186 Sedatives and Hypnotics
 Rationale for Sedative Use in the Intensive Care Unit
Rationale for Sedative Use in the Intensive Care Unit
Medications are commonly administered to critically ill patients to diminish fundamental activities of the central nervous system (CNS) such as wakefulness, memory, and control of voluntary muscle contraction, and to minimize unpleasant symptoms such as dyspnea, pain, anxiety, and fear. Medications are most often used for these purposes in the management of mechanically ventilated patients; they are more likely to receive sedative-analgesics, and in higher doses, than nonintubated patients.1 Paradoxically, most intensive care unit (ICU) patients who receive these potent CNS-active medications are not suffering from acute neurologic diagnoses such as stroke, seizure, or infection. Therefore this chapter focuses on sedative use in critically ill patients who may have toxic-metabolic encephalopathy (e.g., delirium) or no CNS abnormalities at all.
The expression “sedation” or “sedative medications” encompasses elements of sedation, hypnosis, amnesia, analgesia, and muscle relaxation. These words have discrete but related meanings. Sedatives create a state of calmness or lack of excitability without necessarily decreasing awareness. Hypnotics and general anesthetics induce sleep or, more precisely, create the appearance of sleep by reducing the level of consciousness, arousability, or awareness. Amnestics impede new memory formation, whereas analgesics reduce the symptom of pain by peripheral or central mechanisms. Excessive skeletal muscle contraction or motor activity is a major manifestation of agitation which, along with level of consciousness, is the primary observable behavior measured by many sedation scales.2 Antipsychotics and neuroleptics ameliorate disorganized thinking and inappropriate behavior. Most “sedative” medications have clinical effects in several of these categories. For instance, a drug may have both sedative and hypnotic properties, or both analgesic and hypnotic effects, or antipsychotic and sedative effects. Although no one sedative has a completely specific effect, medications typically have greater effects in one of the categories, and the thoughtful intensivist can prescribe medication combinations that maximize desired effects while minimizing unwanted effects. Importantly, given in higher doses, almost all the medications described in this chapter decrease the level of consciousness and reduce unwanted skeletal muscle activity.
 Goals of Sedation for Patients in Intensive Care Units
Goals of Sedation for Patients in Intensive Care Units
Table 186-1 lists 15 indications for administration of sedative and analgesic medications to critically ill patients. The clinician should mentally compare the number of possible indications for use of sedative-analgesics in ICU patients with an analogous list for other common ICU medications. For example, antibiotics have two indications, to prevent or treat infections, and gastric acid–reducing medications have two indications, to prevent or treat gastrointestinal bleeding and improve symptoms of esophageal reflux. Much of the art of sedating ICU patients lies in determining which of the many indications applies to the individual patient on a given day and communicating that rationale to other caregivers.
TABLE 186-1 Indications for Administering Sedative-Analgesic Medications to Critically Ill Patients
| Indication | Comment |
|---|---|
| Minimize ventilator dyssynchrony | Poor synchrony may lead to hypoxemia and dyspnea and is distressing to caregivers. Ventilator adjustment may improve synchrony without medications. |
| Reduce dyspnea associated with severe acute respiratory failure | Reducing minute ventilation to avoid barotrauma can cause severe dyspnea. Tachypnea with short expiratory times can lead to increased auto-PEEP and hypotension. |
| Increase tolerance of intubation | A translaryngeal endotracheal tube can cause pain, gagging, and reflexive biting. |
| Reduce anxiety | Acute severe illness possibly leading to disability or death may produce unwanted psychological distress. |
| Reduce recall of ICU symptoms | Recall of distressing symptoms such as severe dyspnea, terror, restraint, or pain can have long-term psychological consequences.32 |
| Reduce stress response and oxygen consumption | Reducing unwanted motor activity or respiratory effort can decrease total-body oxygen consumption by 15%.87 |
| Reduce elevated intracranial pressure | Coughing, straining, or excessive ventilator dyssynchrony can cause dangerous spikes in intracranial pressure. |
| Reduce pain | Surgical or traumatic wounds, catheter and tube placement, and immobilization usually cause pain. |
| Prevent removal of life-support technology | Removal of an endotracheal tube or vascular catheter can cause death within minutes. |
| Induce sleep | ICU patients often have abnormal chronobiology cycles associated with delirium and impaired immune function. Commonly used sedatives have not been shown to restore normal sleep brainwave patterns. |
| Increase efficiency of patient care delivery | Constant visual observation and verbal and tactile patient reassurance may not be possible in understaffed units. |
| Protect caregivers from violent behaviors | Confused patients can violently assault caregivers. |
| Adjunct during pharmacologic paralysis | Awareness during pharmacologic paralysis is inhumane and can have long-term psychological consequences. |
| Treat delirium | Antipsychotics may reduce disorganized thought processes or behavior while the underlying cause of the delirium is treated. |
| Family considerations | Repeatedly observing the distress of a loved one can cause anguish in family members, who may request that additional sedatives be given to the patient.27 |
ICU, intensive care unit; PEEP, positive end-expiratory pressure.
