CHAPTER 40 Safety and Outcome in Pediatric Anesthesia
Anesthesiology has served as a model for patient safety and was the first medical specialty to recognize patient safety as an independent problem (Gaba, 2000). The safety of infants and children undergoing general anesthesia has improved considerably since the 1970s, as evidenced by significant decreases in anesthesia mortality despite the fact that more complicated surgical procedures have been performed on sicker children and more premature infants.
Since the 1980s, anesthesiologists’ awareness of and interest in the subject of patient safety has reached a new peak, and a number of new steps have been taken to ensure perioperative patient safety (Keats and Siker, 1985; Smith and Norman, 1987; Runciman, 1988a; Runciman, 1988b). In addition to advanced technology for patient monitoring, standards for basic patient monitoring have been implemented (American Society of Anesthesiologists [ASA], 1986; Eichhorn et al., 1986). Documentation of the quality assurance (QA) process has been emphasized as an integral and essential component for hospital accreditation by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) in the United States. To further improve the quality of patient care, a number of national and international organizations have been created, including the International Committee on Prevention of Anesthesia Mortality and Morbidity, the Anesthesia Patient Safety Foundation, the Australian Patient Safety Foundation, and the ASA Committee on Patient Safety and Risk Management (Cooper and Pierce, 1986; Cooper, 1988; Pierce, 1984, 1988; Runciman, 1988b). The Institute of Medicine of the National Academies is an independent, nonprofit organization that seeks to ask and answer the nation’s questions about health and health care. Their reports, such as the Preventing Medication Errors series, have analyzed complex problems in the modern health care industry and provided solutions that have been widely adopted. Sessions on patient safety topics have also been incorporated into the programs of the American Society of Anesthesiologists and Society for Pediatric Anesthesia annual meetings.
Nevertheless, anesthesia-related morbidity and mortality still do occur during the administration of anesthesia and can happen with any anesthesiologist under various situations. An analysis of anesthesia mishaps from closed anesthesia malpractice claims in the United States, before the new patient monitoring standards with pulse oximetry and capnography were instituted, indicated that at least 80% of the claims consisted of preventable hypoxic damage caused by human errors rather than mechanical failures (Davis, 1984).
Allnutt (1987), a member of the British Army Personnel Research Establishment, examined human factors in anesthesia- related mishaps in comparison with those in military aviation accidents. He stresses that “both pilots and doctors make many errors” (i.e., performance that deviates from the ideal). “Usually there is sufficient slack in the system for the error to be … noticed and corrected, but some apparently innocuous errors are not noticed and some systems are not so forgiving as others” (such as a high performance aircraft in flight). “Thus recovery from a control error when flying at high speed, low level may not be possible, whereas the same error in the cruise [at high altitude] might barely occasion comment.” A basic tenet of Allnutt’s theory is that “all human beings, without any exception whatsoever, make errors and that such errors are a completely normal and necessary part of human cognitive function.” He goes on to state that “to claim exemption on the grounds of being a senior professor [or a] test pilot … or of having 30 years’ experience or 3000 accident-free hours, is the first step on the road to disaster.” The first step toward the prevention of catastrophe is for the pilot or the anesthetist to accept that he or she is as likely as anyone else to make an error (Pierce, 1988).
Anesthesia-related mortality
Overall Anesthesia-Related Mortality
The number of deaths associated with general anesthesia has declined steadily over the past several decades as the standard of anesthesia practice has improved and as advances have been made in instrumentation, anesthetic and adjuvant drugs, and safety monitors and standards. An extensive survey of 10 university hospitals by Beecher and Todd (1954) involving nearly 600,000 anesthetic cases between 1948 and 1952 suggested that mortality primarily attributable to anesthesia occurred in 1:2680 anesthesia cases (3.7:10,000), whereas the overall anesthesia-associated mortality was 1:1580 (6.3:10,000) anesthesia procedures (Graff et al., 1964). A survey by Dornette and Orth (1956) showed similar mortality rates. Data from the Baltimore Anesthesia Study Committee (1953 to 1963) showed an anesthesia-related death rate of 2.7:10,000 cases. During the 1970s and 1980s, statistics on anesthesia-related mortality in the United States were scarce, apparently because of medicolegal concerns. Anesthesia-related mortality from Canadian, British, and European sources during this time ranged from 0.7 to 2.2:10,000 anesthetic procedures (Bodlander, 1975; Harrison, 1978; Hovi-Viander, 1980; Turnbull et al., 1980; Lunn and Mushin, 1982; Hatton et al., 1983; Vickers and Lunn, 1983).
In the 1980s, European and Australian studies showed much lower rates of operative mortality directly attributed to anesthesia. A report from the British Confidential Enquiry into Perioperative Deaths (CEPOD), a survey that was jointly organized by the Associations of Anaesthetists and Surgeons of Great Britain and Ireland during 1985 and 1986 and included more than 480,000 general anesthetic procedures, indicated that mortality attributable to anesthesia alone was 1:185,000 (0.054:10,000) procedures (Buck et al., 1987). However, anesthesia, along with other causes, was thought to be a contributory factor in the death of between 1.4 (surgeons’ estimate) and 9.8 (anesthetists’ estimate) per 10,000 cases. A prospective survey of anesthesia outcome by the French Health Ministry during the time from 1978 to 1982, in which nearly 200,000 general anesthetic cases were documented, revealed an intraoperative and early postoperative death rate solely attributable to anesthesia to be 0.76:10,000 procedures, and an intraoperative death rate of 0.44:10,000 cases (Table 40-1) (Tiret et al., 1986, 1988).
