Key Clinical Questions
Does this patient have rheumatoid arthritis or another inflammatory arthritis?
What are the extra-articular manifestations of rheumatoid disease?
Is one responsible for this patient’s hospitalization?
Is this hospitalization due to medication toxicity?
How should the patient’s disease-modifying antirheumatic drugs be managed during the hospitalization, including perioperatively?
What tests and studies are useful to evaluate this patient’s presentation?
What treatments are available?
Introduction/Epidemiology
Rheumatoid arthritis (RA) affects 1% of the population worldwide, with women being more commonly affected. In the recent past, there were only a few disease-modifying antirheumatic drugs (DMARDs), which were not prescribed until after joint damage had occurred. Patients were frequently admitted to the hospital for arthritis treatment, including administration of ACTH, rest, and intra-articular corticosteroid injections. Today, early, aggressive DMARD therapy, including biologic DMARDs, has dramatically improved patient outcomes. Most patients with RA are treated exclusively as outpatients, and are never hospitalized due to the disease itself. However, RA is a systemic disease with numerous potential extra-articular manifestations, including cardiovascular disease. A hospitalist must be alert to these manifestations, as they may lead to hospitalization.
|
Most other common inflammatory arthritides fall into the category of seronegative spondyloarthropathies, which affect up to 2% of individuals, with an equal male to female ratio. They include psoriatic arthritis (PsA) (population prevalence 0.3–1.0%), ankylosing spondylitis (AS) (prevalence 0.1–6.0%, depending on the population studied), inflammatory bowel disease–associated arthritis, reactive arthritis, and undifferentiated spondyloarthropathy. These illnesses are seronegative for rheumatoid factor, and are associated with the presence of human leukocyte antigen (HLA)-B27. The presence of HLA-B27 varies by ancestry. In general, up to 15% of the population is HLA-B27 positive. However, among individuals with spondyloarthropathies, up to 90% are HLA-B27 positive. Spondyloarthritis is characterized by axial arthritis with a predilection for the sacroiliac joints, oligoarthritis, especially of the lower extremities, and enthesitis, or inflammation of ligaments and tendons at attachments to bone. Inflammatory arthritis may be just one manifestation of a systemic disease that may include psoriasis and psoriasiform skin lesions, genital inflammation, inflammatory bowel disease, and inflammatory eye disease, such as uveitis or scleritis.
This chapter reviews articular and extra-articular manifestations of RA and the spondyloarthropathies. We will also review the indications, mechanisms, and most frequent complications of the DMARDs used to treat RA and other inflammatory arthritides, with recommendations for management of DMARD therapy in hospitalized patients with other illness, as well as during the perioperative period.
Pathophysiology
|
Rheumatoid arthritis is thought to result when an environmental factor stimulates an aberrant immune response in a genetically susceptible host. Several genes are associated with susceptibility to development of RA. Most significantly, RA is associated with HLA-DRB1. A short amino acid sequence within this gene, known as the “shared epitope,” is associated with increased risk of severe RA and development of anti-citrullinated peptide antibodies. Within proteins, the amino acid arginine can undergo posttranslational modification, mediated by peptidylarginine deaminases, into citrulline. Autoantibodies against citrullinated peptides appear to be quite specific for rheumatoid arthritis. Identification of these autoantibodies is now part of routine diagnostic testing for RA via the anti-CCP antibody test. An immune reaction against these peptides may initiate an inflammatory response in the joints. With regard to environmental exposures, cigarette smoking is the strongest proven risk factor for rheumatoid arthritis. Cigarette smoking may lead to citrullination of proteins in the lungs, rendering them immunogenic. Citrullinated peptides have been identified in the joints of RA patients, and antibodies against citrullinated peptides are also present in the joints. Up to 70% of patients with RA have anti-CCP antibodies in the serum. Rheumatoid factor (RF), or IgM anti-IgG antibodies, is detected in approximately 80% of patients. When rheumatoid factors are deposited in joints as immune complexes, they may initiate complement-mediated inflammation within the joint. The combination of a positive RF and anti-CCP antibody are highly specific for the diagnosis of RA. However, levels of rheumatoid factor and anti-CCP do not correlate with disease activity in RA.
In RA, the synovium becomes inflamed and hypertrophied, and develops into an invasive tissue known as a pannus. The pannus, composed primarily of synovial fibroblasts, secretes matrix metalloproteinases and other enzymes that erode cartilage and stimulate osteoclasts to erode bone. These processes produce the characteristic appearance of RA on plain radiographs of joint space narrowing and marginal erosions (Figure 257-1). Several cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, IL-6, and IL-12, are elevated in rheumatoid arthritis joints. Each of these cytokines has been or is being studied as potential therapeutic targets for RA. Costimulation of T cells and B cells is important for maintenance of inflammation in RA, and drugs are approved to target this interaction. The mechanisms behind extra-articular manifestations of RA such as rheumatoid nodules, pulmonary, cardiac, and ocular involvement are not as well understood.
