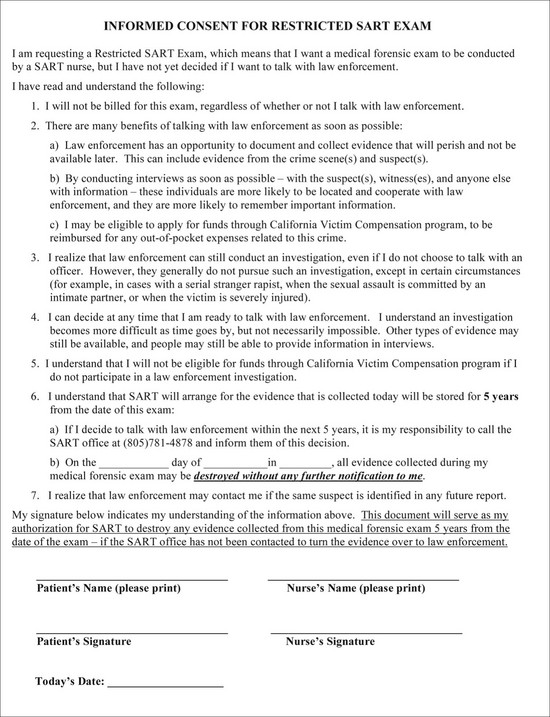
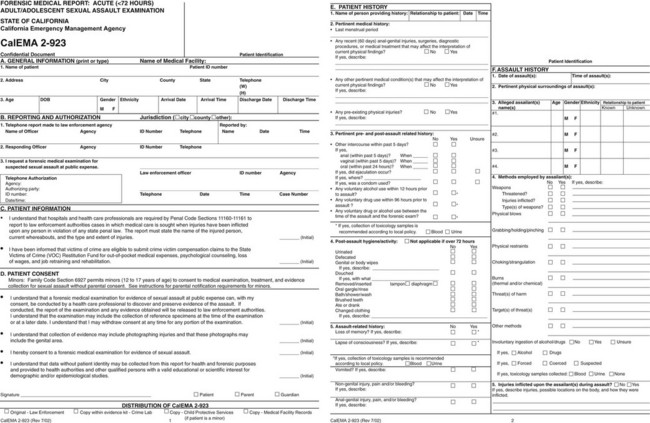
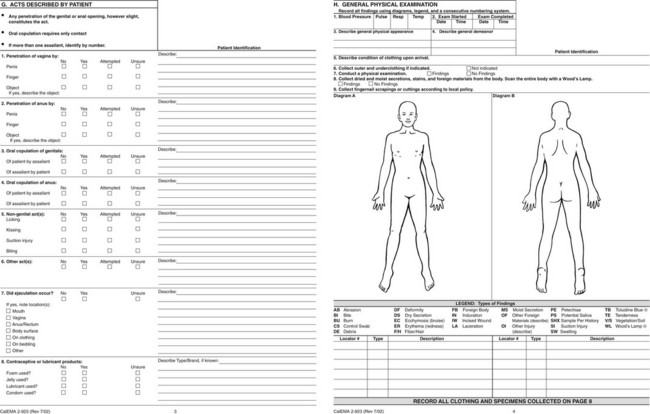
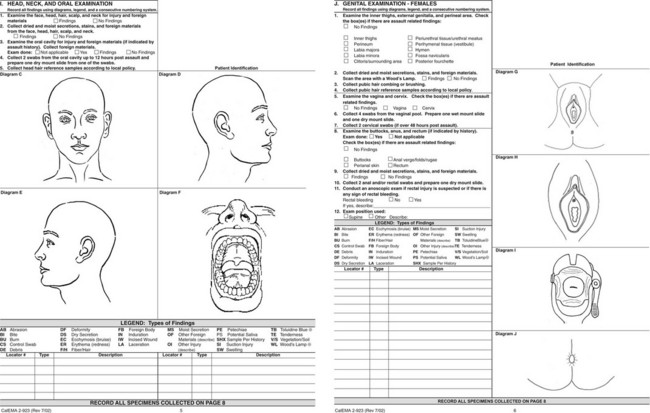
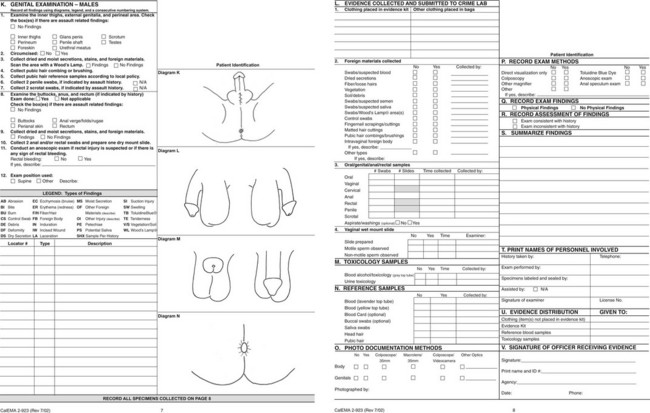
Chapter 67 Sexual violence is a significant problem in the United States. The Centers for Disease Control and Prevention have defined it as sexual activity in which consent is not obtained or not freely given. It pertains to a wide variety of sexual conduct and may entail, but does not require, penetration, completion, or, in certain cases, physical contact (e.g., voyeurism).1 Referred to in statute as sexual assault, it is explicated more precisely by state and local governments. Emergency physicians should be aware of local, state, and federal laws because emergency physicians may be mandated reporters and involved in the evaluation, treatment, evidence collection, and documentation of sexual assault. Major advances in the evaluation and management of sexual assault victims (SAVs) have occurred over the past 30 years. The formation of community-based multidisciplinary teams that first took hold in California is probably the most important. The development of a sexual assault response team (SART) with representatives from the district attorney’s office, law enforcement officials, crime laboratory personnel, medical personnel, including both physicians and nurses, social service agents, and victim advocates came together as a group. These major players have sought to solve the logistic, medical, psychological, legal, and social problems incurred by SAVs. The commitment and mutual cooperation of the SART led to the development of standardized protocols for the care and treatment of SAVs. These protocols specify the procedures for interviewing and examining the SAV and collecting, preserving, and storing evidentiary materials, and include the evidence kit and forms for documentation. Many jurisdictions have adopted this standardized system, and in 2004 the first national protocol was released by the U.S. Department of Justice.2 With a protocol in place, the necessity of having trained forensic examiners (FEs), irrespective of academic credentials, is evident.3,4 Currently, this role subsumes that of the sexual assault nurse examiner (SANE); the ubiquitous, mostly hospital-based SANE programs have contributed substantially to our knowledge and understanding of sexual assault and have improved the care of the victims.5,6 In addition, because of the use of special technologies, including colposcopy, digital photography and videography, and the alternate light source (ALS), the establishment of designated examination centers for sexual violence is increasingly prevalent.7 Much information about the characteristics, physical examination findings, and correlates of injury in SAVs is now available. This information facilitates the management of the SAV, improves the experience of the victim, and ultimately assists in the identification of the perpetrator. Although these changes began as a grassroots movement, a victim-centered, multidisciplinary team approach, including trained FEs, was codified by the federal government in the 1994 Violence Against Women Act (VAWA) and its subsequent iterations in 2000 and 2005. Forensic compliance issues for all states receiving grant monies from this bill began in 2009. Programs must now offer forensic examinations for all SAVs irrespective of whether they report or cooperate with law enforcement and with no out-of-pocket expenses to the SAV. This poses special problems for medical professionals practicing in states in which they are mandated reporters. As many as 18.5% of SAVs who delayed law enforcement involvement, changed their minds8; this raises multiple issues concerning evidence storage, as well as maintenance and chain of custody. Moreover, victim notification about the destruction of forensic evidence presents challenges in an anonymous system. Currently, health care facilities have no nationally regulated mandates, accreditation process, or quality assurance to address these