TABLE 40-1 Historical Changes in Anesthesia-Related Mortality (All Ages)*
| Authors (Country) | Years Includedin Study | Incidence per 10,000 |
| Beecher and Todd (United States) | 1948 to 1952 | 3.7 |
| Graff et al. (United States) | 1953 to 1963 | 2.7 |
| Hovi-Viander (Finland) | 1975 | 2 |
| Lunn and Mushin (United Kingdom) | 1978 to 1979 | 1 |
| Tikkanen (Finland) | 1986 | 0.6 |
| Tiret et al. (France) | 1978 to 1982 | 0.76† |
| Buck et al., CEPOD (United Kingdom) | 1985 to 1986 | 0.05† |
| Eichhorn (United States) | 1976 to 1988 (ASA PS 1 or 2) | 0.05† |
| Kawashima (Japan) | 1994 to 1998 | 0.13† |
| Lagasse (United States) | 1995 to 1999 | 0.75 |
| Fasting and Gisvold (Canada) | 1996 to 2000 | 0.12 |
| Irita (Japan) | 1999 to 2002 | 0.1† |
| Lienhart (France) | 2006 | 0.12† |
ASA PS, American Society of Anesthesiologists physical status; CEPOD, Confidential Enquiry into Perioperative Death.
* For complete citations of studies, consult chapter reference list online at www.expertconsult.com.
† Anesthesia primarily responsible only; other factors may be involved.
A longitudinal comprehensive anesthesia-related mortality study from New South Wales, Australia, which was continued by the same author using the same criteria since 1960 (interrupted between 1980 and 1983 because of the temporary loss of legal confidentiality), has indeed shown a steady decline in anesthetic mortality from 1.8:10,000 cases in 1960 to 0.38:10,000 cases by 1984 (Holland, 1984, 1987). Similarly, a longitudinal study from South Africa has also shown a decreasing trend in anesthesia-related mortality from 3.3:10,000 between 1956 and 1965 to 0.7:10,000 between 1983 and 1987 (Table 40-2) (Harrison, 1978, 1990).
TABLE 40-2 Anesthesia-Related Mortality: Longitudinal Studies at the Same Institution
| Authors (Country) | Years Included in Study | Incidence per 10,000 |
| Holland (Australia) | 1960 to 1969 1970 to 1980 1983 to 1985 | 1.8 0.97 0.38 |
| Harrison (South Africa) | 1956 to 1965 1967 to 1976 1983 to 1985 | 3.3 2.2 0.7 |
From Holland R: Anaesthetic mortality in New South Wales, Br J Anaesth 59:834, 1987; Harrison GG: Death due to anesthesia at Groote Schuur Hospital, Cape Town: 1956-1987. Part II. Causes and changes in aetiological pattern of anesthetic-contributory death, S Afr Med J 77:416, 1990.
In the United States, Eichhorn (1989) analyzed data from nine Harvard University–affiliated hospitals between 1976 and 1988. He reported 11 major anesthesia-related intraoperative accidents, including five deaths based on more than 1 million anesthetic procedures in relatively healthy patients (ASA PS 1 and 2); the anesthetic mortality was 0.05:10,000 cases; postoperative mortality, including two deaths from halothane hepatitis, was excluded from these statistics. After implementation of patient monitoring standards in 1985, there was only one serious accident (no mortality) in 319,000 general anesthesia procedures (Eichhorn et al., 1986). Of the 11 major accidents, eight cases were considered preventable with proper monitoring, especially with capnography. Unrecognized hypoventilation (seven cases) was the most common cause of major mishaps. Inadequate supervision of residents and nurse anesthetists was also contributory. Although Eichhorn’s statistics were based on a malpractice insurance database and are likely different and considerably lower than the data based on a peer-review process, anesthesia-related safety appears to have improved significantly.
Irita and others (2004) analyzed morbidity and mortality statistics in Japan from 1999 to 2002 from the Japanese Society of Anesthesiologists annual survey. They reviewed 3,855,384 cases completed during that time. The incidence of cardiac arrest and mortality totally attributable to anesthesia management was 0.47 and 0.1 per 10,000 anesthesia procedures. Half of the anesthesia-related deaths were caused by airway or ventilatory problems; the other causes were medication-related and infusion/transfusion accidents.
Practitioners of anesthesiology have institutionalized patient safety in their scientific and governing bodies (such as the ASA Anesthesia Patient Safety Foundation and similar organizations in other countries) (Cooper and Gaba, 2002). In 1999, the Committee on Quality of Health Care in America for the Institute of Medicine published a report entitled To Err Is Human: Building a Safer Health Care System (Kohn et al., 1999). The report stated, “Anesthesia is an area in which very impressive improvements in safety have been made.” This statement was based on the statistics that anesthesia-related mortality rates had decreased from two deaths per 10,000 anesthetic procedures in the 1980s to about 1 death per 200,000 to 300,000 anesthetic procedures administered at the time the report was published (probably quoting the report by Eichhorn [1989]). Such dramatic decreases in anesthetic mortality can be attributed to a variety of mechanisms, including wide acceptance of new monitoring guidelines, improvement in monitoring techniques, safer anesthetic drugs, and adoption of QA mechanisms and other systematic approaches for reducing human and systemic errors (Gaba, 2000; Stoelting, 2000; Lagasse, 2002).
