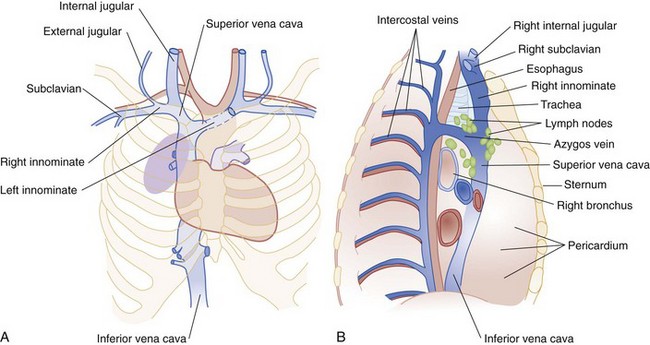
Chapter 123 Oncologic emergencies embody an extensive range of illnesses that can occur at any time during the course of malignant disease. Some oncologic emergencies are insidious and develop during months; others are manifested in hours and can lead to paralysis and death.1 Prompt, accurate diagnosis and appropriate treatment of oncologic emergencies can improve the quality of life dramatically in patients with cancer. With timely intervention, many of these patients can return to their previous level of function and independence. In addition, a reversible life-threatening emergency can occur in a patient with an underlying malignant neoplasm that is otherwise highly treatable or even curable, making identification and management of the oncologic emergency a potentially lifesaving action. Cancer remains the second leading cause of death in the United States. It is estimated that 1,529,560 men and women (789,620 men and 739,940 women) will be diagnosed with and 569,490 men and women will die of cancer of all sites in 2010.2 The most commonly diagnosed new cancer is prostate cancer in men and breast cancer in women. The second most commonly diagnosed new cancer in both sexes is lung cancer. The most common cause of cancer death for both sexes is lung and bronchial cancer.3 Worldwide, the most commonly diagnosed new cancer and most common cause of cancer death is lung and bronchial cancer in men and breast cancer in women.4 The most common malignant neoplasm of childhood is leukemia, followed by brain tumors and lymphoma.5 In 2003, it was estimated that the lifetime risk for development of cancer was 1 : 2 for men and 1 : 3 for women.5 Most cancer patients will experience at least one emergency during the course of their disease, and emergency physicians are increasingly managing complications related to cancer, although definitive therapy for an oncologic emergency is often multidisciplinary, involving surgeons, radiation oncologists, medical oncologists, and other medical and social specialists. Changing trends in cancer have produced an increased number of emergency department (ED) visits secondary to cancer and its complications (Box 123-1).6 In fact, a study reported that about 40% of cancer patients had visited the ED in the last 2 weeks of life.7 Therefore, the emergency physician should be well versed in oncologic emergencies. However, many factors can hinder the identification and management of oncologic emergencies in the ED (Box 123-2). This chapter focuses on the most common oncologic emergencies: fever and neutropenia, superior vena cava syndrome, acute tumor lysis syndrome, hyperviscosity syndrome, hyperuricemia, hypercalcemia, neoplastic cardiac tamponade, and spinal cord compression. Fever is defined as a single oral temperature in excess of 38.3° C (101.3° F) or a sustained temperature of 38° C (100.4° F) for more than 1 hour.8 Fever in the cancer patient can be caused by inflammation, transfusions, antineoplastics, antimicrobials, and tumor necrosis. Although fever can be secondary to malignant disease with a significant tumor burden, fever occurring in cancer patients more commonly has an infectious origin (55-70%). Neutropenia, defined as an absolute neutrophil count (ANC) of less than 500 cells/mm3 or less than 1000 cells/mm3 with predicted decrease to less than 500 cells/mm3, will assist in determining the need for empirical antibiotics and a more aggressive approach to treatment of a febrile cancer patient.9 ANC can be calculated from white blood cell (WBC) and polymorphonuclear (PMN) cell counts as follows: Fever in the neutropenic cancer patient is one of the most common complications related to chemotherapy treatment. It should be presumed to have an infectious origin and thus constitutes a medical emergency. Use of early empirical antibiotic therapy has resulted in a decrease in mortality in patients receiving chemotherapy.8 Many factors predispose the neutropenic patient to infection and sepsis: prolonged bed rest; clinical deterioration; nutritional compromise; disruption of mucous membranes and skin barriers; indwelling catheters; and central nervous system (CNS) dysfunction secondary to cancer, sedatives, opiates, and psychotropic medications. An undetected and untreated infection can be rapidly fatal in this population of patients. Therefore early administration of broad-spectrum empirical antibiotic therapy is recommended in all febrile, neutropenic patients. Consultation with the oncologist and infectious disease specialist will help categorize the risk for patients and aid in the selection of antibiotics based on local resistance patterns (Box 123-3). While antibiotics are being started, diagnostic testing includes a complete blood count with differential cell count, platelet count, prothrombin time, partial thromboplastin time, blood chemistries, urinalysis, and