a lever to force reduction and possibly fracture the neck of the humerus.
 Do not redislocate the shoulder by repeating the motions of the mechanism of injury.
Do not redislocate the shoulder by repeating the motions of the mechanism of injury.
The shoulder is the most mobile joint in the human body. It allows the upper extremity to rotate up to 180 degrees in three different planes, enabling the arm to perform a versatile range of activities. This mobility comes at a cost: it leaves the shoulder prone to dislocation.
In younger patients, most shoulder dislocations are caused by direct trauma and sports injuries. In elderly persons, falls are the predominant cause, and the dislocation often is accompanied by a fracture.
An excessive external rotation or abduction force usually causes anterior dislocations, whereas posterior dislocations usually occur when the humeral head is driven posteriorly with great force and internal rotation, as during a seizure. Posterior dislocations can be subtle and more difficult to diagnose.
The strategy is to relocate the shoulder with minimal damage to the joint capsule and anterior labrum of the glenoid fossa, hoping the patient does not become a chronic dislocator with an unstable shoulder. Chronic dislocators are easier to reduce and come less often to the emergency department, because they learn how to relocate their own shoulders. Of patients whose first shoulder dislocation occurs before 20 years of age, 90% will have a recurrent dislocation. Only 14% of first dislocations after 40 years of age recur.
Posterior dislocations can be reduced using traditional in-line traction on the dislocated arm, along with countertraction using a sheet. Posterior pressure on the humeral head may help.
Inferior dislocations can also be reduced using traction/countertraction, but with scapular rotation as an adjunct.
Numerous studies have shown that early surgical intervention, rather than conservative treatment (especially in the younger athletic population), provides a reduced incidence of recurrent dislocation.
Treatment after reduction traditionally includes immobilization of the shoulder for 4 weeks, followed by rehabilitation. One Australian study suggests that putting the arm in internal rotation (the normal sling position) results in more pronounced labral detachment, inhibiting healing of the underlying injury. Additionally, for patients with anterior shoulder dislocation, sling immobilization (internal rotation) provides no benefit, and positioning in external rotation, using an Ultrasling or similar device, might be more effective.
It might be preferable not to immobilize the shoulder at all, and total immobilization may actually cause worse problems, such as a frozen shoulder, but this remains unproven. After 1 or 2 days, the patient with the uncomplicated shoulder, dislocation should be instructed to start gentle range of motion exercises to help prevent this complication. It should be stressed to the patient that they should not reproduce the position that originally caused the dislocation.

Full access? Get Clinical Tree