Mortality in Infants and Children
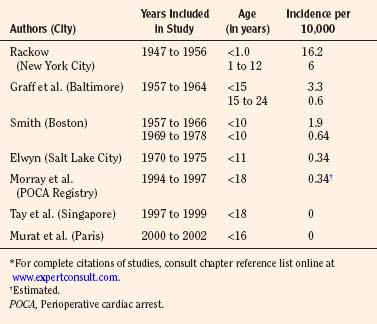
Among the pediatric age group, the anesthesia-related mortality has been reported to be disproportionately high in the literature. In the 1950s, Beecher and Todd (1954) and Stevenson and others (1953) found that accidental deaths resulting from anesthesia were disproportionately high during the first decade of life. Between 1947 and 1956 at the Babies Hospital/Columbia-Presbyterian Medical Center, Rackow et al. (1961) found that the rate of cardiac arrest associated with anesthesia in infants younger than 1 year of age (1 in 617 cases, or 16.2:10,000) was higher than in children aged 1 to 12 years (1 in 1678, or 6.0:10,000) and in adults (1 in 2580, or 3.9:10,000) (Beecher and Todd, 1954). Hypoventilation and hypoxia from ether overdose were among the common causes of death. Smith (1956) emphasized the importance of certain factors contributing to the high anesthetic mortality in pediatric anesthesia. These factors included: lack of proper equipment, improper preoperative rehydration and stabilization, inadequate intraoperative monitoring, error in fluid replacement, and aspiration of vomitus. Today, half a century later, some of these factors are still applicable.
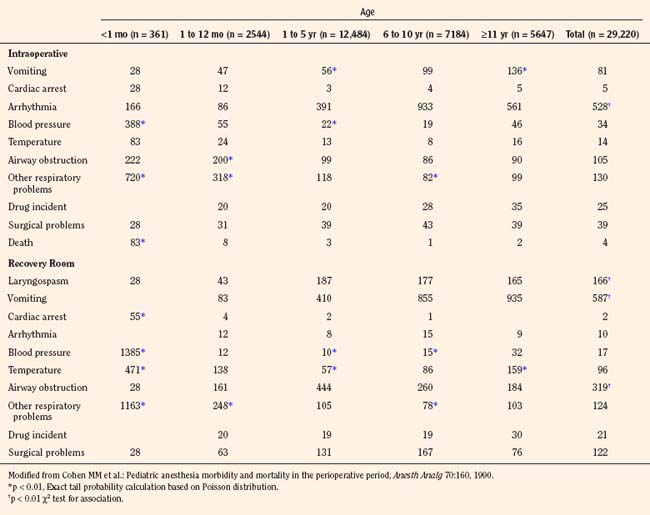
In a report by the Baltimore Anesthesia Study Committee, anesthesia-related mortality for children younger than 15 years of age was found to be 3.3:10,000 cases (vs. 0.6:10,000 for those aged 15 to 24 years) (Phillips and Frazier, 1957; Graff et al., 1964). These authors also found that the ratio of anesthesia deaths to total surgical deaths was higher in the neonatal period than in any other age group. Furthermore, 57% of the deaths related to anesthesia occurred in healthy children (ASA PS 1 and 2). Respiratory problems were implicated in 83% of the anesthesia-related deaths (Graff et al., 1964) (Table 40-3).
In contrast, in a review of 73 anesthesia-related cardiac arrests in children between 1960 and 1972 (33% resulted in death), Salem and others (1975) found that both respiratory (airway obstruction) and cardiovascular causes (blood loss, preoperative anemia, inappropriate injection of succinylcholine and potassium) were equally responsible. In retrospect, most of these accidents were preventable.
In an attempt to improve patient safety during anesthesia in infants and children, a number of important innovations and improvements in perioperative management and monitoring were made by the pioneering pediatric anesthesiologists in the 1950s and 1960s. These innovations include homemade pediatric blood pressure cuffs and precordial stethoscopes (by Robert Smith in Boston) and endotracheal intubation (by Margo Demming in Philadelphia). Fellowship training in pediatric anesthesia also began in several cities in North America and in the United Kingdom in the 1950s and spread across the continent by the early 1970s (see Chapter 41, History of Pediatric Anesthesia).
By the mid-1970s, anesthesia-related morbidity and mortality decreased considerably. Management of known hazards, such as the full stomach, preoperative fever, and hypovolemia, was greatly improved by increased experience and knowledge (Smith, 1975). Smith (1980) reported the anesthesia-related mortality rate of 2:10,000 general anesthesia cases in children (0 to 10 years old) during the decade ending in 1966 at the Children’s Hospital in Boston; the mortality rate decreased to 0.6:10,000 anesthesia cases in the decade ending in 1978. Furthermore, there was a series of 35,710 consecutive tonsillectomies and adenoidectomies, mostly in children, without a single death at the Eye and Ear Hospital of Pittsburgh (Petruscak et al., 1974). There were 7500 consecutive anesthesia procedures for cleft lip and cleft palate repairs without a death at the Children’s Hospital in Boston (Smith, 1975). Elwyn, in his 5-year study between 1970 and 1975 at the Primary Children’s Hospital in Salt Lake City, reported one anesthetic death in 29,101 anesthetic procedures (0.34:10,000) in children under 11 years of age (Smith, 1980). Downes and Raphaely (1979) reported an anesthetic mortality of 0.2:10,000 cases (from a total of 50,000 patients) at Children’s Hospital of Philadelphia. Most fatalities occur during the first year of life, beyond which the risk of mortality is no higher than that in teenagers and young adults (Table 40-3) (Smith, 1975).
Despite advances in pediatric anesthesia, statistics from the 1980s still showed anesthesia-related mortality rates in children that were three to four times higher than in the general patient population, although the mortality rates in children had decreased considerably and appeared to have reached a plateau (Keenan and Boyan, 1985; Gibbs, 1986; Olsson and Hallen, 1988).