 Epidemiology of Sedative Use in the Intensive Care Unit
Epidemiology of Sedative Use in the Intensive Care Unit
Two-thirds of patients requiring mechanical ventilation receive sedative medications.3,4 International practice surveys show that BZDs or propofol are the most common sedatives selected and are often combined with opioids, although the choice of opioid (e.g., morphine, fentanyl, or sufentanil) varies among countries and institutions. A study of 174 ICUs in 2007 reported that over 50% of ventilated patients received intravenous (IV) sedation: 82% received propofol, 31% received a BZD, and 4% received dexmedetomidine. Intravenous opiates were used more commonly with BZDs (70.1%) than with propofol (23.9%).5 Continuous infusion therapy was associated with a markedly prolonged duration of mechanical ventilation and longer time to achieve important weaning landmarks.4,6 In a clinical trial that enrolled patients with adult respiratory distress syndrome, sedatives were administered during 70% of ICU patient-days.7 Contrary to clinicians’ expectations, two studies showed that ventilating patients with small tidal volumes to avoid ventilator-induced lung injury was not associated with an increase in sedative exposure.8,9 Despite general practice surveys showing widespread use of sedatives, there are hospitals that have successfully managed ventilated patients with a “minimal-to-no-sedation” policy.10
What are the clinical consequences of widespread use of potent sedatives? Because there are numerous causes of decreased consciousness in critically ill patients, it is difficult to estimate the independent effect of sedative medications on patients’ clinical status. In one study, one-third of subjects were in an unarousable or deeply sedated state, one-third were in a state of moderate to light sedation, and one-third were in an alert and calm state.11 The correlation between sedation level and amount of sedative medication received during the 8 hours before the assessment was weak (r = −0.13 to −0.32) across different medication classes. These results suggest several mutually compatible possibilities: (1) factors (e.g., organ failure-associated encephalopathy) other than medications influence sedation scale measurements, (2) the pharmacologic effects of sedatives accumulate over days rather than hours, and/or (3) dose-response relationships are nonlinear. Another study showed that mechanically ventilated patients were unarousable to tactile stimulation 32% of the time, yet were rated by their nurses as “oversedated” less than 3% of the time.12
Conditions Requiring Sedation
Determining the specific reasons for administration of sedative medications is problematic in clinical studies, but the question can be approached by determining the prevalence of the syndromes, symptoms, or behaviors that may lead to sedative intervention. Some 20% to 60% of patients recall having significant pain during their ICU stay.13–15 Therefore caregivers should consider pain as the most likely cause when patients show signs of distress or agitation. Delirium was objectively diagnosed in 83% of ICU patients at some time during their illness.16 However, ICU delirium is often hypoactive, manifested as inattention rather than agitation, and therefore may not lead to sedative administration. Because the expected effects of sedative medications can mimic symptoms of delirium (e.g., inattention, confusion, fluctuating level of consciousness), studies that link administration of sedatives such as BZDs to persistent delirium should be interpreted cautiously.17
According to one study, agitated behavior, as documented by nursing notes, occurred in 71% of ICU patients, and two-thirds of the episodes were judged as being severe or dangerous. In this study, caregivers often identified three or more factors they believed contributed to the agitated episode.18 However, another study of mechanically ventilated patients detected agitation in less than 5% of 1833 separate assessments.11 The low prevalence of agitation in this study may have occurred because agitation was assessed only during a narrow time interval. These results suggest caregivers intervene quickly when patients are agitated, even if the underlying cause or causes are difficult to identify. Caregivers probably respond quickly because agitation is so visibly apparent and is associated with numerous adverse clinical events.