specific problems. Allowing SAVs time to consider their options9–11 and providing them with high-quality health care12,13 have been shown to increase their cooperation with police investigations. (See Figure 67-1 for a sample of a form for special consent without law enforcement participation; also refer to www.ccfmtc.tv/pdfs/forms/CALEMA-924i.pdf for abbreviated examination form and protocol.) Based on national emergency department (ED) data, sexual assaults represented 10% of all assault-related injury visits to the ED by female patients in 2006. In 2007, for female individuals of all ages and for boys aged 1 to 9 years, sexual assault was the third leading cause of nonfatal violence-related injury.14 It is important to note that the cost of sexual violence to the health care system is high because it may include not only the initial visit for the crime but also subsequent visits for other health-related issues.7 Women remain the predominate victims (94%), although male victims tend to be victimized at an earlier age.15 Historically, sexual assault has been a largely unreported crime, with only about a third of SAVs coming forward. The major reasons for not reporting include not wanting the assailant to go to jail, having a prior relationship with the assailant, and feeling that the police would blame the victim or be insensitive. Some have sited fear of reprisal, including death, media attention, and shame, for their reluctance.16 The closer the relationship between the victim and offender, the less likely the SAV has been to report the crime17; the relationship between SAV and perpetrator is often absent in the medical record, yet it is critical for safety planning.18,19 A substantial number of SAVs report at or after 72 hours, and they are typically adolescents. There is a high positive correlation between reporting to the police and receiving medical treatment20; early intervention is key to diminishing adverse psychological and physical outcomes for the SAV.17,21 Sexual assault is an extremely common crime, with estimates of 1 in 6 females and 1 in 33 males being assaulted during their lifetime.15 The mean age of a female victim is approximately 20 years. She is most often single. Adolescents account for less than half of all victims seen, yet the incidence of sexual assault peaks in the age group of 16 to 19 years.22 For nearly 40% of victims, sexual assault is the first sexual experience.23 Eighty percent of the time, a person known to the victim perpetrates the assault.15 Former and current boyfriends are equally common as perpetrators, lending support to the position that leaving a violent partner does not always end the violence.19 The younger the victim, the more likely the perpetrator is to be a relative. The location of the sexual assault varies with the victim and the type of perpetrator. In general, adults are usually assaulted in their own home, whereas adolescents are more likely to be assaulted in the assailant’s residence.24 Stranger assaults are less common for both males and females15; they are more likely to involve adults, occur outdoors, and include the use of a weapon and have a greater likelihood of injury.25–27 Alcohol and drug use are common accompaniments to sexual assault.28 Other vulnerable populations include the mentally or physically disabled, the homeless, elderly individuals, sex trade workers, and those previously incarcerated.29,30 Higher rates of sexual assault also occur during college, military service, war, and natural disaster.31 Most assaults involve penile-vaginal penetration,32 and penile penetration is significantly associated with genital injury in females.33 Typically, digital-vaginal penetration is the second most common sexual act reported. Oral-genital contact occurs in less than 30%, with anal assault slightly less common.23,34–36 The use of a foreign object is unusual (10%) and associated with increased trauma.32,37 Anal assault is associated with increased violence,23,25,38,39 offender preference for anal sex,40 and offender problems with sexual dysfunction.41,42 