Key Clinical Questions
What are the signs and symptoms of cervical spine involvement in rheumatoid arthritis and the spondyloarthropathies?
What tests should be ordered in patients with suspected pulmonary-renal syndrome?
Which patients with interstitial lung disease are most likely to respond to corticosteroids?
What are common and uncommon clinical signs and symptoms associated with giant cell arteritis?
What factors portend an impending renal crisis in a patient with known scleroderma?
What are the risk factors for Raynaud digital crisis? What treatments reduce morbidity?
Introduction
Rheumatologic disease rarely presents with acute emergencies, but when it does it may reflect rapidly progressive disease or a delay in diagnosis that leads to significant morbidity and mortality. The most important and common examples of this include recognition of the protean presentations of giant cell arteritis so as to avoid and prevent permanent visual loss and to recognize the clinical pattern of the pulmonary renal syndrome which if not recognized can lead to acute respiratory failure and renal failure requiring dialysis.
The Cervical Spine in the Rheumatic Diseases
Catastrophic neurologic injury and even death may result from cervical spine disease in patients with rheumatoid arthritis (RA) or spondyloarthropathy. Early recognition of the signs and symptoms and appropriate diagnostic evaluation are critical to avoid these complications.
Up to 30% of patients with severe RA have some degree of subluxation of the atlantoaxial joint (C1-C2). In normal patients, the odontoid process of the axis (C2) is secured in front by the anterior arch of the atlas (C1) and posteriorly by the transverse ligament of the atlas. The normal distance between the odontoid process and the anterior arch of the atlas is 3 mm. Inflammation in the small joints that make up the atlantoaxial joint, or tenosynovitis of the transverse ligament of the axis, may weaken the transverse ligament, as well as lead to bony erosions in the odontoid process. As a result, the space between the odontoid and the anterior arch of the atlas widens (Figure 254-1), and the atlantoaxial joint becomes unstable. Most commonly, anterior subluxation, when the atlas slides forward relative to the axis, leads to cord compression and cervical myelopathy. Less commonly, posterior subluxation occurs when the odontoid is badly damaged or fractured. Rarely, vertical subluxation occurs, with C1-C2 impaction, migration of the odontoid into the foramen magnum, brainstem compression, and death. Atlantoaxial instability may also produce vertebrobasilar insufficiency by impairing blood flow in the vertebral arteries, which travel through the transverse foramina of the cervical spine.
Figure 254-1
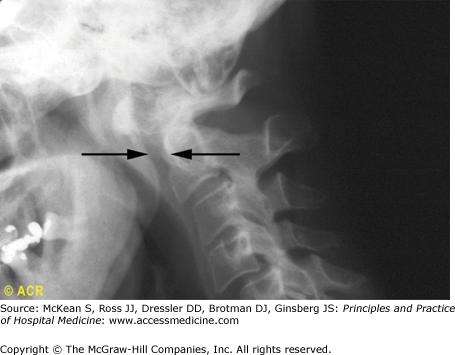
Cervical spine in rheumatoid arthritis, showing atlantoaxial subluxation. A lateral view of the upper cervical region shows posterior displacement of the odontoid process. The preodontoid space measures approximately 8 mm (arrows). Normally this measurement should not exceed 2.5 to 3 mm in an adult, although in a child 4 to 5 mm may be within the normal range. The measurement is made at the base of the anterior aspect of the dens with the neck held in flexion. There is also anterior displacement of C4 on C5. Associated disc-space narrowing and erosion are not present. Atlantoaxial subluxation also occurs in ankylosing spondylitis. (Reproduced from the American College of Rheumatology Image Bank. © 2009 American College of Rheumatology, used with permission.)
Physical signs may include occipital or retroorbital headache, tingling in the fingers, and electric shocks in the upper extremities with neck flexion. Physical findings include hyperreflexia, a positive Babinski test, and sensory loss in the hands and feet. Unfortunately, the neurologic examination may be confounded by muscle wasting, severe joint deformities, and entrapment neuropathies, all of which are very common in RA. Ominous symptoms and signs include a sensation of the head falling forward during neck flexion, syncope, respiratory irregularities, loss of sphincter control, dysphagia, hemiplegia, or nystagmus.
Lateral radiographs of the cervical spine in flexion are the most useful initial diagnostic studies. These are diagnostic if the space between the anterior arch of the atlas and the odontoid is 9 mm or more, with an interval between the odontoid and the posterior arch of the atlas of less than 14 mm in the flexed position. In symptomatic patients, flexion films should only be performed if standard films have excluded odontoid fracture and severe subluxation. When cervical spine radiographs are not diagnostic, magnetic resonance imaging (MRI) with neck flexion and extension should be performed. MRI is especially useful in delineating the extent of cord compression, the relationship of the odontoid to the brainstem, and in planning surgical stabilization. However, compared with plain radiographs, it may underestimate the degree of subluxation.
In the setting of progressive symptoms of cord compression, urgent neurosurgical consultation should be obtained for stabilization of the cervical spine. The role and timing of surgery in patients with atlantoaxial instability without cord compression is uncertain. The utility of medical therapy, such as rigid cervical collars and isometric neck strengthening exercises, is also unclear.