Anxiety during the acute illness is commonly recalled by ICU survivors,14 although a sample of 192 awake mechanically ventilated ICU patients reported a mean anxiety level during intubation that was only slightly higher than that of nonintubated patients assessed on a general medical-surgical ward.19 These results imply that caregivers should not assume that all mechanically ventilated patients require treatment with anxiolytic medications.
ICU patients recall sleep disruption as a major problem during their ICU stay. Polysomnograms demonstrated that because of frequent arousals and severely fragmented sleep architecture, only 40% of critically ill patients exhibited even brief periods of normal rapid eye movement (REM) sleep.20 The other 60% of patients, who also as a group received more sedative medications, showed no evidence of electrophysiologic sleep, but rather had electroencephalograms (EEGs) consistent with diffuse encephalopathy and coma. Sleep deprivation has been associated with a decrease in quality-of-life measures and increased incidence of complications such as neurocognitive dysfunction and delirium.21 Environmental interventions to improve sleep quality (e.g., noise and light abatement) have not been successful in improving EEG-documented sleep.22 Pharmacologic interventions such as increasing propofol infusion rates at night can generate a diurnal pattern of patient arousability, but there is no evidence that propofol or any other widely used ICU sedative creates restful physiologic sleep for ICU patients.23 In a small trial using wrist actigraphy to estimate sleep quality, nighttime administration of melatonin improved sleep in ICU patients with respiratory failure.24 Newer nonbenzodiazepine hypnotic agents such as zolpidem, zopiclone, and gaboxadol have not been studied in critically ill ICU patients to determine whether they improve disordered sleep or improve outcomes.21 The rationale for administration of additional sedation at night is often conceptualized as “resting” patients in preparation for weaning trials in the morning. However, there are few data to support this concept, and one study showed that the reintubation rate was greater among patients with lower sedation scores (e.g., greater sedation) during the shift interval before the planned extubation.11
Dyspnea is an important symptom to consider, because many ICU patients have respiratory failure requiring mechanical ventilation.25 Dyspnea is a complex symptom that arises from both acute and chronic cardiopulmonary conditions but also from constraints imposed by mechanical ventilators. Excessively small tidal volumes, short expiratory times, or slow inspiratory flow rates can worsen dyspnea and lead to potentially injurious ventilator dyssynchrony. A ventilatory mode that allows spontaneous respiratory efforts throughout the respiratory cycle was found to decrease sedation requirements in patients with acute respiratory distress syndrome (ARDS).26 Opiates are considered first-line medications to relieve dyspnea. However, in patients with communication difficulties, caregivers cannot easily determine whether a little dyspnea is causing a lot of anxiety (in which case BZDs are preferred) or a lot of dyspnea is causing a little anxiety (in which case opiates are preferred).27 ICU personnel may choose to use continuous-infusion opiate therapy for almost all ventilated patients, reasoning that most critically ill patients are dyspneic or in pain or both.28
Although detailed investigations are lacking, the severity of respiratory failure is likely positively associated with aggregate dosing of sedatives. However, the number of ICU patient-days with severe respiratory failure (e.g., high positive end-expiratory pressure, high inspired oxygen fraction, prone positioning) represents a minority of all patient ventilator days. For example, among patients with acute respiratory failure due to exacerbation of chronic obstructive pulmonary disease or ARDS, 40% of time on the ventilator was spent in the weaning phase.29 Similarly, one-third of all ventilated patients examined during a single cross-sectional time point were in the weaning phase.25 Therefore, as patients’ respiratory support requirements lessen, sedation also should be weaned. When patients become more alert, caregivers may have heightened concern for inadvertent removal of life-support technology. Although sedatives or restraints offer no guarantee against “treatment interference,”30 fewer than 2% of ventilated patients had unexpected extubations that required reintubation.29
