Fig. 31.1
The da Vinci® Si Surgical System. (Used with permission. Copyright © 2015 Intuitive Surgical Inc.)
The latest version, the da Vinci Xi Surgical System, was released for the US market in early 2014. This system is designed to facilitate the process of surgical access with a newly designed, more flexible robotic arm configuration (Fig. 31.2). The Xi surgical cart can thus access all four surgical quadrants from a single position, which greatly simplifies setup. The arms of the Xi system are also thinner and provide a greater range of motion when compared to the previous models. This novel arm design in combination with instruments of longer reach offers a more flexible port placement. The surgical cart hosts a number of new features including a guided setup process with voice assistance to facilitate a quick and precise setup. A laser targeting system is used to help arrange the surgical cart and the robotic arms in an optimal configuration around the targeted anatomy [6].
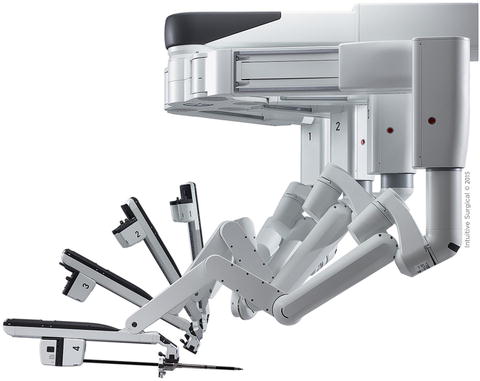
Fig. 31.2
Robotics arms of the da Vinci® Xi System with improved flexibility. (Used with permission. Copyright © 2015 Intuitive Surgical Inc.)
While the technology of the da Vinci Surgical Systems has been progressively updated, all systems remain are very similar in their basic components and contain a surgeon’s console, a surgical cart, and a vision cart. They share the following core features as major differences to conventional laparoscopy:
All systems are designed in a master-slave configuration with physical separation of the surgeon and the patient.
Vision system with a true 3-dimensional image with up to ten times magnification streamed into the stereo viewer of the surgical console resulting in a panoramic view of the surgical field (Fig. 31.3).

Fig. 31.3
The da Vinci® stereo viewer. (Used with permission. Copyright © 2015 Intuitive Surgical Inc.)
Wristed instruments (Fig. 31.4) with seven degrees of freedom and intuitive control (Fig. 31.5) due to the humanoid design of the robotic anatomy (robotic arm and instruments mimic the human upper extremity—movements of surgeon’s hands are followed by surgical instruments).

Fig. 31.4
da Vinci® wristed instruments. (Used with permission. Copyright © 2015 Intuitive Surgical Inc.)
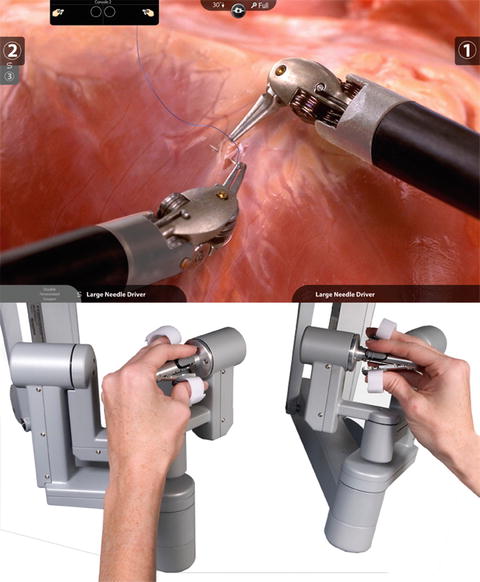
Fig. 31.5
Intuitive control of robotic instruments achieved by humanoid design of the da Vinci® Surgical System and hand-eye alignment. (Used with permission. Copyright © 2015 Intuitive Surgical Inc.)
All systems are equipped with distinct software feature including motion scaling and tremor filtration.