As part of a study of closed malpractice claims by the Committee on Professional Liability of the ASA, Morray and others (1993) compared pediatric and adult closed claims and found a different distribution of serious outcomes in children compared with those in adults. Of 2400 closed malpractice claims, 238 (10%) were in the pediatric age group (15 years old or younger). A majority of cases involved children younger than 3 years of age, and 28% of all pediatric cases involved infants younger than 1 year of age. Respiratory events (mostly inadequate ventilation) were more common than among adult claims (43% vs. 30%), and mortality was higher (50% vs. 35%), mostly attributable to inadequate ventilation. Anesthesia care was judged inadequate more often. The authors concluded that 89% of the pediatric claims that were related to inadequate ventilation could have been prevented with proper monitoring through the use of pulse oximetry and capnography (Morray et al., 1993). Jimenez and others (2007) reviewed 532 pediatric claims from 1973 to 2000. They concluded that claims for death (41%) and brain damage (21%) remained the dominant injuries in pediatric anesthesia claims in the 1990s. Half of the claims in 1990 to 2000 involved patients 3 years old or younger, and one fifth of the patients had ASA PS scores of 3 to 5. Cardiovascular (26%) and respiratory (23%) events were the most common damaging events. The proportion of claims reported as preventable by better monitoring decreased to 16% in the 1990s.
Analysis of anesthesia-related incidents reported to the Australian Incident Monitoring Study (AIMS) showed almost identical characteristics among pediatric age groups (van der Walt et al., 1993). Of the first 2000 cases reported, 10% involved infants and children. Incidents involving respiratory and breathing circuit systems accounted for nearly half of the adverse incidents. As with the ASA Closed Claims Project, the Australian reviewers estimated that 89% of all applicable problems in AIMS could have been detected and potentially prevented by the combination of pulse oximetry and capnography (van der Walt et al., 1993).
A study from Singapore, based on a QA database, reports no fatalities among 10,000 consecutive general pediatric anesthetic procedures from 1997 to 1999 (Tay et al., 2001). A 2004 QA database study from Hôpital d’Enfants Armand Trousseau in Paris also reports zero mortality among 24,165 general anesthesia procedures in children between 2000 and 2002 (Murat et al., 2004). On the other hand, from the Pediatric Perioperative Cardiac Arrest (POCA) Registry in the United States between 1994 and 1997, the anesthesia-related mortality rate was estimated to be 0.36:10,000 (Morray et al., 2000) (see related section). Obviously, a large-scale prospective and longitudinal study is needed to determine the overall pediatric anesthesia-related mortality in the early 21st century.
Anesthesia-related morbidity in infants and children
Perioperative Cardiac Arrests
Incidences of POCA have been reported from North America, Europe, and Australia. Estimated incidence of cardiac arrests ranged 17 to 24:10,000, and as with the mortality rates, the rates are three to 10 times higher in infants than in older children (Olsson and Hallen, 1988; Tiret et al., 1988; Cohen et al., 1990). Studies by Keenan and Boyan (1985) and by Morgan and others (1993) also showed higher incidences of cardiac arrest in younger children (younger than 10 to 12 years) than in older children. Most common causes leading to cardiac arrest involved respiratory and cardiovascular systems and included relative drug overdose, vagal stimulation, hypoventilation, and succinylcholine-induced asystole.
Keenan and others (1991) reported the effect of specialty training in pediatric anesthesia on the safety of children, especially in infants. In a single university hospital setting, the incidence of POCA in infants younger than 1 year of age was 19:10,000 with mortality when residents were supervised by nonpediatric attending anesthesiologists, whereas no cardiac arrest occurred when pediatric anesthesiologists were in charge.
Braz and others (2006) looked at the causes of POCA in children at a teaching hospital in Brazil. They reviewed 15,253 anesthesia procedures that took place between 1996 and 2004. There were 35 cardiac arrests (22.9:10,000) and 15 deaths (9.8:10,000). They identified seven anesthesia-related cardiac arrests but no deaths. The main causes of anesthesia-related cardiac arrest were respiratory events (71.5%) and medication-related events (28.5%). Major risk factors for cardiac arrest were neonates and children under 1 year of age with an ASA PS of 3 or poorer, emergency surgery, and general anesthesia.
Flick and others (2007) reviewed pediatric cardiac arrest data from 1998 to 2005 at the Mayo Clinic. A total of 92,881 anesthetics were administered to children under the age of 18 for noncardiac and cardiac procedures during the study period. The incidence of POCA and mortality during noncardiac procedures was 2.9:10,000 and 1.6:10,000, and the incidence of cardiac arrest during cardiac procedures was 127:10,000. The incidence of POCA attributable to anesthesia was 0.65:10,000, representing 7.5% of the 80 POCA. Both cardiac arrests and mortality were highest among neonates undergoing cardiac procedures. Regardless of procedure type, most patients who experienced POCA (88%) had congenital heart disease. Factors found to be associated with mortality included higher ASA PS, age, the need for mechanical ventilation before surgery, and the cause of the POCA.
Pediatric Perioperative Cardiac Arrest Registry
In order to accurately estimate the incidence of cardiac arrests and adverse outcomes, the Pediatric POCA Registry was formed in 1994 under the combined auspices of the ASA Committee on Professional Liability, the Quality Assurance Committee of the Section on Anesthesiology of the American Academy of Pediatrics (AAP) (Morray, 2004). The registry included 63 institutions, of which 75% were university hospitals and 40% were children’s hospitals. All cardiac arrests requiring cardiopulmonary resuscitation during the immediate perioperative period are eligible for inclusion. During the first 4 years of the registry (1994 to 1997), participating institutions administered an estimated total of 1,089,200 anesthetics to children younger than 18 years old (Morray et al., 2000). A total of 289 cardiac arrests were registered, of which 150 cases were considered as anesthesia-related. The mean overall incidence of anesthesia-related cardiac arrest was 1.4:10,000 with a mortality rate of 26% (0.36:10,000). Of the total anesthesia-related cardiac arrests, 55% occurred in infants younger than 11 months of age (Morray et al., 2000).
