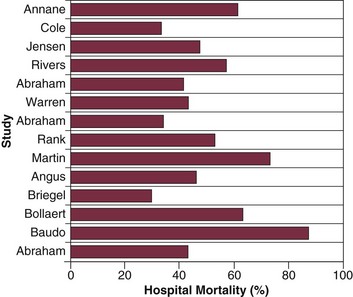
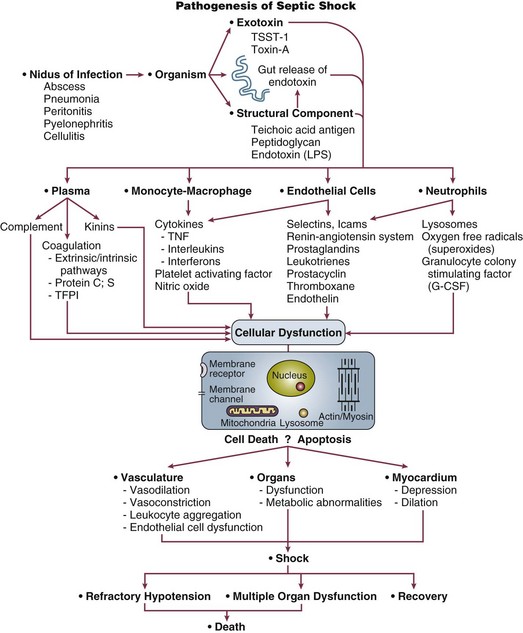
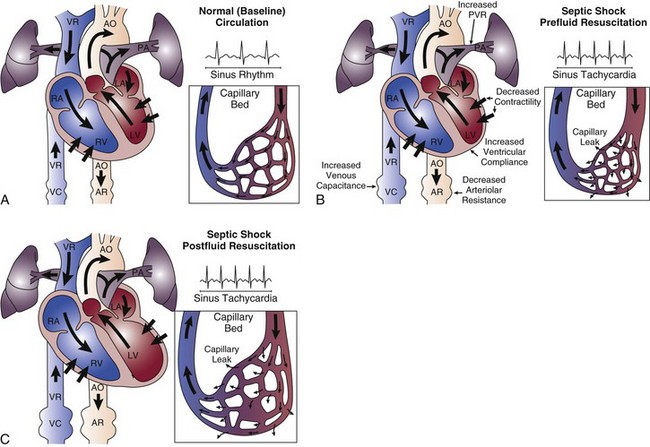
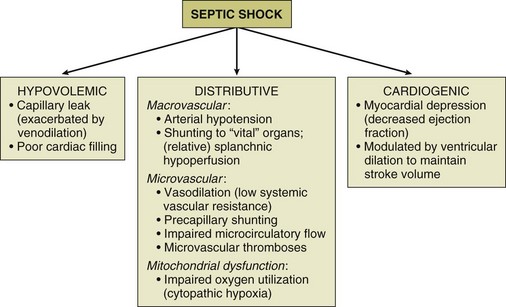
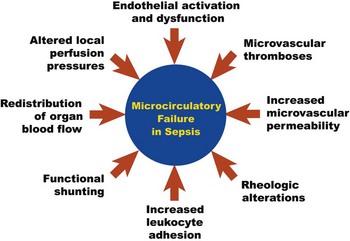
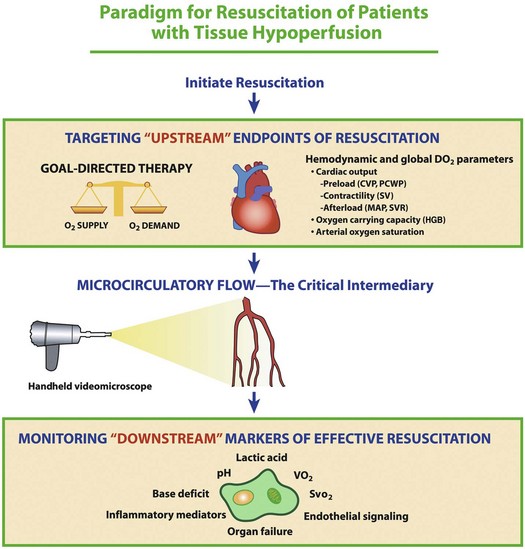
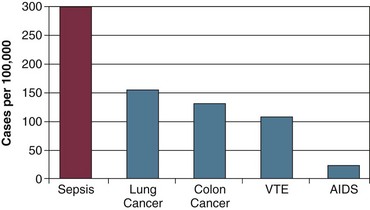
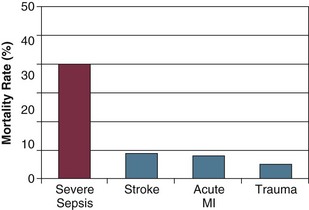
23 This chapter pertains to pathophysiology, assessment, and management of septic shock, the most severe and overt manifestation of the septic condition. This discussion will specifically focus on cardiovascular and hemodynamic aspects. Other critically important elements of sepsis pathophysiology, assessment, and management (i.e., beyond the cardiovascular and hemodynamic aspects) will be addressed in a separate chapter (see Chapter 25, Sepsis and Multiple Organ Dysfunction). This chapter is also focused specifically on the adult patient with septic shock, as principles and evidence may differ in important ways in the pediatric population. The word sepsis originated from the Greek language. Sepsis was synonymous with putrefaction and pertained to the bacteria-mediated decomposition of organic matter.1 The term persisted for more than 2700 years with essentially unchanged meaning.2 In the twentieth century, our modern understanding of the term sepsis became rooted in a disease in which the clinical manifestations were attributed to severe infection and the release of pathogenic bacterial products into the patient’s bloodstream.3,4 The term shock comes from the French word “choquer,” meaning “to collide with.” This is particularly appropriate terminology for shock due to sepsis, given our modern understanding of the sepsis pathophysiology, whereby the body’s host defenses essentially collide with the invading microorganism, triggering a profound proinflammatory host response.1 Shock is defined as a failure of the cardiovascular system to maintain effective tissue perfusion. If effective tissue perfusion is not promptly restored, cellular dysfunction and acute organ failure may occur and may become irreversible, leading to acute organ system failure. When shock develops because of a systemic inflammatory response to infection, it is termed septic shock. The American College of Chest Physicians (ACCP) and the Society of Critical Care Medicine (SCCM) first published consensus conference definitions for sepsis syndromes more than 20 years ago,5 and these definitions were revisited and further developed by international consensus in 2003.6 Septic shock was defined as infection-induced hypotension (systolic blood pressure <90 mm Hg [or a drop of >40 mm Hg] plus signs of tissue hypoperfusion despite adequate fluid resuscitation). The concurrent presence of clinical signs of tissue hypoperfusion (e.g., metabolic acidosis, encephalopathy, acute lung injury, oliguria, acute kidney injury, peripheral extremity discoloration, or impaired capillary refill) is an integral component of making the diagnosis of septic shock, because baseline blood pressure can vary among patients, and patients with lower baseline blood pressure may tolerate an arterial pressure lower than the values stated here without being in circulatory shock. The overarching purpose and major impact of the efforts to establish the contemporary definitions given here was the promotion of uniformity in inclusion criteria for sepsis clinical trials.7 Severe sepsis (sepsis plus acute organ system dysfunction) is a common and deadly disease with major public health implications. Although heterogeneity of definitions of sepsis has historically made the incidence of severe sepsis and septic shock difficult to precisely measure, estimates of the incidence have been possible. Using the International Classification of Diseases (ICD)-9 codes for infection and organ dysfunction, Angus and coworkers estimated that 751,000 cases of severe sepsis occur in the United States every year.8 Figure 23.1 displays the incidence of severe sepsis in the United States compared to other common diseases. The incidence of severe sepsis currently exceeds the incidence of lung and colon cancer, venous thromboembolic disease, and acquired immune deficiency syndrome (AIDS),8–11 and the