8) following head trauma with either
- Significant mechanism of injury (fall from height, high speed MVC), or
- Significant physical examination findings (depressed skull fracture, facial trauma, scalp lacerations).
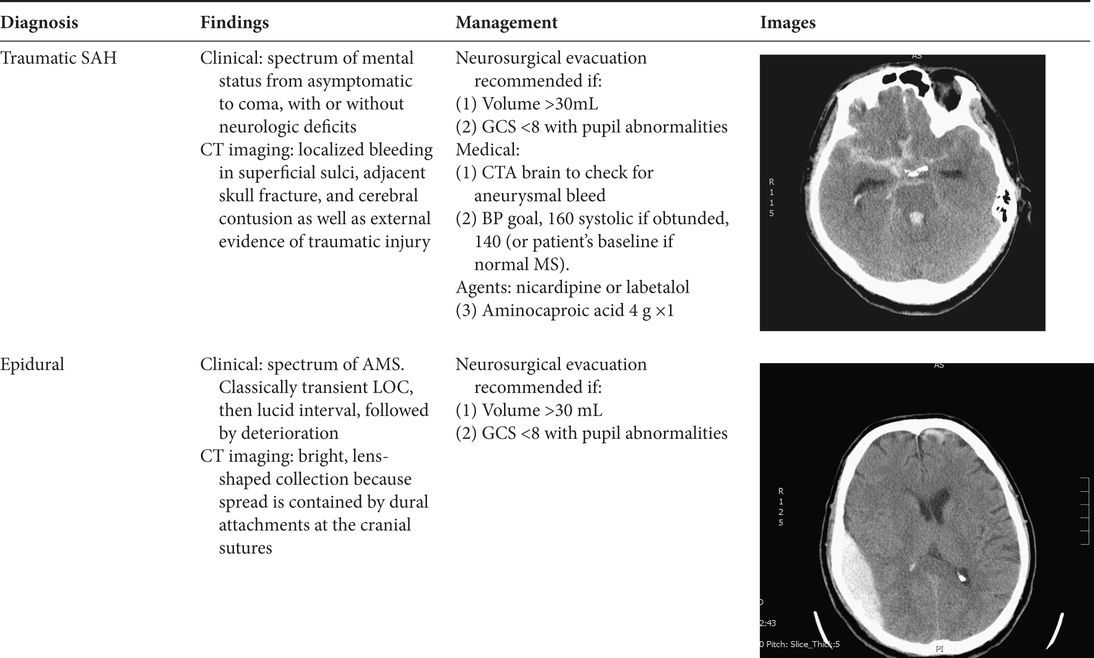
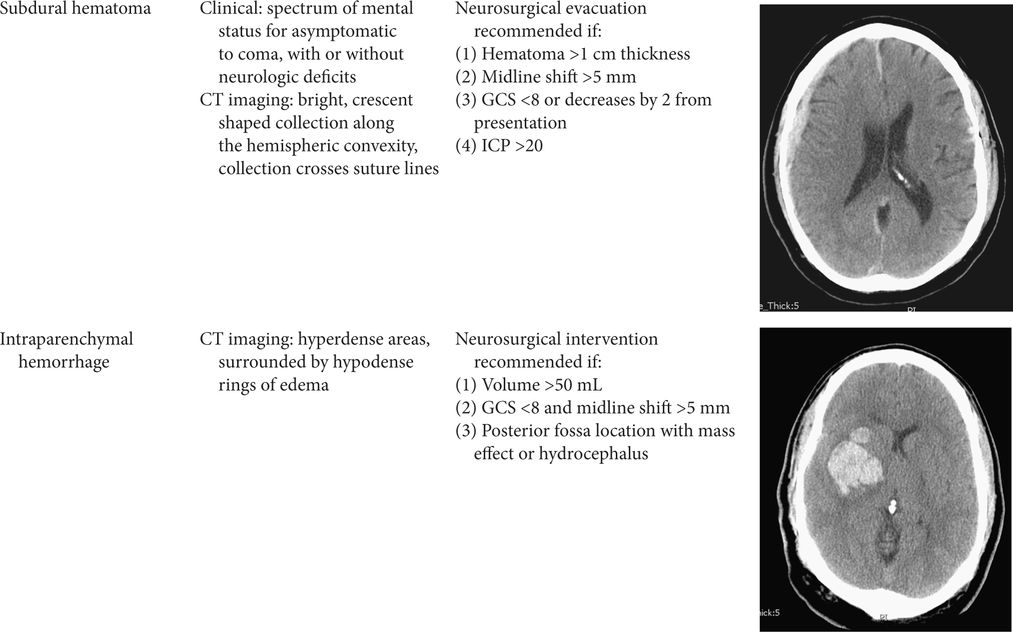
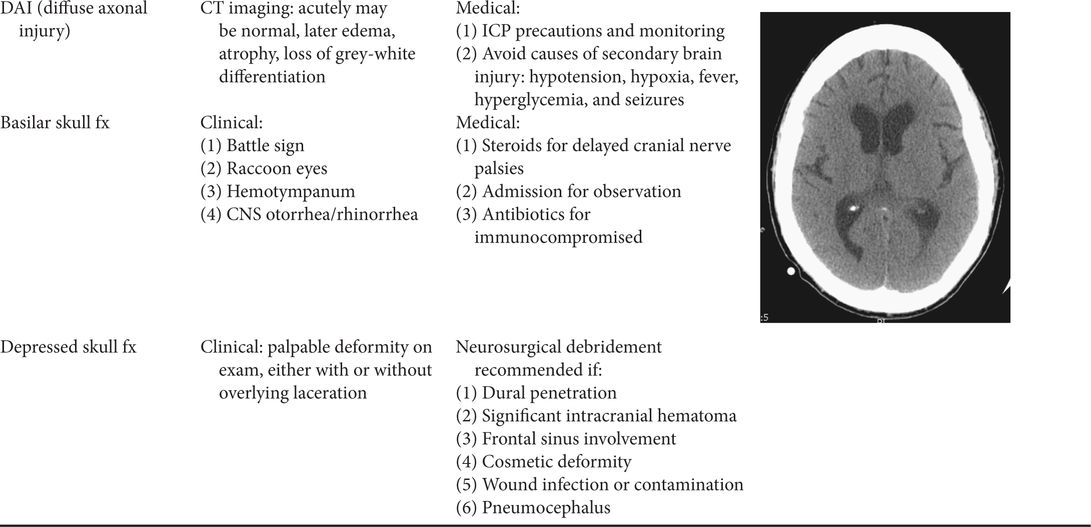
Table 7.1. Common traumatic brain injury patterns
Management
Glasgow Coma Scale
- Calculate concurrently with other resuscitation efforts.
- Preferably before administration of any sedative or paralytic medications.
- Also perform pupillary reflex examination.
Add the total of each column.
Airway
- Early intubation is indicated in all severe TBI patients.
- Maintain c-spine precautions until clearance is possible (i.e., rigid cervical collar, logroll the patient, do not allow them to flex or extend the neck).
Rapid sequence intubation (RSI)
- The cerebral perfusion of severe TBI patients is tenuous, and first pass intubation is critical.
- The RSI medications should include a sedative and a paralytic agent with these objectives:
- Maintenance of hemodynamic stability and CNS perfusion
- Maintenance of adequate oxygenation
- Prevention of increases in intracranial hypertension
- Prevention of vomiting and aspiration.
- Maintenance of hemodynamic stability and CNS perfusion
- Pretreatment may help minimize increase in intracranial pressure (ICP) during intubation (no strong evidence to support its use and not universally used):
- Lidocaine (1.5 mg/kg) intravenous push 3 minutes prior to induction
- Fentanyl (3 micrograms/kg) slow intravenous push 3 minutes prior to induction, after lidocaine.
- Lidocaine (1.5 mg/kg) intravenous push 3 minutes prior to induction
Induction agents