Sedatives, especially BZDs, may be given to induce anterograde amnesia of the presumably psychologically stressful ICU experience.31 This indication is supported by results from an observational study of ARDS survivors. In this study, patients who recalled a greater number of traumatic experiences from the period when they were in the ICU were more likely to develop persistent symptoms of posttraumatic stress disorder years later.32 On the other hand, no one knows the quantity of sedative medication in each class that is required to reliably ensure complete amnesia. In a study of 149 patients, there was no relationship between aggregate sedative dose during mechanical ventilation and patients’ recall of the ICU experience 2 months later.33 In general, intensivists must balance the proven benefits of administering fewer sedative medications (by daily stopping of sedative infusions or use of sedation protocols) against the uncertain adverse effects of unpleasant symptom recall. Indeed, the data suggest that recall of delusional memories (often exacerbated by sedatives) is associated with greater post-ICU psychopathology than is patient recall of unpleasant but real memories.34
 Pharmacology and Clinical Use of Sedatives Commonly Administered in the Intensive Care Unit
Pharmacology and Clinical Use of Sedatives Commonly Administered in the Intensive Care Unit
The intensity of sedation required for patients can vary markedly throughout their ICU stay, depending on the course of their disease, the external environment, and the time of day. The ideal sedative possesses a rapid onset of action, is convenient to administer and titrate, produces effective and reproducible sedation to the desired clinical goal, and is free of hemodynamic, cardiac, or respiratory side effects. To simplify extended infusion in the critically ill patient, the ideal sedative also should exhibit linear pharmacokinetics with no clinically significant protein binding or drug interactions. Drug clearance in renal and hepatic impairment should be clearly characterized, and the ideal sedative would not be cleared by dialysis. Finally, the ideal sedative would permit rapid and predictable recovery after discontinuation, with no long-term adverse effects. Although new sedative agents have been added to the armamentarium in recent years, this optimal group of characteristics has yet to be formulated in a single agent. Therapy with more than one drug is often used to optimize sedation in critically ill patients, and some combination of a BZD or propofol with an opioid analgesic is the most commonly employed regimen.5,35–37
Opioid Analgesics
Although opioid analgesics are recognized as the drug class most frequently prescribed for pain management, opioids also have a role in management of anxiety. Unrecognized or inadequately treated pain from pathology or ICU procedures can create anxiety in 20% to 60% of patients.13–15 Patients who are unable to communicate the source of their distress may suffer from persistent pain. For this reason, early and systematic scrutiny for the presence of pain is crucial to effective management in the visibly anxious ICU patient.
Analgesic agents recommended for use in critically ill patients by the 2002 American College of Chest Physicians/Society of Critical Care Medicine/American Society of Health System Pharmacists Clinical Practice Guidelines38 (hereafter referred to as the Practice Guidelines) are described in Table 186-2. Differences in analgesic potency, response, and recovery time are associated with the pharmacokinetic properties of each drug as well as their mu and kappa receptor-binding affinity in the CNS. In addition to sedation and analgesia, opioids can produce respiratory depression, constipation, urinary retention, nausea, and confusion. Combined use of opioids and BZDs results in synergistic effects that permit dosage reduction, which may reduce adverse effects and drug accumulation. For patients with chronic pain or previous use of opioids, increased dose requirements due to tolerance should be considered. Use of the opioid antagonist, naloxone, as a reversal agent is not recommended routinely after prolonged opioid analgesia because of the risk of withdrawal symptoms and the potential to induce cardiac arrhythmias.38
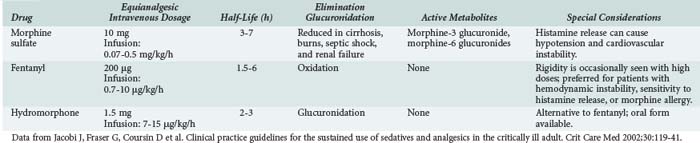
