Ultrasound image of interscalene brachial plexus visualized between the anterior and middle scalene muscles.
In the out-of-plane method the needle tip is not visualized; therefore, localizing the needle is dependent on tissue displacement and/or hydrolocation, in which fluid is injected in small increments to determine needle tip location prior to advancement of the needle [7].
Continuous interscalene block (CISB)
The approach to the brachial plexus for a CISB is identical to that of an ISB. A Tuohy needle is advanced to a point in proximity of the C5–C6 root or the upper trunk and the catheter is then advanced into the target tissue plane. As with ISB, both in-plane and out-of-plane techniques are possible. The in plane-method provides the advantage of visualization of the needle tip location, whereas the out-of-plane method may facilitate placement and advancement of the catheter along the long axis of the brachial plexus. For the in-plane method, a potential disadvantage for catheter placement is that the catheter tip may potentially bypass the nerve medially, given the perpendicular orientation between the needle and the nerve [8]. In the out-of-plane method, the orientation of the Tuohy needle parallel to the long axis of the nerve fibers may theoretically decrease the incidence of intraneural placement [3]. Regardless of the approach the catheter should be secured no further than 3 to 5 cm past the tip of the Touhy needle.
Local anesthetic, saline, or dextrose 5% may be administered through the Tuohy needle to open the tissue plane and facilitate catheter placement in proximity to the brachial plexus. The advantage of using dextrose is that evoked motor response is maintained following injection [9] and, if a stimulating catheter is used, catheter location can be assessed with evoked motor potentials. With any US-guided method, a bolus of local anesthetic may be administered via the catheter and spread adjacent to the nerve, directly visualized.
The catheter is then secured and connected to a pump that delivers local anesthetic continuously and/or via patient-controlled bolus.
Pharmacology
Pharmacology of single-shot interscalene block
Although Winnie recommended a local anesthetic volume of 40 ml [4], US guidance has significantly reduced the volume of local anesthetic needed for successful interscalene block [10]. Successful interscalene blocks using ropivacaine 0.75% have been reported with a minimum volume of 5 ml; notably, block duration was not decreased with lower volumes [11]. Lower volumes of local anesthetics decrease the risk of systemic toxicity, and decrease spread of local anesthetic toward the neuraxis and phrenic nerve [12]. Such low volumes of local anesthetic may not, however, yield adequate motor relaxation or consistency with regard to block onset and duration [11].
Pharmacology of continuous interscalene block
Much variability exists regarding dosing of CISBs. Early studies reported high volume and dosages [13]. Infusions using lower concentrations of local anesthetic (0.2% vs. 0.4%) and higher infusion rates (8 ml/h vs. 4 ml/h) provide superior analgesia [14]. In particular, both a continuous infusion [15] with a bolus dose seems to provide superior analgesia compared with continuous infusions or bolus doses alone [16]. A continuous infusion of ≥4 ml/h is suggested in addition to a bolus dose of ≥4 ml/h for adequate analgesia [3, 16]. Although further study is required, the use of an automated bolus technique has demonstrated superior analgesia compared with a continuous infusion rate [16].
3. Contrast the benefits of an interscalene catheter vs. a single-injection block
ISB provides benefits in the immediate postoperative period, including decreased VAS pain scores, decreased need for analgesic medications, decreased nausea/vomiting, and bypassing of phase 1 PACU [5]. However, the maximum duration of action of an ISB is generally less than 24 hours – yet pain, following shoulder surgery is often severe and persists up until postoperative day (POD) 3 [17].
In the immediate postoperative period (POD 0), single-injection and continuous interscalene catheters are equally beneficial and superior to general anesthesia. However, when the postoperative time is extended to include POD 1 to 3, patients receiving continuous catheters have a longer time to first pain report, lower mean pain scores, less opiate requirements, and report longer hours of sleep as compared to patients receiving ISB or general anesthesia alone. During POD 1 to 3, patients receiving GA vs. ISB have equivalent pain scores and require similar oral analgesics [18]. Consequently, the benefits of ISB appear to be limited to the duration of the block [5].