Considering the above descriptions of the da Vinci Surgical System, it seems apparent that this robotic system offers distinct technical advantages when compared to conventional laparoscopy. Since its first clinical application for a cholecystectomy in 1997 and its market launch in 1999, the system has been used for an increasing amount of surgical procedures including operations from many fields of surgery [7–9]. With growing clinical experience, it soon became evident that the da Vinci could enable advanced surgical procedures to be performed in a minimally invasive fashion [10]. Perioperative parameters are usually improved for almost all surgical procedures when performed via minimally invasive surgery versus an open approach. Although an initial goal of the da Vinci was to perform complex cardiac surgeries, a group of German surgeons found particular value in the system when working in the tight confines of the male pelvis and developed a robotic approach to radical prostatectomy [11]. This insight led to a growing adoption of the da Vinci for this challenging procedure. At the time of this publication, the value of robotic technology for radical prostatectomy has been clearly established by numerous high-level-of-evidence manuscripts, including prospectively randomized trials and meta-analyses. It is the recommended surgical method for this procedure by several clinical guidelines as well as Health Technology Assessments [12].
In continuous pursuit of improving techniques and reduced invasiveness, abdominal surgeons also developed interest in this technology. Reports can be found in the literature of many robotic digestive surgical procedures that have been performed successfully including benign and malignant foregut surgery, colorectal surgery, bariatric surgery, endocrine surgery, hepato-biliary-pancreatic surgery as well as many others.
Clinical Applications of Robotics in General Surgery
Upper Gastrointestinal Tract
Early reports of robotic anti-reflux surgery can be found in the literature of the performance of fundoplication. While many reports demonstrate the general feasibility of the robotic approach for this procedure, no clear clinical advantages over a laparoscopic approach can be derived from the current literature. However, several studies suggest it entails increased operative time and costs of surgery [13, 14].
A similar conclusion can be arrived at for the procedure of robotic Heller myotomy. While some publications suggest a lower rate of perforations with the robotic application, the overall data indicate general feasibility of a robotic approach to Heller myotomy with no clear clinical advantage over laparoscopic technique [15–17].
While many procedures of the field of bariatric surgery are most commonly performed with conventional laparoscopy, several distinct anatomical challenges often exist, including a thick abdominal wall, hepatomegaly, and increased amounts of intra-abdominal fat. These constraints produce a limited workspace, which results in reduced surgical dexterity and impaired ergonomics during conventional laparoscopy. Several publications from other fields of surgery indicate that robotics may facilitate surgery in the obese population [18, 19] and the number of clinical reports of robotic applications for a variety of bariatric procedures is growing.
At this point, the largest body of clinical evidence on robotic use for bariatric indications can be found for Roux-en-Y gastric bypass (RYGB) with early reports beginning in 2003. Since that time, multiple groups have published their clinical outcomes with a variety of surgical methods including hybrid and total robotic approaches to RYGB. While some of the early articles reported challenges of the robotic technology, mainly around the absence of force feedback leading to bowel injuries [20], more recent comparative studies [21–23] as well as systematic reviews [24, 25] do offer some evidence supporting the clinical advantages of robotic RYGB surgery including low rates of anastomotic strictures and leaks. These potential clinical advantages of robotic technique can be explained by the different techniques usually used for the creation of a laparoscopic gastrojejunal anastomosis. While the technical challenges of creating a sutured anastomosis laparoscopically caused a shift towards stapled technique during conventional laparoscopy, the robotic technology enables a return to the hand-sutured style of gastrojejunal anastomosis (Fig. 31.6) which is believed to be superior when compared to stapling. In support of this theory, several comparative studies have shown a lower leak and stricture rate of the gastrojejunal anastomosis when using a robotically sutured technique compared to laparoscopic stapling [21, 23]. A meta-analysis further recognized an advantage regarding postoperative strictures after robotic RYGB when compared to the laparoscopic technique [25].
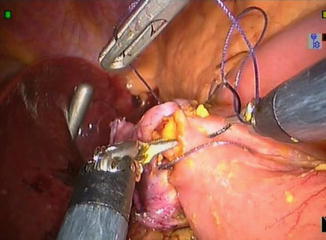
Fig. 31.6
da Vinci® (Intuitive Surgical Inc; Sunnyvale, CA) sutured gastrojejunal anastomosis
While the clinical data of RYGB show some clear indications in regard to the clinical value of the robotic technology, the value of a robotic approach to sleeve gastrectomy (SG) seems less clear. Although the robotic approach may facilitate the mobilization of the stomach and enable suturing of the previously stapled tissue, the most critical element of this procedure is currently still most commonly performed using laparoscopic staplers. Robotic staplers have just recently been released in the United States only, and exclusively for the da Vinci Si System. Further experience with the robotic staplers will show whether this procedure might gain significance as a robotic approach. To date, literature on robotic SG indicates general feasibility and safety with longer operative times [26, 27]. One research group analyzed their series of robotic assisted SGs and compared data to a systematic review of laparoscopic sleeve gastrectomies (LSG): Lower leak and stricture rates were found with the robotic approach to SG [28].