incidence is projected to increase by 1.5% per year, resulting in more than 1 million cases of severe sepsis annually by the year 2020.8 The incidence of sepsis and septic shock is known to be increasing because of a longer lifespan for patients with severe chronic medical conditions that predispose them to acquiring sepsis. This includes an increase in the number of immunocompromised patients in the community, number of infections caused by resistant organisms, increased use of intravascular catheters, and aging of the population.8 Figure 23.1 Incidence (cases per 100,000 population) of severe sepsis in the United States compared to four high-profile diseases.8–11 AIDS, acquired immune deficiency syndrome; VTE, venous thromboembolic disease. Sepsis is the leading cause of death among critically ill patients12 and is responsible for as many deaths annually in the United States as acute myocardial infarction.8 Figure 23.2 displays control arm mortality rates in septic shock clinical trials.1 In a recent large multicenter registry study, septic patients with both arterial hypotension and severe lactic acidosis experienced a 46% mortality rate, whereas the mortality rate for arterial hypotension or severe lactic acidosis alone was 37% and 30%, respectively.13 Overall, severe sepsis in general ranks as the tenth leading cause of death in the United States, with 215,000 deaths annually and an estimated 30% in-hospital mortality rate.8,14 Figure 23.3 displays the mortality rate for severe sepsis compared to other high-profile diseases that may require critical care (acute ischemic stroke, acute myocardial infarction, and trauma).8,15–17 The apparent disparity in mortality rates across these diseases may be explained in part by differences in the conventional approach to treatment, as acute ischemic stroke, acute myocardial infarction, and trauma are all typically treated with aggressive interventions in a time-sensitive fashion. Similar to the “golden hour” concept for trauma care that was first recognized more than 30 years ago18 we are now beginning to understand that early aggressive interventions for sepsis can also have an impact on outcome. Figure 23.3 Mortality rate of severe sepsis in the United States compared to three diseases that are treated aggressively with time-sensitive interventions.8,15–17 MI, myocardial infarction. It is also important to recognize that, in addition to a high mortality rate, severe sepsis and septic shock are associated with serious risk of morbidity among survivors.19,20 A systematic review of the literature found that sepsis survivors had substantially diminished quality of life and a sharply reduced long-term survival after typical short-term (i.e., 28-day) outcomes are assessed.19 Among older adults, severe sepsis has been associated with major persistent cognitive impairment and functional disability that could have a substantial impact on those patients’ ability to live independently.20 Taken together, even among patients who survive the sepsis insult, the development of severe sepsis or septic shock can represent a pivotal event in the trajectory of a patient’s life. Septic shock results when infectious microorganisms in the bloodstream induce a profound inflammatory response causing hemodynamic decompensation. The pathogenesis involves a complex response of cellular activation that triggers the release of a multitude of proinflammatory mediators. This inflammatory response causes activation of leukocytes and endothelial cells, as well as activation of the coagulation system. The excessive inflammatory response that characterizes septic shock is driven primarily by the cytokines tumor necrosis factor-alpha (TNF-α) and interleukin 1 (IL-1) that are produced by monocytes in response to an infection. Although TNF-α and IL-1 are central to the pathophysiology of septic shock and act synergistically to induce hypotension in experimental models, a number of other vital mediators are also known to play a major role, including high-mobility group box 1 (HMGB1) protein.21 Another important recent advance in our understanding of septic shock pathophysiology has been identification of the close link