Figure 16.1. Deep anatomy of the sciatic nerve. The nerve exits the pelvis through the sciatic notch and travels behind the femur to bifurcate just above the knee into the tibial and common peroneal nerves.
F. The PFCN is a purely sensory nerve derived from the ventral rami of the S1 to S3 spinal nerves. Although deep to the gluteus maximus, the PFCN is located medial and superficial to the sciatic nerve. At this level, the PFCN gives off inferior cluneal branches to supply the skin of the lower buttock and perineal branches to supply the skin on the posterior aspect of the external genitalia. The PFCN emerges from the inferior edge of the gluteus maximus to lie within the subcutaneous tissue and descends further along the posterior aspect of the thigh and lower leg to supply the skin of the posterior aspect of the thigh and calf.
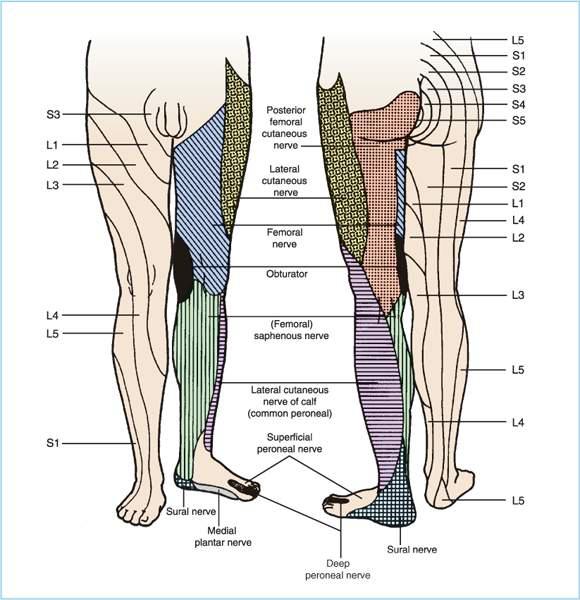
Figure 16.2. Dermatomal and peripheral nerve branches of the leg.
II. Indications
The primary indication for sciatic nerve block is to provide operative anesthesia to the lower leg, ankle, or foot. In order to provide complete anesthesia to the lower leg, the saphenous nerve must also be blocked to anesthetize the skin of the medial lower leg, which is not supplied by the sciatic nerve. In contrast, a continuous sciatic perineural catheter from the level of the sacral plexus down to the popliteal fossa will provide excellent postoperative analgesia for painful procedures of the lower leg such as hallux valgus repair, below the knee amputations, and open reduction-internal fixation of ankle and lower leg fractures. For operative procedures of the femur and knee joint, a sciatic nerve block in combination with a psoas compartment block will provide complete surgical anesthesia for procedures such as total knee replacement, anterior cruciate ligament reconstruction, above-the-knee amputations, and open reduction-internal fixation of femur fractures. A more proximal sciatic nerve block at the gluteal or subgluteal region is commonly indicated for severe knee pain after total knee replacement despite a successful femoral nerve block. For operative procedures of the hip joint such as total hip replacement, only a parasacral approach in combination with a psoas compartment block will provide complete surgical anesthesia.
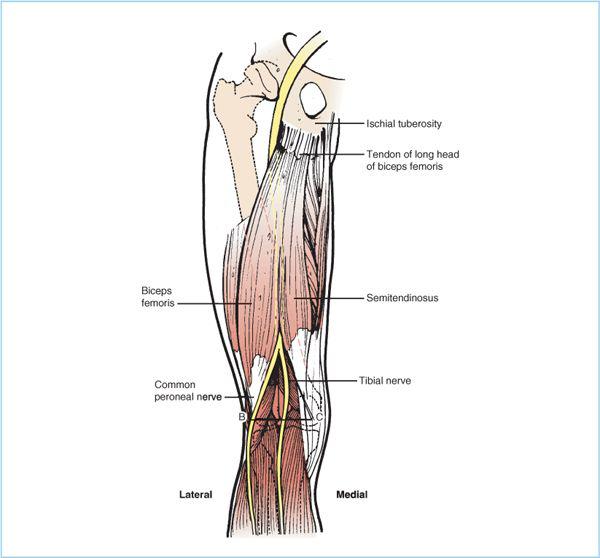
Figure 16.3. Relationship of the sciatic nerve to the muscles of the posterior thigh.