Several analgesics are not recommended for critically ill patients. Meperidine has an active metabolite, normeperidine, which causes CNS excitation associated with delirium and seizures. Because the active metabolite is excreted by the kidneys, patients with renal insufficiency are at high risk for adverse effects. Opioid antagonist-agonists (e.g., nalbuphine, butorphanol, buprenorphine) can reverse the desirable effects of other opiate agents and are not recommended for routine use in the ICU. Nonsteroidal antiinflammatory analgesics offer few advantages for the critically ill and can cause gastrointestinal bleeding, bleeding due to platelet inhibition, and renal insufficiency.38 Alfentanil, sufentanil, and remifentanil are fentanyl derivatives with higher potency and/or shorter half-lives than fentanyl, but comparative data evaluating these agents for sedation in the ICU are scarce, and the drugs are more expensive than fentanyl.37,39
Benzodiazepines
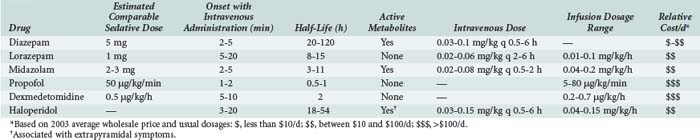
The anxiolytic, amnestic, anticonvulsant, and muscle-relaxing effects of BZDs are mediated through GABAA binding sites on neuronal γ-aminobutyric acid (GABA) receptors. After binding to the receptor site, BZDs facilitate the GABA-mediated increase in chloride conductance with subsequent membrane hyperpolarization and inhibition of neuronal impulses. The amnestic properties of these drugs correlate with their GABA agonist activity in the limbic system.40 BZD binding is stereospecific and saturable, and the potency of an individual BZD agent correlates with its receptor affinity. Other ligands act as antagonists (e.g., flumazenil) or inverse agonists. Inverse agonists reduce the efficiency of GABA interaction with the receptor, causing CNS stimulation; drugs with these properties are in development.41 Table 186-3 describes the comparative pharmacology of selected BZDs and other ICU sedatives.
Both acute and chronic tolerance to BZDs (associated with decreased receptor activity) has been described. In ICU patients, acute tolerance can occur after just 24 hours.41 Paradoxical reactions have also been associated with BZDs, most commonly in the elderly and in patients with a history of preexisting CNS disease, substance abuse, or psychiatric disease. Patients who develop a paradoxical reaction to a BZD should be switched to a medication in another drug class, such as propofol, dexmedetomidine, or haloperidol.
A key protein in the primary metabolic pathway for diazepam, the CYP subfamily enzyme, CYP2C19, is genetically polymorphic. Isoenzymes of CYP2C19 that are present in 3% to 5% of Caucasians and African Americans and 12% to 100% of Asian ethnic groups are associated with a significant decrease in diazepam metabolism. Therefore on occasion, a patient treated with diazepam may experience unexpectedly prolonged sedation.42 Some drugs commonly used in critically ill patients, such as amiodarone, fluconazole, omeprazole, and valproic acid, also inhibit CYP2C19 activity. In contrast, cigarette smoking induces hepatic microsomal enzymes. This effect increases the clearance of diazepam and other BZDs.43 For these reasons, the clinical response to diazepam is often unpredictable in critically ill patients.
Lorazepam has been a preferred agent for ICU sedation in many critical care units since its approval in 1977; lorazepam is recommeded for long-term (>48 hours) ICU sedation in the 2002 Practice Guidelines. Because lorazepam undergoes hepatic glucuronidation to inactive metabolites, its pharmacokinetic parameters are not altered significantly in elderly or critically ill patients, except in those with severe renal or hepatic failure. Lorazepam is the least lipophilic of the injectable BZDs; therefore it crosses the blood-brain barrier slowly, resulting in a delayed onset of action (5-20 minutes) and a longer duration of action, with an elimination half-life of 10 to 20 hours.44 After chronic dosing, accumulation of lorazepam and prolonged sedation are less likely than with diazepam. Lorazepam is also 5 to 6 times more potent than diazepam, and the amnestic effect of lorazepam has a longer duration than an equivalent diazepam dose. Lorazepam can be given by intramuscular injection.41