that exists between the proinflammatory response of septic shock and activation of the coagulation system (e.g., clinical or subclinical disseminated intravascular coagulation [DIC]).22 Although the systemic inflammatory response of sepsis triggers profound macrocirculatory and microcirculatory changes that impair tissue perfusion, another important mechanism playing a role in the development of acute organ dysfunction in septic shock is apoptosis (programmed cell death). Accelerated apoptosis is known to be a critical pathogenic event in this disease. In addition, certain genetic polymorphisms are becoming recognized as major determinants of susceptibility to infection, as well as risk of death from septic shock. Key steps in the pathogenesis of septic shock are shown in Figure 23.4. Patients with septic shock will typically manifest signs of systemic inflammation including fever or hypothermia, tachycardia, tachypnea, and elevation or reduction of the white blood cell count. Although the absence of arterial hypotension does not necessarily exclude the possibility of subclinical tissue hypoperfusion,23 the hallmark of septic shock is arterial hypotension despite adequate volume resuscitation requiring vasoactive drugs for hemodynamic support. Other signs of potential tissue hypoperfusion may include lactic acidosis, oliguria, encephalopathy, or diminished capillary refill in the extremities. Patients with septic shock typically have multiple organ system dysfunctions; clinical evidence of other organ system dysfunction may range from subtle abnormalities to overt organ failure. Multiorgan system involvement in sepsis may include cardiovascular, respiratory, renal, central nervous system, hepatic, metabolic, or hematologic dysfunction. Respiratory system dysfunction manifests as acute lung injury or, in the most extreme cases, the acute respiratory distress syndrome (ARDS). Sepsis-induced renal dysfunction typically manifests with oliguria and may progress to acute renal failure requiring dialysis. Central nervous system dysfunction will manifest as encephalopathy, which may range from mild cognitive impairment to overt coma. Cholestasis is a common manifestation of hepatic dysfunction in sepsis, but in the presence of severe shock, ischemic hepatitis (“shock liver”) may occur. Metabolic derangements of septic shock include a loss of glycemic control (hyper- or hypoglycemia) as well as metabolic acidosis. Septic shock is commonly associated with a consumptive coagulopathy, which is likely present in almost all patients at least subclinically,24 but may also manifest clinically with thrombocytopenia, prolongation of the prothrombin time, or in the most severe cases, overt DIC. The multiple organ dysfunction associated with septic shock is not only a critical event in the pathogenesis of this disease, but is also closely linked with mortality rate.8,25,26 There is an approximate 20% increase in septic shock mortality rate with each additional organ system that fails.8 Early evidence of organ failure is an especially strong predictor of death.26,27 Early improvement in organ function (e.g., 0-24 hour improvement in the Sequential Organ Failure Assessment [SOFA] score28,29) is closely related to sepsis survival, whereas later improvement after the first 24 hours has little predictive value.27 These data, garnered largely from observational studies as well as placebo arms of interventional trials, support the concept that aggressive therapy for sepsis to reverse (or prevent the development of) acute organ system failure within the first 24 hours is closely associated with eventual outcome. The hemodynamic profile of septic shock is the most complex hemodynamic profile of all shock etiologies (Fig. 23.5). What sets septic shock apart from other causes of circulatory shock is the fact that there may be multiple different mechanisms of circulatory shock occurring simultaneously.1,30 Septic shock may have features of (1) hypovolemic shock (poor cardiac filling secondary to severe systemic capillary leak and increased venous capacitance), (2) cardiogenic shock (infection-induced myocardial depression), and (3) distributive shock (arteriolar