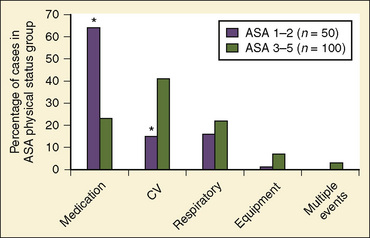
Of the major causes of anesthesia-related cardiac arrests, medication-related (37%) and cardiovascular causes (32%) were most common, together accounting for 69% (Table 40-4). In contrast, the respiratory causes represented only 20%, a marked reduction from the incidence of 43% reported by the ASA Closed Claim Project (Morray et al., 2000). Equipment-related causes comprised 7% of the total (Morray et al., 2000). With regard to the patients’ physical status, 33% were those with ASA PS 1 and 2, a significant decrease from earlier studies of pediatric mortality (57% of deaths), a significant improvement and a move in the right direction, although the percentage is still too high (Graff et al., 1964). Of medication-related cardiac arrests, cardiovascular depression with halothane alone or in combination with other drugs (mostly opioids) accounted for 66% of all medication-related arrests. In healthy children with ASA PS 1 and 2, 64% of cardiac arrests were medication-related in comparison with 23% in those with ASA PS 3 to 5 (Fig. 40-1) (Morray et al., 2000; Mason, 2004). Among the patients who sustained anesthesia-related cardiac arrest in the POCA Registry, death was associated most strongly with an ASA PS 3 to 4 and emergency surgery (Morray et al., 2000). Similar correlations between cardiac arrest or death and ASA PS 3 to 4 were found in the earlier study by Keenan and Boyan (1985).
TABLE 40-4 Mechanisms of Cardiac Arrest
| Mechanism | Number of Cardiac Arrests |
| Medication-related inhalation agents | 55 (37%) |
| Halothane alone | 26 (46%) |
| Halothane plus an intravenous medication | 11 (20%) |
| Sevoflurane alone | 2 (4%) |
| Intravenous medications | |
| Single | 5 (9%) |
| Combination | 5 (9%) |
| Intravenous injection of local anesthetic | 5 (9%) |
| Succinylcholine-induced hyperkalemia | 1 (2%) |
| Cardiovascular | 48 (32%) |
| Presumed cardiovascular, unclear etiology | 18 (38%) |
| Hemorrhage, transfusion related | 8 (17%) |
| Inadequate/inappropriate fluid therapy | 6 (13%) |
| Arrhythmia | 5 (10%) |
| Hyperkalemia | 4 (8%) |
| Air embolism | 2 (4%) |
| Pacemaker related | 2 (4%) |
| Vagal response | 1 (2%) |
| Pulmonary hypertension | 1 (2%) |
| Tetralogy hypercyanotic spell | 1 (2%) |
| Respiratory | 30 (20%) |
| Laryngospasm | 9 (30%) |
| Airway obstruction | 8 (27%) |
| Difficult intubation | 4 (13%) |
| Inadequate oxygenation | 3 (10%) |
| Inadvertent extubation | 2 (7%) |
| Presumed respiratory, unclear etiology | 2 (7%) |
| Inadequate ventilation | 1 (3%) |
| Bronchospasm | 1 (3%) |
| Equipment related | 10 (7%) |
| Central line | 4 (40%) |
| Breathing circuit | 2 (20%) |
| Peripheral intravenous catheter | 1 (10%) |
| Other | 3 (30%) |
| Multiple events | 5 (3%) |
| Hypothermia | 1 (<1%) |
| Unclear etiology | 1 (<1%) |
Modified from Morray JP et al.: Anesthesia-related cardiac arrest in children: initial findings of the Pediatric Perioperative Cardiac Arrest (POCA) Registry, Anesthesiology 93:614, 2000.
Since the last publication of the POCA Registry that was based on data between 1994 and 1997, more than 200 POCA cases have been added to the registry (from 2000 to 2003), and about one half of these cardiac arrests were found to be anesthesia-related (Morray, 2004). In a preliminary report on this new series of cardiac arrests, the cause profile has changed considerably from that of 1994 through 1997 (Fig. 40-2) (Morray, 2004). Medication-related cardiac arrests decreased markedly, from 37% to 12% of the total causes, primarily because of the near disappearance of cardiovascular depression by inhaled anesthetics causing cardiac arrest (Morray, 2004). These welcome changes appear to coincide with the replacement of halothane with sevoflurane (with its lower incidence of causing myocardial depression and bradycardia) as an anesthetic of choice for induction,. As the consequence of reductions in cardiac arrests with medication (primarily from halothane), cardiovascular causes of cardiac arrest increased relatively, from 32% to 52%. Hypovolemia from hemorrhage and a metabolic consequence of massive transfusion and resultant hyperkalemia were the common causes of cardiac arrest under this category (Morray, 2004). Also, with a reduction in medication-related cardiac arrest in healthy infants, the incidence of cardiac arrest in patients with ASA PS 1 to 2 declined considerably from 33% to 19%, one of the most remarkable differences between the first and second databases (Table 40-5).