Figure 257-1
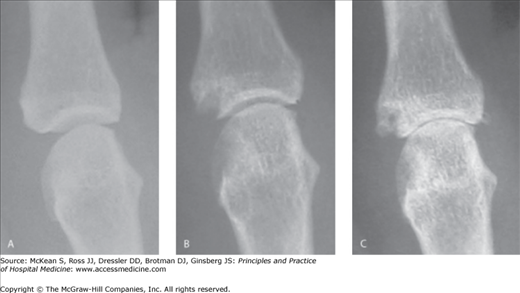
Progressive destruction of a metacarpophalangeal joint by rheumatoid arthritis. Shown are sequential radiographs of the same second metacarpophalangeal joint. (A) The joint is normal one year prior to the development of rheumatoid arthritis. (B) Six months after the onset of rheumatoid arthritis, there is a bony erosion adjacent to the joint and joint space narrowing. (C) After three years of disease, diffuse loss of articular cartilage has led to marked joint space narrowing.(Reproduced, with permission, from Imboden J, Hellmann DB, Stone JH. Current Rheumatology Diagnosis & Treatment. 2nd ed. New York: McGraw-Hill, 2007. Fig. 15-3.)
Spondyloarthropathies share some similar pathogenic mechanisms, as they are also responsive to agents that block TNF-α. These arthritides also feature erosion of bone at the joints. However, spondyloarthropathies are also characterized by bony proliferation in involved joints and the spine. In these diseases, there is significant dysregulation of bone remodeling, such that erosion and proliferation of bone may occur in different locations within the same joint. While the mechanisms of joint inflammation, pannus formation, and bone erosion in spondyloarthropathy are probably similar to those in RA, the bone proliferation is less well understood. Recent observational studies have shown that while TNF-α inhibitors decrease symptoms and inflammation in spondyloarthropathies, they do not halt bony ankylosis, which must therefore be mediated via different pathways.
Differential Diagnosis
Polyarthritis may be inflammatory or noninflammatory. In general, polyarthritis that warrants hospital admission is inflammatory. The differential diagnosis of new inflammatory polyarthritis includes not only rheumatic diseases, but also infections, neoplastic or paraneoplastic conditions, and drug reactions. Rheumatic diseases in the differential include RA, PsA, AS, undifferentiated spondyloarthropathy, polyarticular gout, pseudogout, sarcoidosis, and systemic lupus erythematosus (SLE).
Several infectious agents cause polyarthritis, either directly or indirectly (reactive arthritis). Bacterial infections with Staphylococcus aureus, group A and B streptococci, pneumococcus, and Neisseria gonorrhoeae may present with polyarthritis, usually in the setting of symptomatic or asymptomatic bacteremia with seeding of joints. Group A streptococcus can also cause poststreptococcal reactive arthritis, or less often acute rheumatic fever. Lyme arthritis due to Borrelia burgdorferi may present with intermittent inflammatory polyarthritis, or more commonly with persistent, usually monoarticular, inflammatory knee arthritis. Several viruses are associated with arthritis. Polyarthritis may be a presenting manifestation of hepatitis B, often with an urticarial rash. Hepatitis C and parvovirus B19 may mimic RA, presenting with symmetric polyarthritis and a false-positive RF. Tropical alphaviruses, such as Ross River virus, O’nyong-nyong, and Chikungunya, cause joint symptoms in most infected individuals that may persist for months. HIV may be associated with arthralgias and reactive arthritis. Bacteria can cause reactive arthritis as well, most commonly including Chlamydia trachomatis, Ureaplasma urealyticum, Salmonella, Shigella, Yersinia, and Campylobacter species; clinical features may include arthritis, urethritis, and uveitis.
Do not be fooled into thinking a hospitalized patient has RA based solely on a positive RF. Many infectious and inflammatory conditions, including infective endocarditis, tuberculosis, sarcoidosis, malignancies, and systemic lupus erythematosus and other autoimmune disorders also activate the immune system, and may result in a positive rheumatoid factor. In one study, 20% of patients with either untreated tuberculosis or Klebsiella bacteremia had positive IgM RF. Additionally, up to 55% of patients with hepatitis C infection have positive RF.
Some systemic findings may be seen in RA, although these are also seen in other conditions. Fever and leukocytosis can occur in RA, as may pulmonary and cardiac complications, including pleural effusions, pericardial effusion, and interstitial lung disease. Rheumatoid nodules occur in about 25% of RA patients, although they may not be present at the onset of RA. When present, rheumatoid nodules are associated with extra-articular disease. Fever and leukocytosis with polyarthritis may also occur with septic arthritis, viral-associated arthritis, crystal-induced arthritis, RA, adult-onset Still disease, and rare autoinflammatory conditions such as TNF receptor–associated periodic syndrome. Polyarthritis, high spiking fevers, pericarditis, neutrophilia, and an evanescent rash suggest adult-onset Still disease. Acute HIV infection or EBV infection can present with polyarthritis, fever, rash, and anemia. Systemic lupus erythematosus can cause polyarthritis; a complete blood count can help differentiate SLE from RA, as SLE is associated with cytopenias, while RA is associated with thrombocytosis and leukocytosis (and anemia). A positive antinuclear antibody (ANA) test is present in up to 30% of patients with RA. Polyarthritis accompanied by rapidly progressive interstitial lung disease, myositis, hyperkeratotic, fissuring rash, and Raynaud phenomenon is characteristic of the antisynthetase syndrome, a subset of dermatomyositis. Polyarthritis with fever may also be the presenting symptoms of sarcoidosis, which may be accompanied by erythema nodosum and hilar adenopathy.