Injury is not an inevitable consequence of sexual assault.4,43,44 Adolescent SAVs have been shown to sustain more anogenital injuries than their adult counterparts.26,32,45 Nongenital trauma occurs in 40 to 81% of SAVs, and its presence is associated with anogenital injury.39,45 For nongenital trauma, the extremities are the most commonly injured, followed by the head and neck.46 Serious injury involving hospitalization occurs in about 5%,7 and death associated with sexual assault is estimated at 1% or less, although this latter figure is probably a gross underestimate.38,47,48 Psychological distress and interpersonal difficulties are the major sequelae after sexual assault. These problems are exacerbated in SAVs with known attackers who delay reporting.21,49 Emergency Department Preparation The ED should also be prepared for the unusual victim with significant or life-threatening injuries. In this instance the emergency physician needs to delegate the forensic responsibility to another forensically trained staff member whose sole purpose is to collect the evidence and, if required, follow the SAV to surgery. In cases in which there is substantial injury, following the patient from intake allows the examiner to understand better and document the nature and extent of the trauma and continue the forensic process with little further distress to the patient.50 Numerous consents should be obtained from the SAV, depending on state and local laws (Box 67-1). The FE should be knowledgeable about all statutes governing consent, including whether minors need parental consent. In some states, even if parental consent is not required, the FE may still be required to contact the parents and document the success or failure of this attempt. Most SAVs are concerned about access to the SART record and photographs, particularly when the SART examination facility is within the hospital setting. Keeping these records separate from the primary hospital chart system helps protect the privacy of the victim and has a precedent in the similar handling of psychiatric records. Surveys of SAVs have identified that they desire information about sexually transmitted diseases (STDs), pregnancy, emergency contraception, follow-up care, and physical and psychological health effects of sexual assault.51 Connecting the SAV to outside resources is critically important to care.52,53 Providing written information on these topics to the patient and getting his or her signature in confirmation documents the patient’s receipt of follow-up recommendations. Before the history taking is begun, the SAV’s immediate privacy and personal needs should be addressed. Box 67-2 outlines some of the issues that may make the interview more comfortable for the patient and ensure receipt of reliable historical information from the patient. The group taking the history may include a law enforcement officer, patient advocate, medical assistant, and FE. A detailed history is important. California was the first state to mandate a uniform examination protocol and specific training for examiners (Fig. 67-2).54 Figure 67-2 Forensic Medical Report: Acute (<72 hours) Adult/Adolescent Sexual Assault CalEMA 2-923 from the State of California Emergency Management Agency. This form is available at http://www.calema.ca.gov/PublicSafetyandVictimServices/Documents/Forms%202011/Medical%20forms/Acute%20Adult%202-923.pdf. Accessed January 20, 2013. Questions about sexual acts need to be explicit and phrased in terms understandable to the SAV. Unless specifically asked, many victims will not disclose that injuries are a result of the assault.19 Language used by the SAV to describe sexual acts should be documented in the medical record. It is important for the FE to ascertain whether the victim voiced her lack of consent and whether that terminated the behavior. The victim’s own words should be used as often as possible and recorded in quotation marks to preserve the integrity of the interview; if the police record the interview, it may not be transcribed until weeks or months later. The