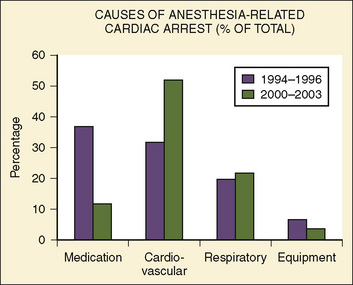
FIGURE 40-2 Causes of anesthesia-related cardiac arrest in children between 1994 and 1996 vs. between 2000 and 2003.
(From Morray JP: Unexpected cardiac arrest in the anesthetized child. Presented at the Society of Pediatric Anesthesia Spring Meeting, March 4-7, 2004.)
TABLE 40-5 Demographic Data from Pediatric POCA Registry Cases, 1994 to 1997 vs. 2000 to 2003
| 1994 to 1997 | 2000 to 2003 | |
| ASA PS | ||
| 1 | 15% | 4% |
| 2 | 18% | 15% |
| 3 | 37% | 46% |
| 4 | 27% | 22% |
| 5 | 2% | 13% |
| Age | ||
| <1 mo | 15% | 13% |
| 1 to 5 mo | 28% | 25% |
| 6 to 11 mo | 13% | 10% |
| 12 mo to 5 yr | 31% | 25% |
| 6 to 18 yr | 13% | 27% |
| Emergency surgery | 21% | 30% |
| Mortality | 26% | 27% |
POCA, Perioperative cardiac arrest; ASA PS, American Society of Anesthesiologists physical status.
Modified from Morray JP: Unexpected cardiac arrest in the anesthetized child. Presented at the Society of Pediatric Anesthesia Spring Meeting, March 4-7, 2004.
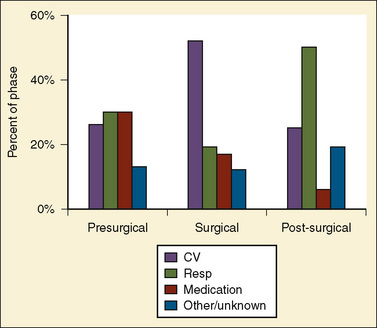
Bhananker and others (2007) subsequently published a study related to cases submitted to the POCA registry between 1998 and 2004. During that time, the registry received 397 reports of POCA in children. Of these cardiac arrests, 193 were judged as anesthesia related. Three quarters of the anesthesia-related arrests occurred in patients of ASA PS 3 to 5. Between 1998 and 2004, cardiovascular causes of cardiac arrest accounted for the highest proportion of anesthesia-related cardiac arrests (41%), in part because of a dramatic decrease in medication-related cardiac arrest. Among these, the most common identifiable cause was hypovolemia related to blood loss. The majority of these cardiac arrests resulted from blood loss that occurred during either spinal fusion or craniotomy and craniectomy. The most common anesthesia-related factors were underestimation of blood loss (48%) and inadequate venous access (22%). As reported in the preliminary communication by Morray (2004) on cases from the POCA Registry between 2000 and 2003, medication-related cardiac arrests decreased dramatically to 18% of all cardiac arrests (12% for 2000 to 2004, see above) from the 37% reported from 1994 to 1997, apparently because of the decrease in the use of halothane for induction of anesthesia. However, it is important to remember that sevoflurane is also a cardiac depressant, and cardiac arrests related to its effects have been identified in the registry. Most cardiac arrests occurred during anesthesia maintenance (58%). Nearly one quarter (24%) occurred in the induction or preinduction phase, and 19% occurred during emergence, transport, or recovery (Fig. 40-3). Eight of 10 cardiac arrests caused by electrolyte imbalance were caused by hyperkalemia from the transfusion of stored blood. The use of fresh blood cells and saline washing of irradiated blood may help in reducing the incidence of transfusion-associated hyperkalemia. Equipment-related cardiac arrests accounted for 5% of the anesthesia-related incidents, and half of these were secondary to central venous catheter complications. Six percent of the causes of cardiac arrest were unknown. Mortality after anesthesia-related cardiac arrest was 28%. The only factors predictive of mortality after cardiac arrest were ASA PS and emergency surgery.
Information about POCA in children (younger than 18 years) between 1988 and 2005 was reported from the Mayo Clinic (Flick et al., 2007). Out of a total of 92,881 anesthesia procedures, of which about 5% were for the repair of congenital heart disease, the incidence of POCA for noncardiac procedures were 2.9:10,000 and the incidence during the cardiac surgery was 127:10,000. The incidence of cardiac arrest attributable to anesthesia, however, was 0.65:10,000 procedures, representing 7.5% of all POCA, much lower than in some of the published reports. Both the incidence of arrest as well as mortality rates were highest among neonates (younger than 30 days’ postnatal life) undergoing cardiac procedures (POCA: 435:10,000; mortality: 389:10,000) (Flick et al., 2007).
Other Perioperative Adverse Events
Computerized data acquisition on nonfatal adverse outcome has become commonplace in most hospitals for QA or quality improvement (QI); such information in pediatric anesthesia has started to appear in the literature. Excellent reviews on this subject have been published (Holzman, 1994; Duncan, 1995).
Cohen and others (1990) reviewed perioperative adverse events in over 29,000 children between 1982 and 1987 at Winnipeg Children’s Hospital. Unlike the adult surgical population, a majority of children (70%) were healthy and had no preoperative medical problems. Infants younger than 1 year of age, particularly those younger than 1 month of age (61% of whom underwent intraabdominal, intrathoracic, or major cardiovascular surgery), had a significantly higher intraoperative incidence of airway obstruction and other adverse respiratory events (9.4%) and hypotension (3.9%) than did older children. Among children 1 to 10 years of age, the most common problem was arrhythmias (3.9% to 9.3%). In the recovery room, infants younger than 1 month of age had hypotension (13.9%), respiratory events (11.6%), and abnormal temperature (4.7%). In older children, the most common adverse event in the recovery period was vomiting (5.9%), followed by airway obstruction (3.2%). This study was performed during the pre-sevoflurane era, when essentially all inhalation inductions were performed with halothane, with potent myocardial depression and bradycardia (Table 40-6).