Perineural catheters prolong the duration of action and analgesic benefit of local anesthetics. However, catheters have drawbacks, including difficulty of placement, the potential for bacterial colonization and/or infection [19–20], and displacement from the optimal location [21].
4. Review alternative regional techniques if the patient had significant pulmonary disease
Complications of interscalene block include transient Horner’s syndrome, recurrent laryngeal nerve palsy, intravascular injection, spinal or epidural anesthesia, pneumothorax, and nerve damage [22]. Interscalene blocks also result in hemidiaphragmatic paralysis, either by direct blockade of the phrenic nerve or due to cephalad spread of local anesthetic reaching the C3–C5 nerve roots [23]. Decreased rates of hemidiaphragmatic paralysis have been reported using lower volumes of local anesthetics with an incidence of 33% (5 ml) and 60% (10 ml) [24]. However, as it is difficult to anticipate which patients will not experience phrenic nerve blockade; caution remains warranted. Consequently, these blocks are contraindicated in patients who have contralateral phrenic nerve or recurrent laryngeal nerve palsies, contralateral pneumonectomy, and patients who have a forced vital capacity of less than one liter [23]. Since general anesthesia is also undesirable and postoperative analgesia still needed, alternative regional anesthesia techniques have evolved.
The suprascapular and axillary nerves are the major terminal nerves supplying the shoulder joint. Therefore performing a blockade of both nerves provides analgesia after shoulder surgery while avoiding the risk of hemidiaphragmatic paralysis.
5. Discuss methods for placement of suprascapular and axillary nerve blocks
Suprascapular nerve block
Nerve stimulation: The most common approach utilizing nerve stimulation alone is the Meier method. In this method, the suprascapular nerve is blocked as it passes from the suprascapular notch to the spinoglenoid notch within the lateral supraspinous groove [2]. The spine of the scapula is identified and marked from the lateral part of the acromion to the medial aspect of the scapular spine. The injection site will be 2 cm cranial and 2 cm medial to the midpoint of the scapular spine (Figure 30.2) [25]. After observing stimulation of the infraspinatus muscle, causing external rotation of the shoulder, 15 ml of local anesthetic is injected. It must be noted that this method carries a slight risk of pneumothorax [2, 25].
Ultrasound guidance: The patient is seated upright and the US probe is placed parallel and superior to the scapular spine. The probe is then moved laterally and the suprascapular notch identified. The suprascapular nerve is a hyperechoic structure located deep to the trapezius and the supraspinatus muscles under the transverse scapular ligament within the suprascapular notch (Figure 30.3) [26]. The evoked motor response is abduction of the shoulder. The optimal volume of local anesthetic required to block the nerve when using US guidance has been suggested to be 5 ml [27], and as little as 10 ml may result in spread to the brachial plexus [28].

The Meier method for the performance of the suprascapular nerve block.
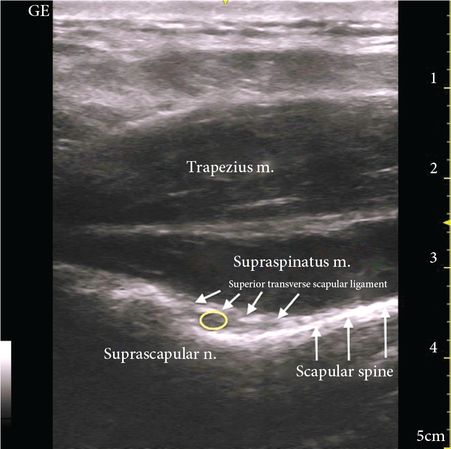
Ultrasound imaging for a suprascapular nerve block. The suprascapular nerve is visualized under the superior transverse scapular ligament deep to the trapezius and supraspinatus muscles.
Related posts:



Full access? Get Clinical Tree