III. Choice of local anesthetic
The choice of local anesthetic for the sacral plexus-sciatic nerve block is dependent on the requirements for onset of anesthesia and duration of analgesia for single-injection techniques, as well the anatomic location where the block is performed. The sciatic nerve block is different from the individual nerve blocks of the lumbar plexus, as the anatomic location of the sciatic nerve block has a significant impact on the total local anesthetic mass requirements.
A. Specifically, the proximal approaches to sciatic nerve block consistently have a shorter latency to complete anesthesia (5) and lower total anesthetic requirement compared with the distal popliteal approaches (6,7). Additionally, epinephrine is not routinely recommended for proximal sciatic nerve block because of the possibility of epinephrine exacerbating ischemic injury due to stretching or sitting on the anesthetized sciatic nerve with a prolonged block.
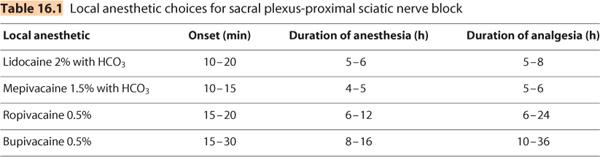
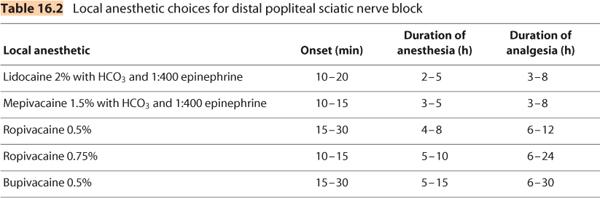
B. With the advent of continuous peripheral perineural catheter techniques, the anesthesiologist has the advantage of providing a rapid onset of surgical block by injection of the shorter-acting local anesthetics (Table 16.1 and 16.2) through the needle or catheter tip (the primary anesthetic block). Subsequently, an infusion of a dilute local anesthetic that possesses sensory-motor dissociation (the most commonly used being ropivacaine 0.2% or bupivacaine 0.125%) may be used to provide the optimal balance of postoperative analgesia with less motor block to facilitate postoperative rehabilitation and recovery. Alternatively, if a central neuraxial technique is chosen as the primary anesthetic, a loading dose (10–15 mL) of the analgesic infusion of ropivacaine 0.2% may be started intraoperatively. The typical postoperative regimen consists of running the analgesic infusion at 4 to 8 mL/h with or without a patient-controlled bolus of 2 to 3 mL every 20 minutes.
IV. Techniques
The sacral plexus-sciatic nerve is the longest nerve in the body and may be blocked at the sacral plexus, gluteal, subgluteal, and popliteal levels. Although, posterior approaches to the sciatic nerve are the most commonly performed techniques, the sciatic nerve may also be blocked from an anterior approach in the proximal thigh, as well as lateral approaches extending from the mid-thigh to just above the popliteal fossa. The choice of technique will be dictated by the requirements for surgical anesthesia and postoperative analgesia, as well as the ability of the patient to assume the appropriate position. Although posterior approaches are the most commonly performed techniques, patient factors (morbid obesity, painful fractures, and the presence of casts-fixation devices) may preclude patients from assuming either the lateral decubitus or prone position. Therefore, either anterior or lateral approaches provide alternative techniques when the patient cannot assume the lateral or prone position. As with lumbar plexus blocks, both single-injection and continuous catheter techniques are available for all approaches. Additionally, both traditional peripheral nerve stimulator (PNS) and ultrasound-guided (USG) approaches will be described. Paresthesia techniques are not recommended for sacral-sciatic nerve blocks.