vasodilation with tissue hypoperfusion in the face of an adequate cardiac output).1 The release of proinflammatory mediators into the circulation causes injury to the integrity of the endothelial cell surface throughout the systemic microvasculature, resulting in severe capillary leak and extravasation of fluid into tissues. Venodilation also compromises venous return. These are major factors in producing hypovolemia in the patient with septic shock. The septic shock patient may have a markedly decreased cardiac preload, especially in the initial phase of therapy. Aggressive resuscitation with intravenous volume expansion modulates the hemodynamic profile of septic shock and allows the patient to achieve a hyperdynamic (i.e., high cardiac output) state.1 The combination of a decreased preload and myocardial depression means that in the early phase of sepsis resuscitation, patients may initially be hypodynamic (i.e., low cardiac output) prior to receiving adequate volume resuscitation. Capillary leak is an ongoing process in the course of septic shock therapy, and therefore hypovolemia may recur later in the course of the disease, even after adequate cardiac filling has been initially achieved. Fluid balance (input of intravenous fluids and output of urine) is an unreliable parameter for assessing adequacy of fluid resuscitation in septic shock. Septic shock is associated with depression of biventricular function with a decrease in the ejection fraction. Ventricular dilation occurs as a compensatory mechanism and raises end-diastolic volume so that stroke volume can be preserved, taking advantage of the Starling principle. When myocardial dysfunction occurs, a high cardiac output can still be achieved in many circumstances because of biventricular dilation, tachycardia, and arteriolar dilatation, as long as the patient is adequately volume resuscitated and does not have a severe cardiac suppression (related either to previously existing cardiac dysfunction or overwhelming sepsis-induced suppression of cardiac systolic function).30 The most important inflammatory mediators that induce myocardial depression are TNF-α, IL-1, and perhaps nitric oxide.31,32 Coronary blood flow is typically normal or increased in septic shock.33 Although coronary blood flow can be diminished by severe arterial hypotension that compromises coronary perfusion pressure (especially if there is preexisting coronary artery disease), myocardial ischemia does not appear to be the causative factor of the depression in myocardial performance. It has been reported that nearly half of patients with septic shock will have echocardiographic evidence of some degree of depression of systolic function, even in the absence of preexisting cardiac disease.34 However, myocardial depression is typically not the predominant feature of the septic shock hemodynamic profile.30 For the majority of patients, aggressive intravascular volume expansion to restore adequate cardiac filling pressures will be enough to achieve a reasonable cardiac output. Septic shock is characterized by peripheral maldistribution of blood flow to tissues such that tissue hypoperfusion abnormalities can persist despite a normal or high cardiac output. This is called “distributive shock.”30 This maldistribution of blood flow may occur at both microcirculatory and macrocirculatory levels. The role of microcirculatory dysfunction is discussed in detail in the next section of this chapter. At the level of the macrocirculation, the autoregulation of blood flow within any single organ system in a normal host can typically maintain effective tissue perfusion over a wide range of systemic pressures (usually ranging from a mean arterial pressure [MAP] of 50 mm Hg to 150 mm Hg). However, there is heterogeneity of blood flow distribution throughout the body in septic shock due to preferential shunting of blood flow to vital organs (e.g., the brain and myocardium). The gastrointestinal tract may be the earliest organ system to experience tissue hypoperfusion in septic shock, as blood is shunted away from the splanchnic circulation in order to preserve blood flow to the brain, myocardium, and skeletal