- Etomidate (0.3 mg/kg) has been demonstrated to be hemodynamically stable and not increase ICP.
- Ketamine (1.5 mg/kg) should be considered if hypotensive or normotensive (avoid if the patient is already hypertensive).
Paralytic agents
- Rocuronium (RSI dose 1.2 mg/kg), onset of action 45–60 seconds.
- Succinylcholine (1.5 mg/kg IV), onset of action 45–60 seconds (avoid in patients with crush injuries).
- Vecuronium (0.1–0.2 mg/kg), onset of action 60–90 seconds.
Breathing
- Avoid hypoxemia and hyperoxemia (goal pulse oximeter of 95%).
- Monitor with quantitative end-tidal PaCO2.
- Maintain PaCO2 levels of 35–38 mmHg.
Circulation
- The goal is to maintain blood flow to the brain. The important measure is cerebral perfusion pressure (CPP), as opposed to systolic blood pressure (SBP). CPP = MAP − ICP. Systemic hypotension causes a decrease in CPP and must be avoided. If someone has increased ICP they need a higher blood pressure to maintain cerebral perfusion.
- 500 mL to 1 L boluses of isotonic crystalloid should be given to maintain SBP >90.
Intracranial pressure
- Intracranial pressure is normally
 15 mmHg.
15 mmHg.
- Traumatic causes of increased ICP:
- Intracranial mass lesions (hematomas)
- Cerebral edema (acute hypoxic ischemic encephalopathy, large cerebral infarction, severe traumatic brain injury)
- Obstructive hydrocephalus.
- Intracranial mass lesions (hematomas)
- See the table below for clinical signs of increased ICP and impending herniation.
| Clinical signs of increased ICP and impending herniation |
|---|
| Unilateral or bilateral fixed and dilated pupil(s) |
| Decorticate or decerebrate posturing |
| Cushing reflex: bradycardia, hypertension, and/or respiratory depression |
| Decrease in GCS >2 |



Full access? Get Clinical Tree