A report from Hôpital d’Enfants Armand Trousseau in Paris was based on a QA database involving over 24,000 pediatric anesthesia cases for a 30 months between 2000 and 2002, when halothane had been completely eliminated from clinical use (Murat et al., 2004). Although this database did not include open-heart and neurosurgical cases, the nature of adverse events and their incidence have changed considerably. As a whole, respiratory events were most common, representing 53% of all intraoperative events (Table 40-7). As with other reports, respiratory events were more common among infants (3.6:10,000 vs. fewer than 1.5:10,000 in older children); in ear, nose, and throat (ENT) surgery than in other surgery; in children who were intubated vs. those who were not intubated, and in those with ASA PS 3 to 5 vs. PS 1 or 2 (Murat et al., 2004). Cardiac events represented 12.5% of all intraoperative events and were mostly observed in sick children (ASA PS 3 to 5).
TABLE 40-7 Respiratory and Cardiac Adverse Events Observed During Anesthesia and in PACU by Age Group
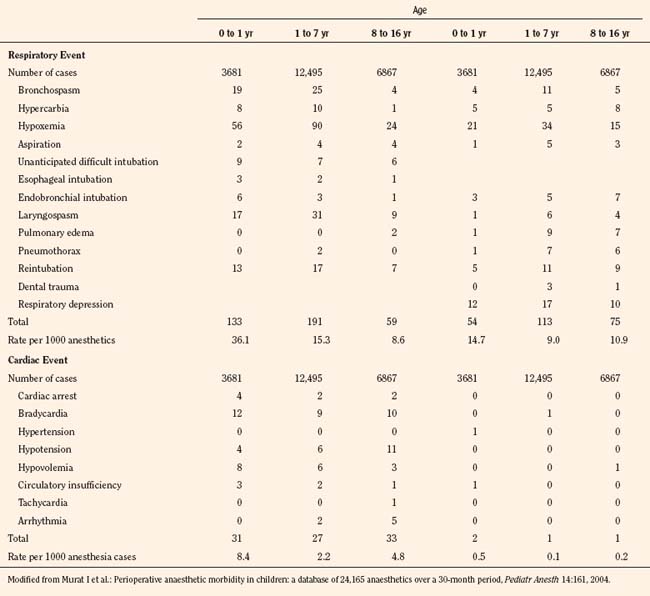
In contrast to earlier reports, the incidence of bradycardia was greatly decreased (13:10,000) and arrhythmias essentially disappeared. There were eight cardiac arrests (3.3:10,000), of which five children were in the ASA PS 3 to 5 category and four were infants 6 months old or younger (Table 40-7). There were no anesthesia-related deaths (Murat et al., 2004). Vomiting was the most common adverse event postoperatively, with an overall incidence of 6%. As with previous studies, vomiting was more common in older children than in infants and occurred more often after ENT surgery compared with other surgery and in children who were intubated vs. those who were not (Murat et al., 2004). Similarly, based on QA data of 10,000 surgical cases, Tay and others (2001) in Singapore found critical perioperative incidents four times higher in infants younger than 1 year of age than in older children (8.6% vs. 2.1%). Respiratory events were most common (77.4%) with laryngospasm accounting for 35.7%. There were no anesthesia-related deaths (Tay et al., 2001).
Down syndrome is the most common autosomal chromosomal disorder in humans. Children with Down syndrome have a number of characteristics that place them at high risk for anesthesia complications, including craniofacial and cardiac anomalies. A study of 488 patients undergoing 930 procedures revealed several anesthesia-related complications. The most common complications were severe bradycardia (3.7%), natural airway obstruction (1.8%), difficult intubation (0.5%), postintubation croup (1.8%), and bronchospasm (0.4%) (Borland et al., 2004). The rates of bradycardia, obstruction, and postintubation croup were statistically significant and more than twice the rate of patients without Down syndrome, suggesting the need for increased vigilance in these patients.
Bradycardia
An outcome study from the Medical College of Virginia examined the incidence of bradycardia in nearly 8000 children younger than 4 years of age (Keenan et al., 1994). Bradycardia (fewer than 100 beats per minute) was more common in infants (1.27%) and decreased with age. The incidence in the group of children who were 4 years old was only 0.16%. Causes of bradycardia included disease or surgery (35%), inhalation anesthesia (35%), and hypoxemia (22%). Of these children, hypotension occurred in 30%, asystole or ventricular fibrillation in 10%, and death in 8%. Significant associated factors predisposing children to bradycardic events, based on multiple logistic regression analysis, were ASA PS, emergency surgery, duration of surgery (longer than 4 hours), and the absence of a trained pediatric anesthesiologist supervising the anesthetic management (Keenan et al., 1994).
Laryngospasm and Bronchospasm
The incidences of laryngospasm and bronchospasm have been studied in a series of large population studies in Stockholm by Olsson and Hallen (1984, 1988). The incidence of laryngospasm in children younger than 9 years of age was 1.7%. The presence of respiratory infection raises the incidence to 9.6%. The incidence of laryngospasm was also increased in patients with obstructive lung disease (6.4%) and in those with a history of previous anesthetic complications (5.5%). The incidence of bronchospasm in the same age group increased from 0.4% to 4.1% in those with respiratory infection. The incidence of bronchospasm was also elevated (2.4%) in patients at high risk (ASA PS 3 or higher) (Olsson, 1987).
