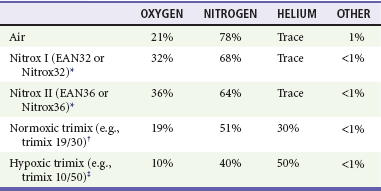
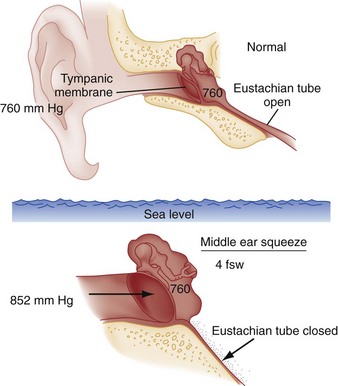
Chapter 143 Underwater free diving to salvage wrecks and to harvest seafood, sponges, coral, and mother-of-pearl has been practiced for more than 5000 years.1 Historically, divers also used breathing tubes, such as hollow reeds; however, it is nearly impossible to use these at depths of more than 3 feet because of the restriction of inspiration by underwater pressure. Subsequent inventions from the 16th to the 19th centuries, including diving dresses, allowed divers to remain underwater for prolonged periods at depths of up to 12 fathoms (72 feet).2 The first diving dress (1715) was a reinforced, leather-covered barrel with watertight armholes and a viewing porthole.2 With the advent of these technologies, the symptoms of diving-related illness began to be recognized. Colonel William Pasley, the officer in charge of a unit of the British Royal Engineers that salvaged the sunken warship HMS Royal George in 1840, observed symptoms in his divers.3 At approximately the same time, similar symptoms and even fatalities were observed among caisson workers.* The ailment became known as caisson disease, but the construction workers on the Brooklyn Bridge (built from 1870 to 1883) attached the name “the bends,” characterizing the symptoms that often caused the victim to bend forward in pain.3 The first clinical description of caisson disease was by Paul Bert in 1878.3 He correctly attributed the disease to nitrogen gas coming out of solution in the tissues during decompression. This led to the recommendation of slow ascents for pressurized workers and the development of the first recompression chambers. The significant breakthrough allowing diving at depth was the invention of the aqua-lung by Jacques-Yves Cousteau and Emile Gagnan in 1943.2 The lighter and less expensive equipment, widely known by its acronym SCUBA (self-contained underwater breathing apparatus), does not require a surface supply of air or the support personnel that are necessary for helmet diving. This innovation allowed widespread deep-sea diving, and millions of divers have become certified to date. Most amateur divers use compressed air, open-circuit scuba equipment at depths of less than 130 feet of seawater (fsw). Systems with artificial mixtures of various gases, however, are used to extend the depths to which divers can descend. Some of these are used in sport diving, but their use is uncommon and is primarily limited to commercial applications (Table 143-1). Table 143-1 *Enhanced air nitrox, oxygen enriched air, nitrox, EANx, SafeAir, “devil gas,” “voodoo gas.” †A normoxic mix, such as 19/30, is used in the depth range of 30 m (100 feet) to 60 m (200 feet). ‡A hypoxic mix, such as 10/50, is used for deeper diving, as a “bottom” gas only; it cannot safely be breathed at shallow depths where the oxygen partial pressure is less than 0.18. The total number of diving-related injuries is unknown, but the absolute numbers of patients with decompression-related illnesses, one of the most serious dive-related injuries, continue to climb as the number of divers has increased despite the rate per 10,000 dives remaining relatively constant since 2001.4 This rate varies somewhat on the basis of the type of diver: 0.015% for scientific divers, 0.01 to 0.019% for recreational divers, 0.030% for U.S. Navy divers, and 0.095% for commercial divers.5 The rate of mortality in diving varies between 1.5 and 9 per 100,000 dives. With the popularity of diving and the relative ease of rapid travel from distant destinations, it behooves even the land-locked emergency physician to be aware of diving-related illnesses. To understand the pathophysiologic processes of dysbarisms and barotrauma, one should be familiar with several of the laws of physics that define the behavior of liquids and gases (Table 143-2; Figs. 143-1 to 143-5). The human body is composed mostly of water and behaves like a liquid subject to Pascal’s law, which states that a pressure applied to any part of a liquid is transmitted equally throughout. Pressure changes, however, do alter the volume within the air-filled spaces of the body, including the lungs, bowel, sinuses, and middle ear, according to Boyle’s law. This law states that at constant temperature, the absolute pressure and the volume of gas are inversely proportional (PV = k). In other words, as pressure increases (with descent), the gas volume is reduced; as the pressure is reduced (with ascent), the gas volume increases. Table 143-2 Figure 143-1 Pascal’s law. A pressure applied to any part of a liquid is transmitted equally throughout. Middle ear barotrauma (MEBT), also known as barotitis or “ear squeeze,” is the most common complaint of scuba divers. It is experienced by 30% of novice scuba divers and 10% of experienced divers.6,7 The middle ear is an air-filled space with solid bone walls except for the tympanic membrane (Fig. 143-6). The eustachian tube is the only anatomic passage to the external environment. External ear barotrauma is less common than MEBT and results from the outward bulging of the tympanic membrane during descent. Normally, the external auditory canal is filled with water during descent. Obstruction of the external auditory canal because of cerumen, stenosis, earplugs, or a tight-fitting wet suit hood can trap air, causing a relative negative pressure. This may lead to localized pain. Patients may have hemorrhages in the wall of the external auditory canal on examination, but the symptoms are typically self-limited.8 Inner ear barotrauma (IEBT) results in damage to the cochleovestibular apparatus. It is much less common than MEBT but is associated with greater morbidity. A large negative pressure gradient develops in the middle ear if the diver is unable to equalize pressure during descent, similar to MEBT. Inward deflection of the tympanic membrane is transmitted to the oval window of the cochlea through the ossicles. Movement