A. Parasacral nerve block approach (PSNB). The parasacral technique blocks the sacral plexus proximal enough to reliably provide anesthesia to the sciatic and PFCN, as well the superior and inferior gluteal nerves, nerve to the quadratus femoris, and the pudendal nerve (8, 9) contained between the piriformis muscle posterior and the pelvic fascia anterior. Therefore, it can be described as true sacral plexus block. In contrast to slightly more distal gluteal approaches, the PSNB approach (in conjunction with a psoas compartment block) can provide true unilateral anesthesia for hip surgery (10,11). The only two landmarks that are important are the posterior superior iliac spine (PSIS) and IT (Figure 16.4). Therefore, it is a relatively easy block to learn with a high success rate (12). The relative disadvantages of this block include the proximity of structures anterior to the sacral plexus (iliac vessels, ureter, and bladder) and the associated weakness of the hamstrings and adductor muscles. Therefore, for procedures of the lower leg, a more distal approach at the popliteal fossa maybe more appropriate.
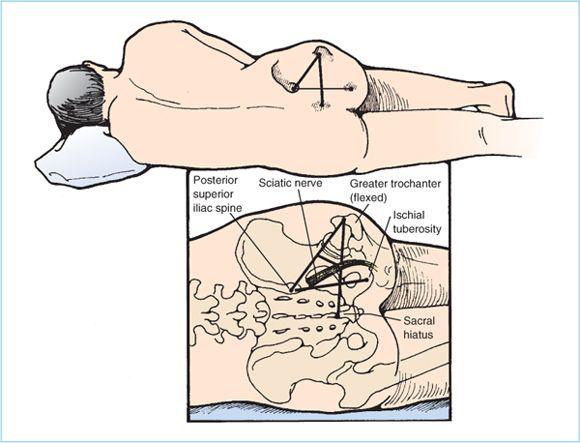
Figure 16.4. Landmarks for posterior sciatic block at the hip.
1. Patient position. The patient is placed in the lateral position with a slight forward tilt with the operative side to be blocked uppermost. The dependent limb should be straight and the operative limb should be flexed slightly at both the hip and knee.
2. The external landmarks are the PSIS and the IT. A line is drawn connecting the PSIS and IT corresponding to the sacrotuberous ligament. The proposed needle insertion site is along this line 6 cm caudal to the PSIS, which allows access to the sacral plexus as it passes through the greater sciatic foramen.
3. After aseptic skin preparation and draping followed by local anesthetic skin infiltration of the proposed needle insertion site, a 100-mm (4-in.) 21-gauge stimulating needle is attached to a PNS (typical settings of 1.5–2.0 mA, 2 Hz, 100 μs) and a syringe of local anesthetic.
4. The stimulating needle is advanced perpendicular to the skin in a parasagittal plane until a sacral plexus evoked motor response (EMR) is elicited at a current output between 0.2 and 0.5 mA. Acceptable EMR includes not only plantar flexion (TN) or dorsiflexion (CPN) of the foot or toes but also hamstring contractions (biceps femoris, semimembranosus, and semitendinosus) as acceptable endpoints.
5. The upper margin of the greater sciatic notch may be encountered as the needle is advanced, which serves as a gauge of further needle advancement. In this case, the needle is introduced slightly caudal along the same line. The needle is advanced in the same initial direction until an acceptable EMR is elicited. The needle should not be advanced 2.5 cm beyond the depth of bony contact (8).
6. After the final needle position is obtained and an initial 3-mL test dose to confirm the absence of intravascular location of the local anesthetic injection, a total of 20 mL of local anesthetic is incrementally injected with frequent intermittent aspirations to reduce the risk of intravascular injection. Typical onset time for sensory and motor anesthesia is 10 to 20 minutes depending on the total mass of local anesthetic injected and the EMR elicited. Clinical studies have demonstrated that TN EMR (plantar flexion at the foot or ankle, as well contraction of the medial hamstring muscles [semimembranosus and semitendinosus]) predicts a higher success rate of anesthesia (13).
7. A continuous catheter technique can be used to provide extended duration analgesia. The initial needle insertion site and approach are the same as the single-injection technique. A larger bore (17- to 18-gauge) insulated stimulating Tuohy needle is typically used to localize the sacral plexus. After localization of the sacral plexus and injection of the local anesthetic, the needle is angulated slightly caudal to facilitate catheter passage. A 19- to 20-gauge catheter is inserted through the Tuohy needle and advanced no more than 2 cm past needle tip. The needle is then withdrawn over the catheter and the latter fixed in place with a sterile clear adhesive dressing. The proximal end of the catheter is then connected to an automated infusion pump.