The first robotic bariatric procedure performed was a robotic placement of an adjustable gastric band (AGB) by Cadiere and Himpens in 1998 [29]. Subsequently, other authors have reported on the feasibility and safety of performing robotic AGB placement [30, 31]. Although it seems apparent that robotic technology can provide advantages during some parts of the dissection and suturing the anterior gastric plication, the lack of tactile feedback may be a disadvantage during the “blind” preparation of the posterior gastric tunnel. In addition, AGB is a surgical procedure of low complexity and few perioperative complications occur when it is performed laparoscopically. Therefore, the incremental clinical value of robotics to this procedure might be limited considering the added cost.
Besides these common bariatric procedures, robotics has also been applied to some more advanced procedures including biliopancreatic diversion with duodenal switch (BPD/DS) and revisional surgery (RS) [32]. While both procedures are of advanced complexity and therefore have the potential to benefit significantly from the technical advantages of a robotic approach, a very limited number of reports of its application can be found in the literature. Due to its limited application and the extensive need for multi-quadrant access (from stomach to ileocecal valve), BPD/DS will most likely not develop into a dominating robotic indication. The new da Vinci Xi system is designed for four-quadrant access and may demonstrate increased suitability for this procedure in the future. Revisional surgery is currently significantly increasing in terms of case numbers and the complex nature of these procedures makes it ideal for the robotic approach. It is expected that the body of evidence in regard to robotic RS will increase over the next few years and shed more light on the value of robotics for this bariatric procedure.
Several reports can be found in the robotic application for early gastric cancer with similar indications as for a laparoscopic approach. Overall data suggest that robotic surgery for gastric cancer is safe, feasible, and results in similar perioperative outcomes when compared to conventional laparoscopy [33–35]. In addition, it has been suggested that the technical specifications of the robotic technology enable a minimally invasive approach to D-2 lymphadenectomy [35]. This procedure has been established as the gold standard of treatment, with improved long-term oncological outcomes for the patients when compared to a limited D-1 lymphadenectomy [36]. More systematic data is needed to verify this potentially very meaningful advantage of robotics over conventional laparoscopy.
Colorectal Surgery
Besides evidence of general feasibility, the role of robotics in colon surgery remains undetermined at this point: While the technical advantages of robotics could play a role during more complex maneuvers including extended lymphadenectomy (D3 for right colectomy) and the formation of intra-corporeal anastomoses, more substantial clinical evidence is needed to verify clinical advantages of robotic technology for colon surgery.
A greater body of evidence can be found for the application of robotics in rectal surgery, particularly regarding the treatment of rectal cancer (Fig. 31.7). While conventional laparoscopy can be safe and effective for the resection of rectal cancer by experienced hands, relatively high rates of conversions and circumferential margin positivity have been demonstrated by systematic research [37–39]. Therefore, the laparoscopic approach has not yet been established as the gold standard approach for patients with rectal cancer [40, 41]. The technical superiority of robotics holds the promise to overcome the limitations of conventional laparoscopy in this setting and may result in fewer conversions and reduced rates of positive margins when compared to conventional laparoscopy [10]. While most of the studies of this sort which have been performed to date are of limited quality and therefore prone to bias, more systematic research of the field of robotics for rectal cancer is currently under way and first results are expected soon.
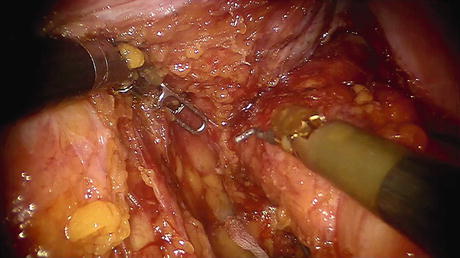
Fig. 31.7
da Vinci® (Intuitive Surgical Inc; Sunnyvale, CA) low anterior resection
An emerging and highly interesting novel procedure is a robotic application in transanal resection of low-risk rectal cancers and benign conditions (Fig. 31.8). Several research groups have published their laboratory experience as well as initial clinical experience of transanal robotic surgery for local excisions and retrograde total mesorectal excision [42, 43].