of the oval window creates a pressure wave within the perilymph of the cochlea, which causes an outward distention of the round window into the middle ear. Sudden equilibration of pressure in the middle ear or a vigorous Valsalva maneuver may rupture the round window, lead to hemorrhage into the inner ear, or tear the labyrinthine (Reissner’s) membrane.9–11 Obstruction of the sinus ostia by mucosal thickening, polyps, pus, or deviated septum predisposes to sinus barotrauma, the second most common complaint among divers.8,9 The air-filled maxillary, frontal, and ethmoidal sinuses are susceptible to volume-pressure changes on ascent or descent; the most commonly affected is the maxillary sinus, followed by the frontal.11 The most common symptom is facial pain; epistaxis is common. As water pressure increases during descent, a negative pressure develops within the dive mask over the eyes and nose, which must be equalized by forced exhalation through the nose. When this is not adequately performed, the large negative pressure gradient may lead to facial and conjunctival edema, diffuse petechial hemorrhages on the face, and subconjunctival hemorrhages.8 Very rarely, optic nerve damage can result from severe facial barotrauma. Nitrogen narcosis, known as rapture of the deep, results from the intoxicating effects of increased tissue nitrogen concentration at depth. Symptoms include euphoria, false feeling of well-being, confusion, loss of judgment or skill, disorientation, inappropriate laughter, diminished motor control, and tingling and vague numbness of the lips, gums, and legs.3 With breathing of compressed air, symptoms typically begin to occur at approximately 100 feet and often become profound at depths of more than 150 feet.3 Because of these dangers, the use of compressed air is not recommended for sport diving to depths of more than 120 feet. Although the effects of nitrogen narcosis resolve with ascent to shallower depths and are variable between individuals, the diver may drown because of poor judgment or seriously impaired motor skills in the presence of a dive emergency. Rarely, other gases, such as carbon monoxide and carbon dioxide, can contaminate the air that is compressed into a tank. This can happen, for example, if the compressor intake is placed too close to the compressor’s engine exhaust. As in the case of oxygen and nitrogen, the partial pressure of these contaminants in the tissues increases dramatically with depth, potentiating their clinical effects. The symptoms of hypercarbia or carbon monoxide poisoning are more severe at elevated partial pressures. Hypercarbia increases a diver’s susceptibility to CNS oxygen toxicity.3 Rebreathers release microscopic calcium hydroxide or “soda lime” dust particles into the apparatus.12 These particles are small enough and have geometric characteristics that allow them to be deposited in the alveoli. When soda lime comes into contact with water, it forms a caustic liquid. In the event of a hose rupture allowing seawater contamination of the circuit, caustic burns to the mouth, throat, and airways may result. Chronic exposure to soda lime dust may contribute to long-term effects on respiratory function. Serious gastrointestinal barotrauma is a rare condition in scuba divers. It results from the expansion of bowel gas in the small intestine and colon on ascent after diving. Predisposing factors include consumption of carbonated beverages, large meals, or gas-producing foods before diving as well as performance of the Valsalva maneuver in the head-down position. Symptoms include eructation, flatulence, bloating, and crampy abdominal pain. In divers with inguinal or other hernias, the potential for expansion of trapped gas within the hernia exists, and expansion may result in incarceration or strangulation.13,14 Gastric rupture is a rare complication.14 Although gastrointestinal barotrauma is a rare entity, it should be suspected in the diver-patient with a provocative history and abdominal pain. Asthmatics have a twofold increased risk for pulmonary barotrauma compared with the general diver population.15 There are six mechanisms that contribute to the increased risk in asthmatics: 1. Bronchospasm and mucus plugging predispose local regions of lung to injury. 2. When air is compressed, it becomes denser. This may contribute to greater turbulent flow through narrow airways. 3. During scuba diving, there is a reduction in breathing capacity related to the effects of immersion. At 33 feet underwater, the maximum breathing capacity of a normal scuba diver is only 70% of the surface value. At 100 feet underwater, the reduction is approximately 50%. 4. When compressed air (from the scuba tank) expands in the regulator before delivery to the lungs, it cools (Charles’ law). Breathing of chilled air may trigger bronchospasm in asthmatics who have a cold-induced component of their disease. 5. Scuba diving takes some effort; asthmatics who have an exercise-induced component of their disease may experience bronchospasm. 6. Compressed air may be contaminated by pollen and other allergens. Traditionally, asthmatics were advised not to dive. Several experts, however, propose more liberal guidelines.16–18 The risk of diving is probably acceptable if the diving candidate with asthma demonstrates normal pulmonary function at rest (forced vital capacity [FVC], midexpiratory flow, forced expiratory volume in 1 second, and forced expiratory flow between 25 and 75% of FVC) and after strenuous exercise. Asthma severity can wax and wane. Because symptoms may worsen for 4 to 6 weeks after an upper respiratory infection or during certain seasons, asthmatics should refrain from diving until they are completely free of symptoms despite the pulmonary function criteria. Pulmonary barotrauma can also cause alveolar hemorrhage.19,20 Patients may present with hemoptysis coincident with chest pain and dyspnea. Chest radiography may reveal an interstitial infiltrate.