8. Clinical pearls. If there is no EMR at a needle depth of 10 cm, the needle direction should be redirected caudally 5 to 10 degrees along the same line. Bony contact is preferred as this serves as an added safety step in judging the adequate depth of needle insertion.
B. Sciatic nerve block, posterior transgluteal approach. This is the classic technique of sciatic nerve block as initially described by Labat and later modified slightly by Winnie. This approach shares similar indications for both single-injection and continuous perineural catheter techniques, with the exception of not consistently blocking the sacral plexus branches (nerve to the quadratus femoris, superior and inferior gluteal nerves) required for complete anesthesia for hip surgery.
1. Patient position. The patient is placed in the lateral decubitus position with a slight forward tilt, hips flexed with the operative side to be blocked uppermost. The dependent limb should be straight and the operative limb should be flexed slightly at both the hip and knee.
2. External landmarks. The three palpable landmarks include the PSIS, the superior-most aspect of the GT, and the sacral hiatus. A line is drawn between the PSIS and GT. A second line is drawn from the SH and the GT. At the midpoint of the line between the PSIS and GT, a perpendicular line is drawn until it intersects with the line between the SH and GT (Figure 16.4). This third line is known as the Labat line and typically intersects the line between the SH and GT at a distance of 4 to 5 cm, and corresponds to the proposed needle insertion point. The proposed needle insertion point corresponds to the lateral border of the sciatic notch.
3. After aseptic skin preparation and draping followed by local anesthetic infiltration of the proposed needle insertion point, a stimulating needle (typically 100–150 mm [4–6 in.], 20–21 gauge) is slowly advanced at right angles to the spherical skin plane of the buttocks. The stimulating needle is attached to a PNS (typical settings of 1.5–2.0 mA, 2 Hz, 100 μs) and a syringe of local anesthetic.
4. The skin and underlying muscular/adipose tissue of the buttock is highly mobile and the skin-to-nerve distance may be substantial, especially in obese patients. Therefore, the fingers of the palpating hand should be firmly pressed on the needle insertion site to decrease the skin-to-nerve distance and skin should be stretched between the index and middle finger to allow greater precision in needle movement.
5. As the stimulating needle is advanced, the initial EMR observed may be gluteus muscle contractions, indicating that the needle tip is still too shallow. The needle is advanced further until EMR of the hamstring muscles, or plantar flexion or dorsiflexion at the ankle or foot are observed. The final position of the needle tip is judged to be adequate when EMR are elicited at 0.2 to 0.5 mA.
6. If the initial needle pass does not result in nerve localization, then a systematic approach is recommended for needle redirection. If bone is encountered, the depth should be noted as this likely represents the lateral border of the sciatic notch and the sciatic nerve will be located slightly deeper and more medial. Therefore, the needle is withdrawn to just below the skin and redirected with a slight medial angulation and advanced until the desired EMR is elicited. If this step does not elicit a desired EMR, mentally visualize the course of the sciatic nerve as it emerges from the medial side to the center of the sciatic notch and then curves downward to course midway between the GT and IT. At this point, the needle is redirected in a systematic manner in 5- to 10-degree increments cephalad or caudad along the Labat line.
7. After the final needle position is obtained and an initial 3-mL test dose to confirm the absence of intravascular location of the local anesthetic injection, a total of 25 to 35 mL of local anesthetic is incrementally injected with frequent intermittent aspirations to reduce the risk of intravascular injection. Typical onset time for sensory anesthesia is 25 to 35 minutes depending on the total mass of local anesthetic injected and the EMR elicited. Seeking an EMR of both branches (TN and CPN) of the sciatic nerve and dividing the total local anesthetic injection equally between the two nerves improves both onset time and success of complete sciatic nerve block (14).
8. A continuous catheter technique may be utilized to provide extended duration analgesia. The initial needle insertion site and approach are the same as the single-injection technique. A larger bore (17- to 18-gauge) insulated stimulating Tuohy needle is typically used to localize the sciatic nerve. After localization of the sciatic nerve and injection of the local anesthetic, the needle tip is angulated slightly caudal toward the midpoint of the GT and IT to facilitate catheter passage along the course of the sciatic nerve. A 19- to 20-gauge catheter is inserted through the Tuohy needle and advanced no more than 2 cm past the needle tip. The needle is then withdrawn over the catheter and the latter fixed in place with a sterile clear adhesive dressing. The proximal end of the catheter is then connected to an automated infusion pump.