In patients with RA undergoing general anesthesia, cervical spine lateral radiographs with flexion and extension views should be obtained to exclude significant subluxation. Preoperative anesthesia consultation is mandatory in the RA patient with cervical instability. Fiberoptic intubation should be considered to limit neck manipulation.
Neurologic disease is common in the spondyloarthropathies, particularly in ankylosing spondylitis. In longstanding disease, the spine is rigid, fused, osteoporotic, and brittle. Spinal fracture may occur with mild trauma, or even spontaneously. The most dreaded outcome is an acute cervical fracture, generally presenting as acute neck pain with or without neurologic compromise. Cord compression with quadriplegia may ensue unless the spine is promptly stabilized. Neurosurgical involvement is requisite. Ankylosing spondylitis may also be complicated by atlantoaxial subluxation, as in RA. Arachnoiditis may lead to scarring of sacral and lumbar nerve roots and cauda equina syndrome, with saddle anesthesia, paraparesis, and bowel and bladder disturbances.
Airway Involvement in the Rheumatic Diseases
Airway involvement is a rare but significant source of morbidity and mortality in the rheumatic diseases. In Wegener granulomatosis (WG), a systemic vasculitis characterized by upper and lower respiratory granulomatous inflammation and glomerulonephritis, inflammation may occur in the subglottis and proximal trachea. Tracheobronchial WG often does not respond to systemic therapy and may run a course independent of the other manifestations of WG, leading to recurrent infections or ventilatory obstruction. Tracheobronchial involvement should be suspected when a patient with known WG presents with sore throat, cough, and difficulty with secretions. Chest radiography and spirometry are helpful initial tests, which may be confirmed with laryngoscopy or computed tomography scan. When this complication is suspected, otolaryngologic consultation is mandated. Treatment involves intralesional steroid injection and dilatation of obstructive lesions. When severe, stenting and tracheostomy may be necessary.
Relapsing polychondritis is characterized by episodes of inflammation of the cartilaginous structures of the outer ear, nose, larynx, and tracheobronchial tree. Tracheobronchomalacia may result from the loss of the supporting cartilage of the upper airway, resulting in either fixed airway obstruction or hyperdynamic collapse. Concerning symptoms include progressive dyspnea, stridor, hoarseness, sore throat, and chest discomfort. The flow-volume loop is a useful screening test. It may reveal extrathoracic obstruction, intrathoracic obstruction, or both. This may be confirmed with bronchoscopy or dynamic CT scanning. Treatment options include stenting, balloon dilatation, or tracheostomy.
Pulmonary-Renal Syndromes
Patients may present to hospital with both pulmonary infiltrates and renal insufficiency, and no obvious cardiac or infectious cause. This should raise consideration of several diseases leading to pulmonary-renal syndromes, especially when these patients have proteinuria or active urinary sediments consistent with nephritis. Pulmonary-renal syndromes may be immune complex related, as in systemic lupus erythematosus (SLE) and cryoglobulinemia, or mediated by direct antibody binding, as in antiglomerular basement membrane (anti-GBM) disease, also known as Goodpasture syndrome. It may also be pauci-immune, characterized on biopsies by a relative lack of immunoglobulin and complement. These include the vasculitides associated with antineutrophilic cytoplasmic antibodies (ANCA), such as Granulomatosis with Polyangiitis (Wegener granulomatosis), microscopic polyangiitis (MP), and Churg-Strauss syndrome (CSS). Clinical clues may suggest a specific diagnosis, such as the arthritis, pleurisy, and photosensitivity of SLE; upper respiratory symptoms, such as sinusitis or otitis, suggestive of WG; or mononeuritis multiplex often seen in the ANCA-associated vasculitides.
Laboratory evaluation in this setting should include ANCA, antinuclear antibody (ANA), anti-GBM antibody, and cryoglobulin. Biopsy should be considered. In the face of undifferentiated disease and clinical deterioration, empiric therapy including high-dose corticosteroids and even cyclophosphamide or rituximab may be necessary, pending the results of testing or biopsy.
Interstitial Lung Disease
Interstitial lung disease is an uncommon but feared complication in a variety of rheumatic diseases including scleroderma, dermatomyositis/polymyositis (DM/PM), rheumatoid arthritis, SLE, and mixed connective tissue diseases. It affects up to 50% of patients with scleroderma, 30% of patients with DM/PM, and 10% of patients with RA. While parenchymal lung disease is often insidious, in some cases it may be explosive and necessitate hospitalization. Patients may present with progressive dyspnea, dry cough, and desaturation with exercise oximetry.
High-resolution chest CT is very useful in characterizing interstitial lung disease. It may reveal ground glass opacities, seen in many conditions including acute interstitial pneumonia, nonspecific interstitial pneumonia, desquamative interstitial pneumonia, Pneumocystic pneumonia (PCP), viral pneumonia, pulmonary edema and acute respiratory distress syndrome. Honeycombing and traction bronchiectasis are seen in fibrotic lung disease and usual interstitial pneumonia and consolidative inflammatory lung disease is seen in cryptogenic organizing pneumonia. However, there is much overlap in the radiographic appearance of different forms of interstitial lung disease. Lung biopsy may be diagnostic, although the potential utility of a pathologic diagnosis must be balanced against the hazards of lung biopsy in patients with tenuous respiratory status.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