Neoplastic processes should also be considered in the differential diagnosis of polyarthritis. Hematologic malignancies, chronic lymphocytic leukemia in particular, can induce secondary autoimmune phenomena.
The patient’s inflammatory disease history is somewhat predictive of the risk of extra-articular disease. A patient with well-controlled isolated articular disease in the past is less likely to have extra-articular disease than a patient with prior extra-articular disease. The intensity of immunosuppressive medication is also relevant. Several infectious processes can mimic extra-articular manifestations of RA, and vice versa.
The most common extra-articular manifestations of RA are rheumatoid nodules, secondary Sjögren syndrome, and pleural effusions. Less commonly, patients can develop pulmonary fibrosis, pulmonary nodules, and pericardial effusions. Felty syndrome (RA, neutropenia, and splenomegaly) used to occur in 1% of RA patients, and is now even rarer. Patients with RA are at increased risk for lymphoma. The risk of lymphoma correlates with the severity of RA disease activity, with an incidence ratio of 1.8 in individuals with RA compared to the general population. The risk does not appear to be significantly different among patients treated with different DMARD regimens. For many patients with seronegative spondyloarthropathies, arthritis is only a part of the disease. Many have associated inflammatory bowel disease, inflammatory eye disease, or psoriasis. Aortic insufficiency and apical pulmonary fibrosis are less common complications.
Febrile patients with RA should be aggressively investigated for infection. Fever related to active RA is generally low grade (≤ 38.5°C). Prior joint damage places RA patients at increased risk for septic arthritis: a tense effusion in one or more joints or a joint effusion accompanied by fever mandates diagnostic arthrocentesis. Treatment with TNF-α inhibitors increases the risk of skin infections, bacterial pneumonia, hepatitis B reactivation, and septic arthritis. Because TNF-α has a particular role in maintaining granuloma integrity, latent tuberculosis infection, and fungal infections such as histoplasmosis and coccidioidomycosis can reactivate in individuals treated with TNF-α inhibitors. In these patients, tuberculosis is often disseminated or extrapulmonary, and may present in an unfamiliar manner, as with septic arthritis or central nervous system involvement. The largest number of cases of TB in patients receiving biological agents has been reported in individuals receiving infliximab, followed by adalimumab, then etanercept. The risk of serious infection, including tuberculosis, also seems substantial with certolizumab. There are no reported cases of TB in individuals receiving abatacept or rituximab for treatment of RA. Although patients should be screened for TB before anti–TNF-α therapy, screening for TB is imperfect, and false-negative tests are common in patients with RA. Patients should also be screened for hepatitis B and C prior to starting TNF-α blockers or other DMARD therapy.
Pleural and pericardial effusions are occasionally seen in patients with RA. A pleural effusion should always be evaluated for infection, especially if the patient is taking DMARD therapy. TNF-α inhibitors can cause drug-induced lupus, usually manifesting as a rash with pleural or pericardial effusion.
Direct drug toxicity is a rare cause for admission of a patient with inflammatory arthritis. Methotrexate can cause significant anemia or other cytopenias in the setting of renal insufficiency. Mild elevations in transaminases occasionally occur with methotrexate, leflunomide, and other DMARDs. If significant elevations in aspartate aminotransferase or alanine aminotransferase are observed, both viral and autoimmune hepatitis must also be considered. More commonly, transaminase elevations in patients with inflammatory arthritis are attributable to NSAID use. Methotrexate may also cause hypersensitivity pneumonitis in up to 0.1% of treated patients. It is an idiosyncratic reaction that may occur any time during the course of therapy, most often during the first few months of therapy. The pneumonitis must be distinguished from pneumonia by bronchoscopy and biopsy, as it presents with dyspnea, cough, fever, and bilateral infiltrates on chest X-ray. There are case reports of hypersensitivity pneumonitis with leflunomide and sulfasalazine treatment.
Diagnosis
Even with advances in diagnostic testing and imaging, RA remains a clinical diagnosis, based on symptoms and examination findings, with laboratory and imaging studies as supporting evidence. Untreated patients with RA complain of morning stiffness involving numerous joints and muscle groups, lasting for at least an hour. RA is classically symmetric and leads to swelling and tenderness of the small joints of the hands, primarily the wrists, metacarpophalangeal joints, and proximal interphalangeal (PIP) joints (Figure 257-2). Other commonly involved joints include the knees, shoulders, ankles, hips, and metatarsophalangeal joints. If arthrocentesis is performed, the synovial fluid is inflammatory, generally with 2000 to 20,000 white blood cells/mm3
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