C. Sciatic nerve block, USG posterior subgluteal approach. Although USG sciatic nerve block at the gluteal level may be attempted, it is technically challenging due to the required depth of the sciatic nerve at the ischial spine level, especially in obese patients. A slightly more caudal approach at the level where the sciatic nerve courses between the GT and IT offers several advantages (15). First, the sciatic nerve is likely to be more superficial and inferior to bulkiest portion of the gluteus maximus. Second, the location of the sciatic nerve is consistently observed to be at the midpoint between highly echogenic (and therefore, visible) IT medially and GT laterally. The sciatic nerve is visualized as a hyperechoic, oval to lip-shaped structure found in between the GT and IT. The sciatic nerve is located within the subgluteal space sandwiched directly deep to the fascial plane of the gluteus maximus and superficial to the underlying quadratus femoris muscle (Figure 16.5).
1. Patient position. The patient is placed in the lateral decubitus position with a slight forward tilt, hips flexed with the operative side to be blocked uppermost. The dependent limb should be straight and the operative limb should be flexed slightly at both the hip and knee.
2. Probe selection. A mid to low frequency curved array transducer (2–5 MHz) is typically used for this block. The lower frequency allows for a greater depth of penetration and the curved probe provides a wider field of view required to visualize the GT and IT.
3. Probe placement and sonoanatomy. The ultrasound probe is initially placed at a 90-degree angle to the skin, with the long axis of the probe directly over and parallel to a line drawn between the inner borders of the IT and GT (Figure 16.5).
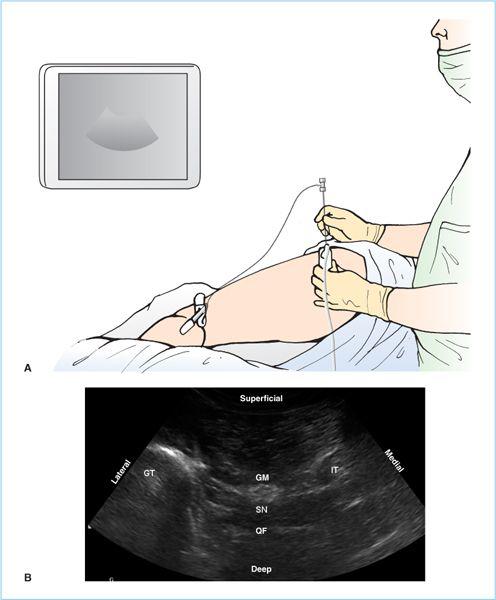
Figure 16.5. Ultrasound visualization of the sciatic nerve (S) in the subgluteal region. The patient lies in the lateral position with the hips and knees flexed. The curved array ultrasound probe is placed at the level of the inferior border of the gluteus maximus (GM) in the middle of the proximal thigh (A). The image is image is adjusted to show the greater trochanter (GT) laterally, the ischial tuberosity (IT) medially, and sciatic nerve (S) will be visualized between these two landmarks, deep to the GM and superficial to the quadratus femoris (QF).
a. Typically, the depth of the sciatic nerve is 5 to 8 cm depending on the body habitus of the patient.
b. The gain and focal point are adjusted to optimize the appearance of the GT, IT, and subsequently the sciatic nerve.
c. At this point, the sciatic nerve often appears as hyperechoic, oval to lip-shaped structure. Slight adjustments in the probe position will enhance the anisotropy of the nerve and optimize its sonographic appearance within the subgluteal compartment. The subgluteal compartment is a fascial compartment bounded medially by the IT and laterally by the GT. The sciatic nerve is sandwiched in between the fascial plane of the gluteus maximus muscle and superficial to the underlying fascial plane of the quadratus femoris muscle (Figure 16.5B).