Lorazepam is formulated in 18% polyethylene glycol (PEG) and 2% benzyl alcohol in propylene glycol (PG) for injection. Although usual lorazepam doses deliver only minute amounts of PEG and PG, long-term sedation with high doses can lead to patients receiving substantial doses of PEG and PG. Both the PEG45 and the PG46,47 components of the vehicle have been associated with development of lactic acidosis, hyperosmolar coma, and reversible nephrotoxicity with high doses or lengthy infusions. Although the dosages implicated have not been prospectively defined, lorazepam doses exceeding 18 mg/h for longer than 4 weeks, or 25 mg/h for hours to days, should be avoided.38 Because of its poor solubility, precipitation can occur when lorazepam is administered by continuous infusion. On the basis of manufacturer information and clinical recommendations, the manufacturer’s vial concentration (either 2 or 4 mg/mL) should be diluted 1 : 1 with 5% dextrose injection in a glass container, not in polyvinyl chloride bags.48
Midazolam, a short-acting, water-soluble BZD prodrug, is approximately 3 times more potent than diazepam. After self-converting to a lipid-soluble form by closure of the diazepine ring at physiologic pH values in the bloodstream, midazolam rapidly enters the CNS to produce sedation within 2 to 5 minutes. This property makes midazolam ideal for patients who require immediate control of anxiety or agitation.38 Initial dosages recommended are 2 to 5 mg IV every 5 to 15 minutes. The drug quickly redistributes to peripheral tissues, and effects dissipate if a continuous infusion is not initiated. When infused over days for chronic sedation, the mean elimination half-life of 10 hours may increase to 30 hours as peripheral tissue stores release accumulated midazolam. The pharmacodynamic effects of BZDs often do not correspond well with reported elimination half-lives.49 In comparing the clinical sedation recovery rate (time to wakefulness) for midazolam versus diazepam, 8 trials reported a faster recovery rate from diazepam, 19 trials reported no difference in sedative recovery time, and only 1 trial demonstrated a faster recovery with midazolam.38
Midazolam is metabolized by the CYP3A4 isoenzyme to an active metabolite, α-hydroxymidazolam, which has 60% of the potency of the parent drug. α-Hydroxymidazolam is quickly biotransformed to its conjugated salt, α-hydroxymidazolam glucuronide (10% potency), which does not significantly contribute to the sedative properties of midazolam except when it accumulates in renal failure. Inhibitors of CYP3A4, such as macrolide antibiotics, diltiazem, propofol, and fluconazole, reduce the metabolism of midazolam and prolong its sedative actions.41 The combined effects of drug interactions, altered protein binding, fluid shifts, altered hepatic metabolism, and renal failure can result in prolonged elimination and an unpredictable time to awakening after discontinuation of midazolam when the drug is used for longer than 48 to 72 hours. For these reasons, the 2002 Practice Guidelines recommend midazolam for short-term use only.38
Several randomized controlled studies have compared BZD sedatives in critically ill patients. Two unmasked studies in mixed populations of ICU patients reported no difference between midazolam and lorazepam in time until sedation or in time until return to baseline mental status.49,50 In contrast, a double-masked randomized comparison of lorazepam versus midazolam, using a target-controlled IV infusion titrated to maintain a moderate level of sedation for 12 to 72 hours, reported a delayed emergence from sedation with lorazepam.44 Other longer-term studies suggest that lorazepam is easier to titrate to the desired sedation level than midazolam.51
Because lorazepam is equally effective and produces less hypotension, it is the BZD recommended in the 2002 Practice Guidelines for most ICU patients; it is administered either by continuous infusion or by intermittent IV dosing (1-4 mg every 2-6 hours).38
BZDs, particularly midazolam and diazepam, can cause respiratory depression and hypotension due to vasodilation when administered in large doses. If these effects require rapid reversal, flumazenil may be used to antagonize BZD agonists at the GABA receptor binding site. Flumazenil administered IV in doses of 0.2 to 1 mg reverses the sedative and amnestic effects of BZDs immediately. Flumazenil is metabolized rapidly, with a half-life of 1 hour but a clinical duration of effect often less than 30 minutes; therefore, situations requiring prolonged antagonism may necessitate a continuous flumazenil infusion. Diagnostically, flumazenil has been used to differentiate between BZD-induced unresponsiveness and other forms of CNS pathology. Flumazenil is relatively contraindicated in patients with known BZD dependence and chronic use, because acute withdrawal symptoms and seizures have been reported in these patients.41



Full access? Get Clinical Tree