experienced FE also gathers information about the sequence and type of sexual acts that occurred during an assault, including not only kissing, fondling, use of foreign objects, and digital manipulation, but also fetishism, voyeurism, or exhibitionism on the part of the suspect. Table 67-1 lists additional information, which may be useful for the investigation. Table 67-1 Useful Information Not Routinely Found on the Sexual Assault Forms The ubiquitous nature of recording devices means that an important, early question to ask of the victim is whether such devices were used by the suspect or bystanders; this may provide evidence of the assault.55 Inquiry about drug and alcohol usage is important and necessary.56–58 Like driving under the influence, a sexual assault may be the first indicator that the victim has a drug or alcohol problem.59 Recent data indicate that drug and alcohol abuse by the victim is associated with a concurrent increased risk of an additional assault in the next 2 years; assaulted drug users are at risk for an escalation of drug abuse after the assault60 and self-blame.61 These victims need prompt referral for counseling and drug rehabilitation programs, a service frequently overlooked by forensic teams.62 Furthermore, the use of drugs and alcohol are relevant to issues of consent, credibility, and corroboration.63,64 In the past, studies have not found a correlation between substance use and injury,65 but recent studies indicate an increase in nongenital26,43 and anogenital.33 trauma. The FE should order drug screening if the victim reports loss of consciousness or forced ingestion, appears confused, is amnesic, or has other changes in physical or vital signs that are suspicious for drug use.55 National drug screening data from SAVs show that the prevalence of drug use is higher among SAVs than the general population.66,67 Moreover, drugs are frequently used in combination. The two most popular combinations are alcohol and marijuana, followed by alcohol and benzodiazepines.68 Routine surveillance for drugs and alcohol is recommended because self-reporting is inaccurate69 and drug-facilitated sexual assault appears to be increasing worldwide.70,71 Screening should include blood, urine, and, with newer technology, samples of head hair.72 Special policies and procedures need to be developed for SAVs who are incapacitated or are otherwise incapable of giving consent.73,74 One should not forget to inquire whether the suspect used drugs or alcohol. Perpetrators who use drugs and alcohol are less likely to use condoms, and on apprehension, drug testing will be needed to confirm this information and should be routine. A history of childhood abuse increases the risk of repeat assault. Researchers now believe that identification of this vulnerable group is a prerequisite for prevention. The sexual assault examination may be the one time during which the question of prior abuse is raised; a positive answer provides additional justification for referral for psychological services.29 About a quarter of the victims requiring sexual assault evaluation will have mental health problems. A history of mental illness has been shown to increase the severity of the sexual and physical attack. Moreover, the sexual assault often results in an exacerbation of the mental illness and a higher rate of post-traumatic stress disorder.75 Similar vulnerabilities accrue to sex trade workers and to women with a history of previous incarceration, current or past substance abuse, or homelessness.29 Knowledge about the victim’s prior sexual experience is pertinent. New information has emerged that women without sexual experience are more likely to sustain genital trauma and specifically more likely to have hymenal tearing.76 Because hymenal and vaginal tears are usually associated with the dramatic presentation of bleeding, it is incumbent on the examiner to ascertain the source of hemorrhage. The lack of visible genital injury in the female who has not had prior sexual experience does not exclude the possibility of intercourse. Much