4. Needling technique
a. After aseptic skin preparation and draping followed by local anesthetic skin infiltration of the proposed needle insertion site, a 100-mm (4-in.) 21-gauge stimulating needle is attached to a PNS (typical settings of 1.5–2.0 mA, 2 Hz, 100 μs) and a syringe of local anesthetic.
b. After placing the target structures in the middle of the screen, the stimulating needle may be placed either lateral to the lateral aspect or medial to the medial aspect of the ultrasound probe. The preferred approach is to place the needle tip lateral to the lateral aspect of the ultrasound probe (Figure 16.5A) and advanced in plane (to the ultrasound beam) at an appropriate angle toward the sciatic nerve. The needle will approach the sciatic nerve from a lateral to medial direction at a relatively steep angle. Therefore, the needle tip may be difficult to see at it approaches the sciatic nerve. Simply injecting a small amount (0.5–1.0 mL) of local anesthetic will result in the formation of a small hypoechoic collection that is easily visible, thereby providing an indirect but useful assessment of needle tip location. The initial typical target site for the perineural needle placement is the space located between the greater trochanter and the lateral aspect of the sciatic nerve. The needle tip may then be adjusted in real time to achieve a circumferential collection of local anesthetic around the sciatic nerve.
c. As the needle tip approaches the sciatic nerve, a visible pop or loss of resistance is seen and felt as the needle tip penetrates the fascial plane of the gluteus maximus. At this point, the PNS may be activated and the location of the needle tip confirmed by the appropriate sciatic nerve EMR. Local anesthetic is injected and local anesthetic distribution deep to the gluteus maximus within the subgluteal space and around the sciatic nerve is observed in real time. Typically, a volume of 15 to 25 mL is all that is required to obtain satisfactory local anesthetic distribution around the sciatic nerve.
5. If a continuous catheter technique is indicated, a larger bore (17- to 18-gauge) insulated stimulating Tuohy needle is typically used for initial placement of the needle tip and local anesthetic within the subgluteal compartment. After local anesthetic distribution (by injection through the needle tip) is ensured the ultrasound probe is placed aside within the sterile field. A 19- to 20-gauge catheter is inserted through the Tuohy needle and advanced no more than 2 to 3 cm past needle tip. At this point, the ultrasound probe is placed over the original site, and an additional 3 to 5 mL of local anesthetic is injected through the catheter while observing for local anesthetic distribution within the subgluteal compartment around the sciatic nerve to ensure correct catheter tip position. The needle is then withdrawn over the catheter and the latter fixed in place with a sterile clear adhesive dressing. The proximal end of the catheter is then connected to an automated infusion pump.
D. Sciatic nerve block, posterior infragluteal-parabiceps approach. Traditional proximal posterior approaches to sciatic nerve block described in preceding text require needle placement deep to the gluteus maximus. This approach may be difficult and painful, especially in obese patients if multiple needle redirections are required. Additionally, the sciatic nerve at the level of the gluteal approaches is in close proximity to the inferior gluteal artery, thereby increasing the potential risk of vascular puncture and/or intravascular injection. A newer proximal posterior approach to sciatic nerve block relies on two easily identifiable landmarks (2): the lateral border of the biceps femoris muscle tendon and the inferior border of the gluteus maximus (gluteal crease). At this location, the sciatic nerve is just lateral to the lateral border of the tendon (Figure 16.3). The infragluteal-parabiceps technique has several advantages, which include a relatively shallow depth (as compared to the traditional approach of Labat), the absence of any muscles or major vascular structures (which should decrease the potential for patient discomfort and intravascular injection of local anesthetic). The technique described in the subsequent text relies on peripheral nerve stimulation, although USG techniques may also be used.
1. Patient position. The patient is placed in the lateral decubitus position with a slight forward tilt, hips flexed with the operative side to be blocked uppermost. The dependent limb should be straight and the operative limb should be flexed slightly at both the hip and knee. Alternatively, the patient may also be placed prone to enhance the visibility of the gluteal crease.
2. External landmarks. The gluteal crease is identified and marked with a line. The lateral border of the biceps femoris muscle tendon is identified. A helpful approach to identify the biceps femoris muscle tendon is to first locate its tendinous insertion at the IT. The course of the tendon is palpated as it descends in the posterior thigh. The proposed needle insertion point is 1 cm below the gluteal crease along the lateral border of the biceps femoris muscle tendon.