Up to 40% of children preparing for anesthesia have an upper respiratory tract infection (URI). Possible effects of recent or current URIs and the incidence of respiratory events have been studied by a number of investigators using parental interviews or written questionnaires. Of more than 1500 children, Schreiner and others (1996) found that patients who developed laryngospasm were more than twice as likely to have an active URI than were patients in the control group without URIs. A survey of more than 2000 children by Parnis and others (2001) did not find statistically significant differences in the long-term outcome of children with a recent history of URI. They did, however, find that orotracheal intubation was associated with an increased probability of respiratory complications compared with the use of a face mask or laryngeal mask airway (LMA). Similarly, in more than 1000 children, Tait and others (2001) found no difference between children with active or recent URIs vs. asymptomatic children, with respect to the incidence of laryngospasm, bronchospasm, or long-term respiratory sequelae. However, children with current or recent URIs had significantly more overall adverse respiratory events, including breath-holding and major desaturation (arterial oxygen saturation [SpO2] of less than 90%). Independent risk factors for adverse respiratory outcome in children with active URIs included tracheal intubation (younger than 5 years of age), history of prematurity, reactive airways disease, parental smoking, surgery involving the airway, and the presence of copious secretions and nasal congestion (Tait et al., 2001). A logistic regression analysis was created to look at the relationship between preoperative URI symptoms and adverse events during emergence from anesthesia. No association was found between particular URI symptoms and the rate of adverse events, but adverse events were increased if peak URI symptoms had occurred within the preceding 4 weeks (Homer et al., 2007).
The LMA has been advocated as an alternative to tracheal intubation for airway management in children with URIs. Von Ungern-Sternberg and others (2007) studied over 800 children having elective surgery with an LMA. A medical history of recent URI within the 2 weeks before anesthesia approximately doubled the risk of laryngospasm, oxygen desaturation, and coughing both intraoperatively and in the recovery room. This risk was further increased in younger children and in children undergoing ENT surgery (Tait et al., 2001). Flick and others (2008) reviewed 130 cases of laryngospasm in children at the Mayo Clinic and found that the use of an LMA was associated with laryngospasm even when adjusted for the presence of upper respiratory tract infections and airway anomaly.
Passive smoke exposure was studied in 405 children undergoing mask anesthesia procedures. The incidence of airway complications during anesthesia or postanesthesia recovery was significantly higher in children with passive smoke exposure. Intraoperative laryngospasm and airway obstruction were 4.9 and 2.8 times, respectively, more likely in children with passive smoke exposure (Jones and Bhattacharyya, 2006). Perioperative assessment of children undergoing surgery should include screening for passive smoke exposure to alert anesthesia providers to potential complications.
Aspiration
Studies before the 1970s reported high morbidity and mortality from pulmonary aspiration of gastric contents (Mendelson, 1946). The Baltimore Anesthesia Study Committee reported a mortality rate of 39% in children associated with pulmonary aspiration (Graff et al., 1964) (see Chapter 13, Induction, Maintenance, and Recovery). Studies reported since the 1980s, however, indicate marked improvements in outcome.
From a computer database covering the years between 1967 and 1985, Olsson and others (1986) reviewed more than 185,000 anesthesia cases in all ages and identified 83 cases of pulmonary aspiration of gastric contents (4.7:10,000 cases). The rate of gastric aspiration in children younger than 9 years of age (8.6:10,000) was nearly three times higher than that in young adults (20 to 49 years old). In 47% of patients with aspiration, pneumonia or atelectasis developed, as confirmed by chest radiograph. The mortality rate in children was relatively low (0.2:10,000) (Olsson et al., 1986). Risk factors associated with aspiration included the skill and experience of anesthetists, a number of coexisting diseases, ASA PS 3 to 5, emergency surgery, nighttime operation, history indicating an increased risk of regurgitation (e.g., esophageal disease, pregnancy), and difficult intubation. Other high-risk categories included children with intestinal obstruction, increased intracranial pressure, increased abdominal pressure, and obesity. Incidence of gastric aspiration was even lower in studies from the French-speaking countries (1.0:10,000) and from Norway (2.9:10,000) in the 1980s (Tiret et al., 1988; Mellin-Olsen et al., 1996). No fatalities were reported.
Borland and others (1998) studied the incidence and outcome of perioperative aspiration during the 5 years between 1988 and 1993 involving over 50,000 general anesthetic cases at Children’s Hospital of Pittsburgh. They identified 52 cases of aspiration (10.2:10,000 cases), of which 25 patients aspirated gastric contents (4.9:10,000) (the rest were blood or pharyngeal secretions). Approximately 80% of aspirations occurred during induction. Most patients were treated aggressively with fiberoptic bronchoscopy through the endotracheal tube (ETT), removal of solid particles, and continuous positive pressure ventilation. Most patients had radiographic evidence of aspiration (e.g. infiltration, pneumonia, atelectasis, or pulmonary edema), but fulminant chemical pneumonitis secondary to aspiration, as reported in early publications, was absent (Mendelson, 1946). No death was attributable to aspiration. Among the different pediatric age groups, the incidence of aspiration was highest among children 6 to 11 years of age (0.22%). Several risk factors for intraoperative aspiration were identified: ASA PS 3 or higher, a history of previous esophageal surgery, and patients with previous chemotherapy undergoing central venous catheter (Broviac catheter) placement. Twenty-nine percent of these children were kept intubated in the postanesthesia care unit (PACU) for several hours or longer, but only 23% of these patients stayed overnight. None of these children developed clinically significant pneumonia, and there were no deaths (Borland et al., 1998).







Full access? Get Clinical Tree