Fig. 31.8
da Vinci® (Intuitive Surgical Inc; Sunnyvale, CA) transanal surgery
A number of reports from the field of robotic hepatobiliary surgery can be found. Robotic pancreatic resections have been performed for a variety of procedures including distal, central, and total pancreatectomy as well as for pancreaticoduodenectomy [44, 45]. Current literature suggests the feasibility of robotic pancreatic resection with potential advantages over open and laparoscopic surgery in terms of short-term outcomes. However, quality of these studies is limited and more systematic research is needed to verify these positive early findings. Similarly, robotic liver resections have been reported to be safe and feasible in experienced hands [46, 47]. While robotic technology seems to have advantages that facilitate a variety of surgical maneuvers that are needed during liver resection, more advanced robotic instrumentation will be needed to enable widespread application.
Single-Site Surgery
While some groups reported their early experience with robotic surgery through a single incision using the conventional da Vinci instruments in unconventional arrangements [48], a dedicated set of semi-rigid instruments and curved cannulae for robotic single-site surgery was released in 2011 [49]. This platform was predominantly used for cholecystectomy (Fig. 31.9). Literature shows the general safety and feasibility of the technique with potentially shorter OR times and facilitated learning curves when compared to conventional single-incision laparoscopy [50, 51]. Several reports can be found on the application of robotic single-site surgery for other procedures [52].
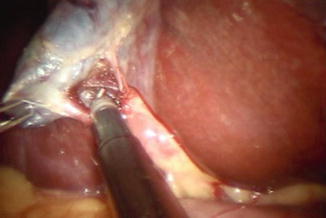
Fig. 31.9
da Vinci® (Intuitive Surgical Inc; Sunnyvale, CA) Single-Site cholecystectomy
Fluorescence Imaging
Recently, an intraoperative near infrared fluorescence imaging system has been developed for the use with the da Vinci Si system. The technology has been used during a variety of surgical procedures to visualize blood flow (Fig. 31.10), lymph node mapping, intraoperative cholangiography and to identify anatomy of the surgical field [53–55]. Systematic research will be needed to determine the impact of this technology on clinical outcomes.
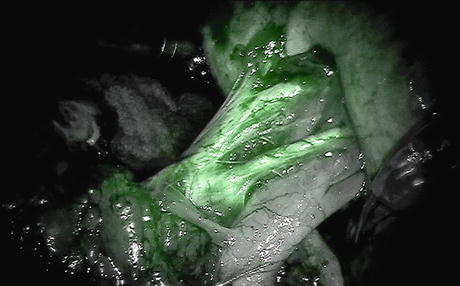
Fig. 31.10
da Vinci® (Intuitive Surgical Inc; Sunnyvale, CA) fluorescence imaging of renal hilum
Limitations of Current Robotic Systems for General Surgery
Despite the clear technological advance represented by surgical robotics and potential it holds to overcome several limitations of conventional laparoscopy, the use of robotic systems in the present day does not come without controversy: There is abundant data to suggest that robotics are safe and feasible for many procedures in General Surgery, but overall clinical outcomes are often not superior when compared to conventional laparoscopy and/or open surgery. While some studies suggest clinical advantages in certain applications, the clear value of robotics and its role in General Surgery remains undefined. Robotics entails increased costs due to capital investment, system maintenance, and reposable instruments, so it must prove it can deliver short- and long-term patient benefits by providing unique solutions to otherwise unobtainable clinical demands in order to be cost effective. Unfortunately, current published studies on this topic are low-level-of-evidence and are therefore prone to bias. Various prospectively randomized trials from different fields of General Surgery are currently underway to answer some of these important questions that stand in the way of robotics becoming the gold standard for numerous procedures of the field of General Surgery.
Related posts:
 End Points of Resuscitation
End Points of Resuscitation
 Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
 The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
 New Minimally Invasive Treatments for Acid Reflux
New Minimally Invasive Treatments for Acid Reflux
 Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
 Brain Cancer: The New Frontiers
Brain Cancer: The New Frontiers

Full access? Get Clinical Tree