can be gleaned about the suspect from a careful interview of the SAV. Areas of interest for the examiner include the methods of approach and control of the SAV, the offender’s reaction to resistance by the victim, and the occurrence of sexual dysfunction in the suspect. Although the approach to the victim is usually easy to obtain, understanding how the suspect controlled the victim may not be immediately clear, as the mere presence of the suspect may be perceived by the victim as a threat to life and may result in control of the victim’s actions. Most protocols inquire about verbal threats and weapons, but getting the exact context of these (verbatim if possible) and determining whether the threats were carried out are important. Few assaults are silent; one should inquire about demands, reassurance, compliments, questions, concern, or apologies by the perpetrator. Similarly, if a weapon was used, notation should be made regarding whether the victim saw the weapon or whether it remained a verbal threat only. Was it a weapon of choice (brought with the suspect) or one of opportunity? Did the suspect relinquish it at any time or use it? The examiner should inquire into the amount and timing of the force used by the assailant along with the use of any derogatory or profane language. The examiner should inquire about strangulation; SAVs typically do not volunteer this information. Strangulation tends to occur late in abusive relationships and has been associated with a higher risk for major morbidity and mortality.77,78 The FE should take special care to ask questions in a manner that does not imply that the victim should have done something to protect herself or to prevent the occurrence of the sexual assault. In some cases, resistance may provoke an alternative demand, compromise, negotiation, and threat of force or use of force. If force is threatened, the examiner should be clear about whether it was used and understand how much and how long it was applied. If a change of demeanor occurred, the FE should know what caused it and what was the change.79 Nearly 34% of convicted rapists have a sexual dysfunction, and this information is obtainable from the SAV. Sexual dysfunction includes impotence, premature ejaculation, retarded ejaculation, or conditioned ejaculation (Box 67-3). This knowledge improves the examiner’s ability to understand and collect the evidence. A premature ejaculator may have left semen on clothing or in the environment rather than intravaginally. Retarded ejaculation is associated with multiple sex acts, including anal intercourse, and a more violent attack, involving both genital and nongenital trauma.39,80 Serial rapists have been identified based on language and demand for a specific order of sexual acts from several SAVs. In addition, the SAV can be asked about any unique lesions or pathology of the perpetrator’s genitalia or other identifying characteristics.81 Penetration with a foreign object is associated with greater violence and an increased prevalence of genital and nongenital trauma, stranger assault, and multiple assailants.33,37 The FE should understand that the definition of a foreign object on the forensic medical form is not the same as the legal definition. The legal definition of foreign object is any substance, instrument, or device, including any body part other than a sexual organ.82 The FE should inquire about the methods used to avoid detection and facilitate escape, such as wearing masks or gloves, blindfolding the victim, or disabling the phone. An experienced assailant may also attempt to destroy evidence, such as forcing the victim to shower. Lastly, the FE should ask about missing items. Valuables or personal items retained as souvenirs have evidentiary value. The FE should ask the victim if the assailant is known to him or her; even if the assailant is unknown, the victim may have a wealth of information about characteristics and behavior of the assailant.41 The physical examination should be meticulous and include the collection of trace evidence and reference standards (see Fig. 67-2). There is a positive association between SAV injury and the filing of charges, successful prosecution, and sentencing.5,83 In general, the sequence of observation, photography in situ, collection of evidence, and written documentation should be followed (Box 67-4). All items should be dry and placed in paper containers (plastic is not used because it inhibits drying and degrades biologic evidence) that are labeled (Box 67-5) and sealed. Each container should be sealed securely with tape, and the examiner should initial or sign across the tape and onto the container or bag. For the integrity of the evidence to be preserved, the SAV should not be left alone in the room with it, and the FE should wear powder-free gloves to prevent contamination of the evidence. If the evidence is stored, a locked unit should be available. Methods for preserving the chain of custody, a fundamental principle in the criminal justice system, should be understood by all personnel (Box 67-6). A complete examination and historically relevant evidence collection should be performed, irrespective of the time between assault and examination. One investigator documents the retrieval of salivary DNA from a bite mark on a body even after the body had been submerged in water for more than 5 hours.84 The FE should not second-guess what the laboratory may or may not recover based on rigid time frames. If there is a history of loss of consciousness or significant memory impairment, then all specimens should be collected. The FE needs to describe the SAV’s demeanor and general appearance. The examiner should be especially careful to use specific terms and note responsiveness and ability to cooperate and give a history. All clothing worn during the assault should be inspected, collected, and photographed. A Wood’s lamp or ALS should be used to detect dried secretions and to document the findings (Box 67-7). BOX 67-7 Wood’s Lamp and Alternate Light Source High-intensity, tunable light source Uses four narrow bands: 450, 485, 525, and 570 m Two wide bands: white light, all wavelengths below 530 nm Colored goggles used to block the reflected light and pass only the fluorescent light Because of absorptive differences between normal and damaged tissues, can detect injuries not seen with the naked eye More accurate for certain body fluids and substances than Wood’s lamp
Sexual Assault
Perspective
Epidemiology
Distinguishing Principles of Disease
Obtaining the History and Consent
History of Type of Sexual Assault
Positions used during the assault
Affects the location of injury
Positions used during the examination
Helps to orient pictures
Sexual dysfunction in the suspect
Associated with increased violence and anal attack
Repeated thrusting by suspect
May explain loss of seminal product
Victim assistance with insertion of penis
May explain lack of genital injury
Did penis remain in vagina after ejaculation?
May explain loss of seminal product
How do you know ejaculation occurred?
Helps determine where semen may be found
Prior sexual experience
Lack of sexual experience associated with increased hymenal trauma
Gravity and parity
May be a factor in genital injury
History of prior victimization
At increased risk for post-traumatic stress disorder; need triage for counseling
Mental health history, sex trade worker, previous incarceration, homeless, history of substance abuse
Increased severity of attack, worsening mental health problems, increased risk of revictimization, worsening drug use
Past medical history
May explain physical or laboratory findings
Sexual arousal and response
Need to assuage guilt, understand prevalence; may alter physical findings
Use of Recording Devices by Suspect or Bystanders
Drug and Alcohol Use
History of Child Abuse
Mental Illness
Prior Sexual Experience
Methods of Controlling the Victim
Sexual Dysfunction in Offenders
Use of Foreign Object
Methods Used by the Offender to Avoid Detection
Performing the Physical Examination and Evidence Collection
Examination of the Skin

Full access? Get Clinical Tree


Sexual Assault