Sensitization of Myofascial Pain Pathways in Tension-Type Headaches
Lars Bendtsen
Rolf Detlef Treede
Recent studies on tension-type headache indicate that the nociceptive input to the central nervous system may be increased because of activation or sensitization of peripheral sensory afferents. In addition, the responses of nociceptive neurons in the central nervous system to their synaptic inputs from peripheral sensory afferents appear to be enhanced in patients with chronic tension-type headache, as suggested by several pain perception studies and pharmacologic studies. Sensitization of second- and third-order neurons in the central nervous system may be induced by the barrage of nociceptive impulses from the periphery. In this way, both peripheral and central sensitization may play a role for initiation and maintenance of tension-type headache (Table 70-1). Recent studies demonstrate that treatment with drugs that counteract sensitization has an analgesic effect in tension-type headache. The evidence for sensitization of myofascial pain pathways in tension-type headache is discussed.
PERIPHERAL FACTORS
The most prominent clinical finding in patients with tension-type headache is a considerably increased tenderness to palpation of pericranial myofascial tissues (19,22,24). The increased pericranial tenderness has been found both in patients with episodic and in patients with chronic tension-type headache (18,22) and both during and outside headache (16,23). The tenderness seems to be uniformly increased throughout the pericranial region and both muscles and tendon insertions have been found excessively tender (10,13,19,22) (Fig. 70-1). In addition, it has been demonstrated that the pericranial tenderness is positively associated with both the intensity and the frequency of tension-type headache (19) and with muscle hardness (1).
What could be the pathophysiologic basis for the possible pain originating in the myofascial tissues? Under normal conditions, myofascial pain is mediated by thin myelinated (Aδ) fibers and unmyelinated (C) fibers, and the thick myelinated (Aα and Aβ) fibers normally mediate innocuous sensations (31). Various noxious and innocuous events such as mechanical stimuli, ischemia, and chemical mediators could excite and sensitize Aδ-fibers and C-fibers (26) and thereby play a role for the increased tenderness in tension-type headache.
The role of the first two events—mechanical strain and ischemia—has been extensively studied in tension-type headache. Numerous electromyographic (EMG) studies using surface electrodes have demonstrated that muscle activity is only slightly increased in tension-type headache (16). However, it has been reported that EMG activity is significantly increased in small localized areas of the muscle, the so-called myofascial trigger points (15). Continuous activity in a few motor units over long time could be sufficient for excitation or sensitization of peripheral nociceptors (7), but the findings by Hubbard and Berkoff (15) have not yet been reproduced by other groups. Muscle tenderness and hardness at tender muscle sites could also result from a local contracture (i.e., shortening of the contractile apparatus without action potentials in the muscle fibers) rather than normal contraction of motor units (33). This mechanism would explain the lack of EMG abnormalities in tension-type headache, but the mechanisms of peripheral nociceptor activation by a contracture have not yet been studied in enough detail (27). By use of the elegant microdialysis technique, Ashina et al. (5) demonstrated that lactate levels in a tender site in the trapezius muscle did not differ between patients and healthy subjects during rest and static exercise, ruling out muscle ischemia in these patients. Thus, it can be concluded that the muscle pain in tension-type headache is not caused by
excessive muscle contraction and muscle ischemia. However, it cannot be excluded that a locally increased muscle tone without EMG activity (contracture) may result in microtrauma of muscle fibers and tendon insertions or that excessive activity in a few motor units may excite or sensitize peripheral nociceptors.
excessive muscle contraction and muscle ischemia. However, it cannot be excluded that a locally increased muscle tone without EMG activity (contracture) may result in microtrauma of muscle fibers and tendon insertions or that excessive activity in a few motor units may excite or sensitize peripheral nociceptors.
TABLE 70-1 Potential Mechanisms of Enhanced Pain Sensitivity (Hyperalgesia) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Peripheral muscle afferents could be activated and sensitized by endogenous substances such as serotonin and bradykinin (26). Recently, Mork et al. demonstrated that when a combination of the endogenous substances bradykinin, serotonin, histamine, and prostaglandin E2 was slowly infused into the trapezius muscle, patients with frequent episodic tension-type headache developed more pain (29) and tenderness (30) than healthy controls. Concomitant psychophysical measures indicated that peripheral sensitization of myofascial sensory afferents was responsible for the muscular hypersensitivity in these patients (30). However, Ashina et al. (6) demonstrated that the in vivo interstitial concentrations of adenosine 5-triphosphate, glutamate, glucose, pyruvate, urea, and prostaglandin E2 in tender muscles during rest and static exercise did not differ between patients with chronic tension-type headache and healthy controls. The authors concluded that tender muscle sites in these patients are not sites of ongoing inflammation.
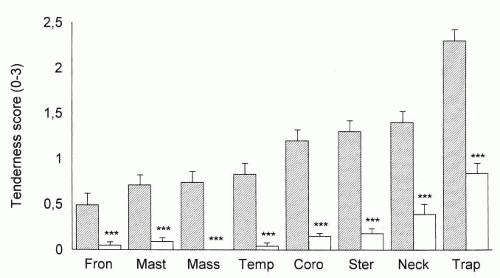 FIGURE 70-1. Local tenderness scores (mean ± SE) at eight pericranial locations in 40 patients with chronic tension-type headache (hatched bars) and in 40 healthy controls (open bars). The patients had significantly more tenderness than the controls at all locations. Abbreviations: Fron, frontal muscle; Mast, mastoid process; Mass, masseter muscle; Temp, temporal muscle; Coro, coronoid process; Ster, sternocleidomastoid muscle; Neck, neck muscle insertions; Trap, trapezius muscle. ★★★P ≤ 0.0002. (Reproduced from Bendtsen L, Jensen R, Olesen J. Decreased pain detection and tolerance thresholds in chronic tension-type headache. Arch Neurol. 1996;53:373-376, with permission.) |
To summarize, pericranial myofascial tenderness and muscle hardness are frequently observed in tension-type headache. These findings are similar to trigger points in other myofascial diseases (35). Some studies indicate that the increased myofascial pain sensitivity in tension-type headache may be caused by activation or sensitization of peripheral nociceptors. However, firm evidence for peripheral abnormalities as a cause of myofascial tenderness is still lacking.
CENTRAL FACTORS
The increased myofascial pain sensitivity in tension-type headache could also be caused by central factors, such as (a) sensitization of second-order neurons at the level of the spinal dorsal horn/trigeminal nucleus, (b) sensitization of supraspinal neurons, and (c) decreased antinociceptive activity from supraspinal structures. The measurement of pain sensitivity to various types of stimuli applied to various parts of the body have provided important information about the nociceptive system in tension-type headache. Pain detection thresholds have been reported normal in patients with episodic tension-type headache (12,14,17,19) except for a recent study in patients with frequent episodic tension-type headache (30). In contrast, pain detection and tolerance thresholds have been found decreased in patients with chronic tension-type headache in all studies performed with sufficient sample size (10,20,21,32) (Fig. 70-2) (Table 70-2,).
Related posts:







Full access? Get Clinical Tree