3. After aseptic skin preparation and draping followed by local anesthetic infiltration of the proposed needle insertion point, a stimulating needle (typically a 50–100 mm [2–4 in.], 21–22 gauge) is inserted just lateral to the biceps femoris muscle tendon with an angle of 70 to 90 degrees to the skin and advanced in a cephalad manner. The stimulating needle is attached to a PNS (typical settings of 1.5–2.0 mA, 2 Hz, 100 μs) and a syringe of local anesthetic.
4. As the stimulating needle is advanced, the needle tip passes through skin and subcutaneous tissue until the desired EMR is elicited. Contraction of the biceps femoris muscle is not accepted as this indicates either direct muscle stimulation or stimulation of the motor branch. If this occurs, the needle is advanced slightly deeper. The desired EMR is inversion or plantar flexion of the foot (see subsequent text). If plantar flexion is elicited, the needle tip is redirected just lateral to obtain inversion. Alternatively, if the dorsiflexion is obtained, the needle tip should be slightly adjusted medial to elicit inversion. The final position of the needle tip is considered optimal when the desired EMR is still elicited at 0.2 to 0.5 mA.
5. After the final needle position is obtained and an initial 3-mL test dose to confirm the absence of intravascular location of the local anesthetic injection, a total of 25 to 35 mL of local anesthetic is incrementally injected with frequent intermittent aspirations to reduce the risk of intravascular injection. Typical onset time for sensory anesthesia is 15 to 25 minutes depending on the total mass of local anesthetic injected and the EMR elicited.
6. A continuous catheter technique may be utilized to provide extended duration analgesia. The initial needle insertion site and approach are the same as the single-injection technique. A larger bore (17- to 18-gauge) insulated stimulating Tuohy needle is typically used to localize the sciatic nerve. After localization of the sciatic nerve and injection of the local anesthetic, the needle angle is decreased and the needle tip is oriented toward the midpoint of the GT and IT to facilitate catheter passage along the course of the sciatic nerve. A 19- to 20-gauge catheter is inserted through the Tuohy needle and advanced no more than 3 to 5 cm past needle tip. The needle is then withdrawn over the catheter and the latter fixed in place with a sterile clear adhesive dressing. The proximal end of the catheter is then connected to an automated infusion pump.
7. Clinical pearls. Asking the patient to “bend the leg” (flexion at the knee) results in contraction of the hamstring muscles, which helps to accentuate the location of the lateral border of the biceps femoris muscle tendon. Understanding the anatomy of the sciatic nerve is key to interpreting EMR when using a PNS technique (Figure 16.6).
a. Plantar flexion corresponds to stimulation of the TN.
b. Dorsiflexion corresponds to stimulation of the CPN.
c. Eversion corresponds to stimulation of superficial branch of the CPN, located on the lateral aspect of the CPN.
d. Inversion corresponds to stimulation of the TN (contraction of the tibialis posterior muscle) and the deep branch of the CPN (contraction of the tibialis posterior muscle). Therefore, inversion indicates that the needle tip is central in location to the sciatic nerve with simultaneous stimulation of both the TN and the deep branch of the CPN. Additionally, intraneuronal topography of the TN demonstrates that the nerve bundles innervating the tibialis posterior muscle are located within the lateral aspect of the TN (16). Therefore inversion indicates that the needle is near the lateral portion of the portion of the TN, which lies in close proximity to the CPN.
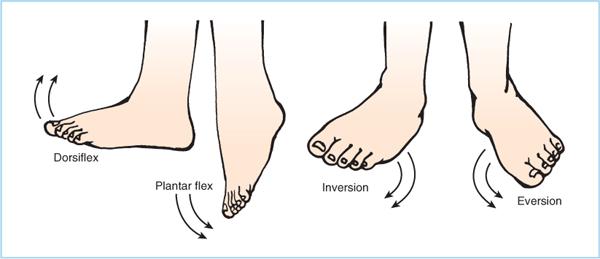
Figure 16.6. Foot movements with sciatic stimulation.







Full access? Get Clinical Tree