muscles. Ischemic injury to the gastrointestinal tract may be a source of ongoing systemic inflammation in septic shock. The three components of the hemodynamic profile of septic shock are displayed in Figure 23.6. Microcirculatory dysfunction is a pivotal element of the pathogenesis of septic shock.35–38 Although the macrocirculation (heart and large arteries) regulates the global distribution of blood flow throughout the body, it is the microcirculation that controls the delivery of blood flow to tissues. Using intravital videomicroscopy, experimental models of sepsis have demonstrated impaired microcirculatory flow velocity, “stopped-flow” microvessels, increased heterogeneity of regional perfusion, and low density of perfused capillaries.39–42 These derangements can cause marked alterations of oxygen transport including impaired tissue oxygen extraction.43 With the advent of new investigational videomicroscopy techniques, it is now possible to study the microcirculatory network in human subjects with septic shock. Microcirculatory failure appears to be one of the critical pathogenic events in sepsis that is associated with acute multiorgan dysfunction and death.35–38 As these alterations of microcirculatory flow in sepsis can occur in the absence of global hemodynamic perturbations (i.e., absence of low arterial pressure or low cardiac output),36,42,44 derangements of small vessel perfusion are largely a function of intrinsic events in the microcirculation. The causes of microcirculatory flow alterations in sepsis (Fig. 23.7) are multifactorial and include endothelial cell dysfunction, increased leukocyte adhesion, microthrombi formation, rheologic abnormalities, altered local perfusion pressures due to regional redistribution of blood flow, and functional shunting.39,45 The proinflammatory cytokines released in sepsis cause diffuse endothelial cell activation, which is associated with neutrophil activation, expression of endothelial adhesion molecules (i.e., integrins and selectins), and localization of white blood cells to areas of microvascular injury. Pan-endothelial cell injury increases microvascular permeability with the influx of proinflammatory cells into the tissues; this is hypothesized to be an important pathogenic step in the development of acute system organ dysfunction in sepsis. Leukocyte adhesion of white blood cells to the microvessel endothelial surface (primarily in the postcapillary venule) further impedes microcirculatory blood flow. The endothelial injury also triggers the activation of the coagulation cascade via expression of tissue factor on the microvascular endothelium, resulting in fibrin deposition and microvascular thrombosis that may further impair microcirculatory flow. All of these mechanisms collectively contribute to microcirculatory failure in septic shock.37,39 Although septic shock research has classically been focused on macrocirculatory hemodynamic parameters that reflect the distribution of blood flow globally throughout the body, a functional microcirculation is another critical component of the cardiovascular system that is necessary for effective blood flow to tissues. This conceptual framework is depicted in Figure 23.8. Although a shift of research focus from global hemodynamic parameters to indices of microvascular perfusion could potentially be viewed as a major change of direction for septic shock research, the microcirculation likely represents a logical next frontier in the evolution of our understanding of circulatory failure in shock states.37,46 Although there are currently no therapies to specifically target microcirculatory dysfunction in sepsis, going beyond optimization of macrocirculatory hemodynamics and developing new innovative strategies to reverse microcirculatory failure could (in the future) potentially represent a cutting edge method to augment tissue perfusion in sepsis.
Septic Shock
Overview
Historical Perspective
Contemporary Definitions
Epidemiology
Pathogenesis
Clinical Presentation
Hemodynamic Profile of Septic Shock
Hypovolemia
Myocardial Dysfunction
Distributive Shock
Microcirculatory and Mitochondrial Dysfunction
Microcirculatory Dysfunction
Septic Shock