Scuba Diving and Dysbarism
Perspective
Principles of Disease
GAS LAW
FORMULA
SIGNIFICANCE
Pascal’s law: A pressure applied to any part of a liquid is transmitted equally throughout.
ΔP = ρg (Δh)
ΔP is the hydrostatic pressure.
ρ is the fluid density.
g is acceleration due to gravity.
Δh is the height of fluid.
Pressure increases in a contained space are transmitted throughout; significant for inner ear barotrauma and middle ear barotrauma (see Fig. 143-1)
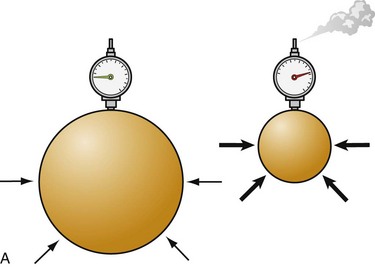
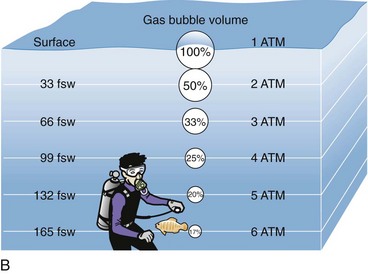
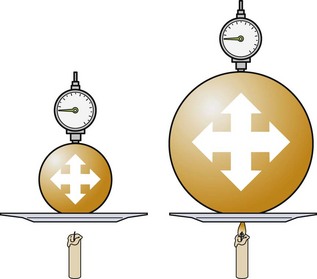
Boyle’s law: At a constant temperature, the absolute pressure and the volume of gas are inversely proportional. As pressure increases, the gas volume is reduced; as the pressure is reduced, the gas volume increases.
P1 • V1 = P2 • V2
Relates to change in the volume of a gas caused by the change in pressure due to depth, which defines the relationship of pressure and volume in breathing gas supplies (see Fig. 143-2)
Charles’ law: At a constant pressure, the volume of a gas is directly proportional to the change in the absolute temperature.
V1/T1 = V2/T2
Increasing pressure (filling a scuba tank) causes heat; cooling a tank decreases the pressure (see Fig. 143-3)
The general gas law combines these concepts to predict the behavior of a gas when the factors change.
P1 • V1/T1 = P2 • V2/T2
P1 is the initial pressure.
V1 is the initial volume.
T1 is the initial temperature.
P2 is the final pressure.
V2 is the final volume.
T2 is the final temperature.
A means of relating pressure, volume, and temperature together in one equation when variables are not constant
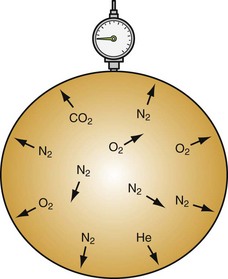
Dalton’s law: The total pressure exerted by a mixture of gases is equal to the sum of the pressures (partial pressures) of each of the different gases making up the mixture, with each gas acting as if it alone is present and occupies the total volume.
PTotal 3 P1 + P2 + P3 + … + Pn
Nitrogen under pressure acts as if other gases are not present (see Fig. 143-4)
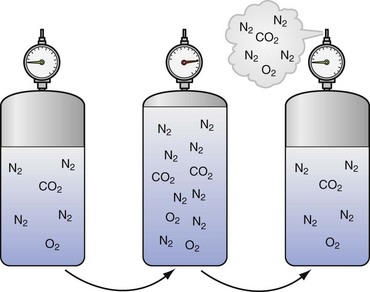
Henry’s law: The amount of a gas that will dissolve in a liquid at a given temperature is directly proportional to the partial pressure of that gas.
ep = ekc
e is approximately 2.7182818 (the base of the natural logarithm).
p is the partial pressure of the solute above the solution.
c is the concentration of the solute in the solution.
k is the Henry’s law constant.
More nitrogen is taken into solution (e.g., serum) at high pressures than comes out of solution at lower pressures (see Fig. 143-5)
Clinical Features
Middle Ear Barotrauma
External Ear Barotrauma
Inner Ear Barotrauma
Barosinusitis
Facial Barotrauma
Disorders Arising at Depth
Contaminated Air
Disorders Arising on Ascent
Gastrointestinal Barotrauma
Pulmonary Barotrauma

Full access? Get Clinical Tree


Scuba Diving and Dysbarism
Only gold members can continue reading. Log In or Register to continue