analysis of any accessible sites suggestive of infection. Two sets of blood culture specimens are recommended for aerobic, anaerobic, and fungal growth. If an indwelling catheter is present, at least one set of blood culture specimens should be obtained from the device lumen as well as from a peripheral vein. A routine chest radiograph is obtained at most institutions. However, studies show that a chest radiograph is not necessary in patients with no respiratory symptoms and normal physical examination findings.9 Urine should be sent for culture even in the absence of pyuria. However, the use of sputum culture and Gram’s stain has become controversial because of inconsistencies in collection and preparation that have led to false-negative and false-positive results. Some oncologists discourage rectal temperature readings for patients with neutropenia because of the risk of tearing the rectal mucosa and establishing a potential nidus for disseminated infection. However, this has not yet become the standard of care and may vary among institutions. An indwelling nasogastric tube predisposes the neutropenic patient to sinusitis. When imaging for suggested sinusitis is required, computed tomography (CT) is preferred to sinus films. A lumbar puncture, preceded by head CT, is indicated when symptoms point to the CNS.10 Some authorities have recommended surveillance cultures of the stool, nose, and throat. This recommendation is not universally accepted and is generally not indicated in patients with solid tumors. Despite an intensive and comprehensive evaluation, an infectious cause is initially substantiated in only 30% of febrile, neutropenic patients.11 Overall, approximately 85% of the initial pathogens isolated in febrile neutropenic patients are bacterial, and of these, 60 to 70% are gram-positive pathogens. Gram-negative bacilli, particularly Pseudomonas aeruginosa, were the most common pathogens until the 1980s. However, the administration of prophylactic antibiotics primarily active against gram-negative pathogens during chemotherapy, the widespread use of indwelling venous catheters, and the newer chemotherapy regimens have led to an increase in gram-positive pathogens.12 In an attempt to prevent these infections, oncologists may initiate antimicrobial prophylaxis with trimethoprim-sulfamethoxazole (Bactrim) or quinolones for immunosuppressed patients before development of fever.11 In addition, recombinant human granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor are used to stimulate rapid increase in granulocytes in neutropenic patients in an effort to decrease the duration and degree of neutropenia and immunosuppression. Local resistance patterns are used to guide treatment. Patients are risk stratified and then treated accordingly. Patients with fever who appear in good condition are considered at low risk. Patients with fever who have severe neutropenia, appear ill, and are expected to have a protracted course are at high risk.13 In the initial evaluation and management of the febrile cancer patient, one must take into account the particular underlying malignant neoplasm, prior use of antimicrobial therapy, and how the degree of treatment has affected the host’s immunologic compromise. For example, in acute leukemia, normal circulating neutrophils and monocytes are largely replaced by blast cells, which do not function well in the phagocytosis and killing of bacterial and fungal agents. Chemotherapeutic agents and irradiation exacerbate or potentiate the underlying defect in already compromised host defenses. Corticosteroids impair granulocyte and mononuclear cell mobilization in leukemic patients. Patients with severely compromised host defenses and those in whom fever is accompanied by an increase in respiratory rate, change in mental status, agitation or apprehensiveness, and hemodynamic instability should be urgently treated. Significant advances in the antimicrobial armamentarium have been made in the past 10 years with the development of broad-spectrum single agents such as the carbapenems (imipenem-cilastatin, meropenem) and the third- and fourth-generation cephalosporins (ceftazidime, cefepime). These agents, when investigated as monotherapy in neutropenic, febrile patients, have been found to be as effective as a dual-drug combination of an antipseudomonal penicillin (ticarcillin, carbenicillin, or piperacillin) plus an aminoglycoside (gentamicin or tobramycin). Furthermore, single-drug therapy is associated with fewer adverse effects.8 Amikacin is generally reserved as a second-line aminoglycoside for isolates that demonstrate aminoglycoside resistance. Antifungal and antiviral agents are not usually indicated during initial therapy, although they are becoming increasingly prevalent. Antifungal therapy is recommended if there is no improvement within 3 days of treatment.8 Box 123-3 summarizes current recommendations for antimicrobial therapy for fever in neutropenic cancer patients. The drug most commonly used for treatment of gram-positive bacteria is vancomycin.8 Use of empirical vancomycin is indicated in the following circumstances: • Clinically suspected catheter infections • Known colonization with penicillin- and cephalosporin-resistant pneumococci or methicillin-resistant S. aureus • Blood cultures positive for gram-positive bacteria before final identification and susceptibility testing • Hypotension or other evidence of cardiovascular impairment Several clinical trials validate the outpatient management of selected patients older than 16 years with neutropenic fever. These patients must be at low risk for serious infection and must have close follow-up and unrestricted access to health care professionals.14 The Multinational Association for Supportive Care in Cancer has introduced a prediction tool to assess patients suitable for outpatient therapy that accounts for burden of illness and social factors.14 Contraindications to outpatient therapy are as follows: Colony-stimulating factors are used in prophylaxis of neutropenic fever. However, their routine use as an adjunct to antibiotics in the treatment of neutropenic fever is controversial and currently recommended only in select, high-risk patients.15 Initiation of treatment should be made in consultation with the patient’s oncologist. Superior vena cava syndrome (SVCS) is an acute or subacute process caused by the obstruction of blood flow through the superior vena cava (SVC) secondary to compression, infiltration, or thrombosis. It occurs in approximately 1500 persons in the United States annually.16 Malignant disease is the most common cause of SVCS and currently accounts for 60 to 85% of cases.17 It is estimated that 2 to 4% of all cancer patients will have SVCS; in fact, SVCS is often the initial presenting sign of the tumor, and it is a poor prognostic marker.18 The most common cancers associated with SVCS are non–small cell lung cancer (50%), small cell lung cancer (25%), and lymphoma and metastatic lesions (10%).17 However, benign causes of SVCS, such as intrinsic thrombus, are gradually increasing, accounting for 20 to 40% of all cases owing to more frequent use of intravascular devices.19 Other common nonmalignant causes are goiter, pericardial constriction, primary thrombosis, idiopathic sclerosing aortitis, tuberculous mediastinitis, fibrosing mediastinitis (histoplasmosis and methysergide treatment), arteriosclerotic or (rarely) luetic aneurysm, nephritic syndrome, and indwelling central venous catheters. In contrast to SVCS in the adult population, SVCS in pediatric patients is most often iatrogenic secondary to indwelling catheters, ventriculoperitoneal shunts, and complications of cardiovascular surgical procedures. Knowledge of the unique anatomic relationship of the SVC in the anterior superior mediastinum is crucial to understanding of the clinical presentation of SVC obstruction. The SVC is easily compressed by any of its contiguous structures (trachea, heart, aorta, azygos vein, and paratracheal and bronchial lymph nodes). This compression can produce a constellation of symptoms that reveal the likely site of the pathophysiologic process (Fig. 123-1). The SVC arises from the innominate veins, which in turn arise from the internal jugular and subclavian veins. The azygos vein, the last main auxiliary vessel of the SVC, drains blood from the chest wall. As a consequence of this anatomic relationship, if the SVC is blocked above or at the entrance of the azygos, blood may bypass and decompress the obstruction through the chest wall collateral vessels and rejoin the SVC through the azygos. If the obstruction falls below or at the entrance of the azygos, blood must traverse in a retrograde manner down the azygos and other chest wall veins to reach the drainage area of the inferior vena cava and subsequently cause more prominent symptoms. SVCS symptoms develop during a period of 2 weeks in about one third of patients and in a longer time in others.16 SVCS causes edema of the upper body, particularly of the head and neck. Early signs may include periorbital edema, conjunctival suffusion, and facial swelling, which will be most evident in the early morning hours and subside by midmorning. This edema may be significant enough to compromise the lumen of the trachea, causing stridor and dyspnea, or of the esophagus, causing dysphagia. One of the most common presentations in SVCS is dyspnea and swelling of the face, trunk, and upper extremities. Cough, dysphagia, and chest pain are less commonly reported, each occurring in approximately 20% of patients. With increasing impedance to blood flow, the full-blown syndrome begins to be manifested with thoracic and neck vein distention (67% and 59%, respectively), facial edema (56%), tachypnea (40%), tightness of the shirt collar (the Stokes sign), plethora of the face, edema of the upper extremities, and cyanosis.16 Other concerning symptoms are neurologic, such as headaches, confusion, and even coma, suggesting cerebral edema, ischemia, or both. Although cerebral edema is rare, it can be fatal. The usual course of SVCS is that collaterals develop, and symptoms improve when this occurs.17 There is little evidence in the literature to substantiate the notion of untreated SVC obstruction as immediately life-threatening, as was once believed, except when it occurs with respiratory compromise or cerebral edema.20 Survival in patients with SVCS depends mainly on the course of the underlying disease. The clinical diagnosis of SVC obstruction is mimicked by a few other clinical entities, most noteworthy of which are pericardial tamponade and heart failure; both can usually be excluded by physical examination and bedside cardiac ultrasound examination. The chest film is abnormal in 84% of patients with SVCS; the most common abnormalities are mediastinal widening (64%) and pleural effusion (26%).16 It reveals a mass in nearly 10% of patients. When superior mediastinal mass is present, 75% are on the right side, and in approximately 50% of patients, the masses are combined with pulmonary lesions or hilar adenopathy. Pleural effusion is an associated finding in approximately 20 to 25% of patients and is customarily found in the right hemithorax. CT of the chest with intravenous administration of contrast material is the most useful imaging study to evaluate the SVC.16 History and physical examination combined with the CT chest scan with intravenous contrast enhancement will help differentiate between intrinsic and extrinsic compression of the SVC. The presence of collateral vessels with compression of the SVC is a reliable indicator of SVCS. Venography is relatively contraindicated because of its concomitant bleeding complications. It is generally warranted only during placement of a stent or surgery. MRI may be useful in patients who cannot receive an intravenous contrast agent. Invasive diagnostic procedures, including bronchoscopy, mediastinoscopy, scalene node biopsy, and limited thoracotomy, are commonly used to establish the diagnosis and extent of the disease. SVCS is considered an immediately life-threatening oncologic emergency only if CNS symptoms are present. If a true emergency exists, a stent can be emergently placed in the SVC or radiation therapy can be used.21 In all other cases, once the clinical diagnosis is entertained, a tissue biopsy specimen should be obtained promptly before treatment decisions are made. Although supportive therapy may be instituted to alleviate symptoms, definitive therapy is dependent on the histologic diagnosis. The American College of Chest Physicians and the National Comprehensive Cancer Network both recommend consideration of radiation therapy, stent placement, or both. Historically, emergent radiation therapy was the treatment of SVCS. Currently, this is recommended only emergently for patients who present with stridor due to central airway obstruction or severe laryngeal edema. In an attempt to relieve the obstruction, current management uses radiation therapy for cancers responsive to this treatment and chemotherapy in other cancers because of the increased incidence of tumor sensitivity to newer antineoplastic agents. Complete relief of symptoms is achieved with chemotherapy in approximately 80% of patients with non-Hodgkin’s lymphoma or small cell lung cancer and in 40% of those with non–small cell lung cancer.16 However, temporizing measures that alleviate symptoms related to vascular compression should be rapidly instituted. Other current management approaches include percutaneous transluminal stent placement and bypass surgery.21 Placement of an intravascular stent to bypass the obstruction is particularly useful in patients requiring urgent intervention before tissue diagnosis because of severe symptoms such as respiratory distress. Stent placement is also useful for patients whose cancer is minimally responsive to chemotherapy or radiation therapy and for those patients with a thrombus associated with an indwelling catheter. Surgical bypass grafting is infrequently used to treat SVCS but may be useful in cancers resistant to chemotherapy and radiation therapy. The prognosis for patients treated for SVCS depends on the tumor type, with better survival rates in patients with lymphoma than in patients with bronchogenic carcinoma. Median life expectancy of patients with malignant causes of SVCS is 6 months, but this varies widely by the underlying malignant condition.20
Selected Oncologic Emergencies
Perspective
Fever

Clinical Features
Diagnostic Strategies
Differential Considerations
Management
Superior Vena Cava Syndrome
Clinical Features
Ancillary Evaluation
Management





Full access? Get Clinical Tree


