FIGURE 1 Pain mechanisms in vulval pain: Women with vulval pain show increased pain responses to noxious stimuli on the vulva (A) and at distant sites (B). Variations in pain response and anxiety may contribute to discrete phenotypes (C) [30]. Central mechanisms appear to augment pain in women with vulval pain syndromes, both in response to stimuli on the vulva (D) and the thumb (E) [51], however, phenotypes may also be identified by clinical presentation and reflect different central mechanisms (F and G) [31].
Two brain imaging studies have been undertaken in women with vulval pain. In the first, the response to vulval pressure was assessed in women with vulval pain and pain-free controls and a central augmentation of pain was demonstrated [52] (Fig. 1d). The second, investigated the response to pressure pain on the thumb (e.g. a site distant from where the clinical pain is experienced) and looked for differences between subgroups of vulvodynia patients. There findings strongly support the need to carefully phenotype patients as they were able to demonstrate marked differences in the brain response to noxious stimulation between women with provoked and unprovoked vulval pain and more subtle differences between those with primary and secondary vulval pain [32] (Fig. 1f-g).
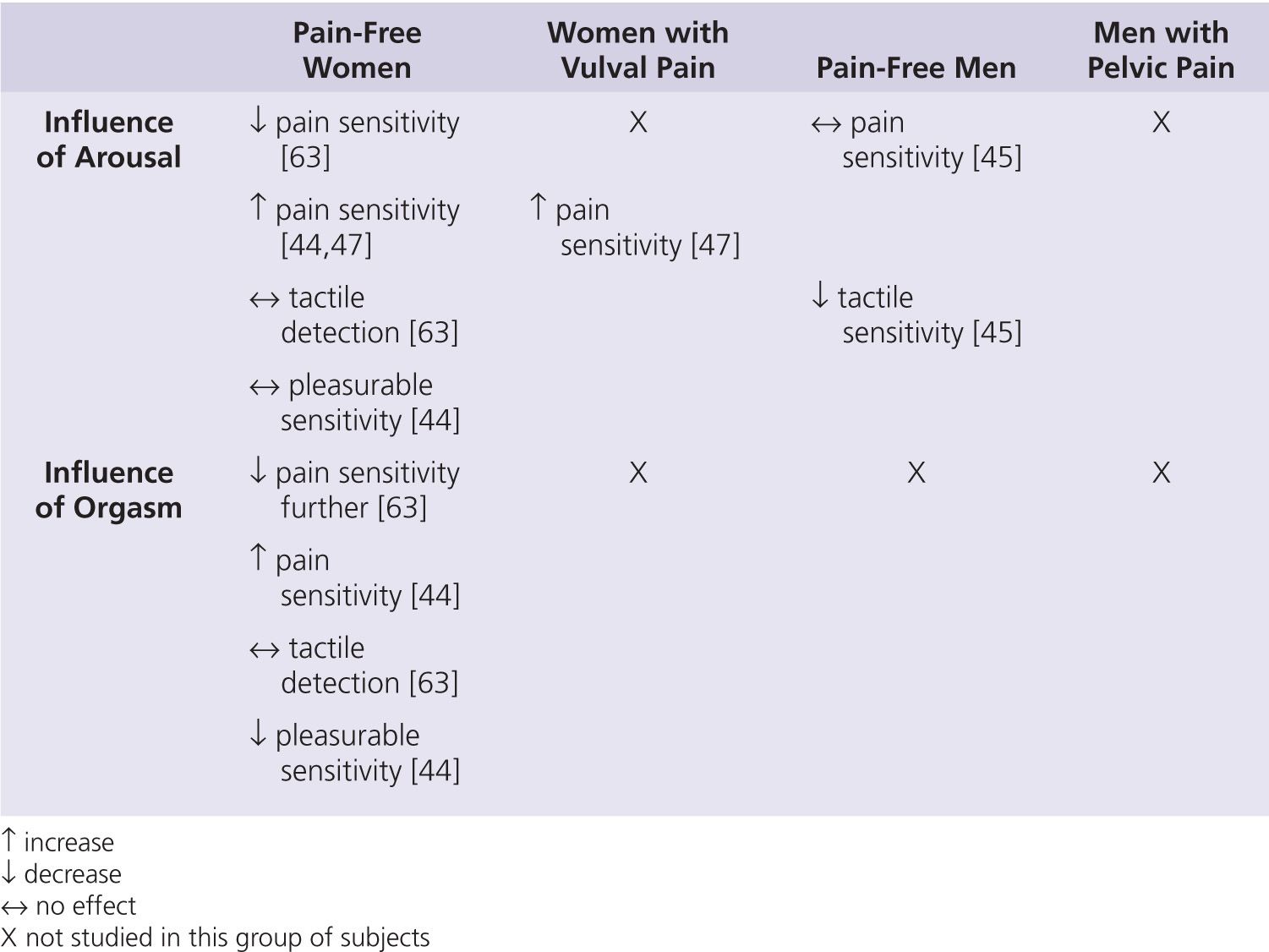
Whilst these findings support the idea that both men and women suffering from sex-related pain may have features in common with other chronic pain conditions, the relevance of these findings to the experience of pain during intercourse is harder to see. The few recent studies that have investigated the influence of sexual arousal and orgasm on sensory perception may help with our understanding. However, these studies have been relatively small and have produced contradictory results (Table 2).
Treatments
There have been few good quality randomized controlled trials investigating treatment options for sex-related pain. As with the other areas of research discussed, such studies are hampered by the heterogenous population presenting with sex-related pain or dyspareunia and the lack of a robust method of phenotyping patients. Furthermore, at present there is no gold standard treatment option to which to compare any novel treatment.
Assessment of Sex-Related Pain
The treatment of sex-related pain should ideally be individualized and multi-disciplinary. Therefore the aim of the assessment is to identify potential causative or maintaining factors or underlying pain mechanisms in order to rationalize the components of a treatment package. As always, the assessment of a patient with sex-related pain should include a detailed history, thorough examination and appropriate investigations. However, sexual dysfunction in the partners of those suffering with sex-related pain can also develop [17,35,57] and therefore an assessment of the partner may be required. It is also important to establish what the patient and potentially their partner want from treatment. Although this might appear obvious, pain-free sex may not always be the goal. For example, some may just want validation of a medical cause to their symptoms whilst others may want a pregnancy and therefore be requesting referral for consideration of assisted conception techniques.
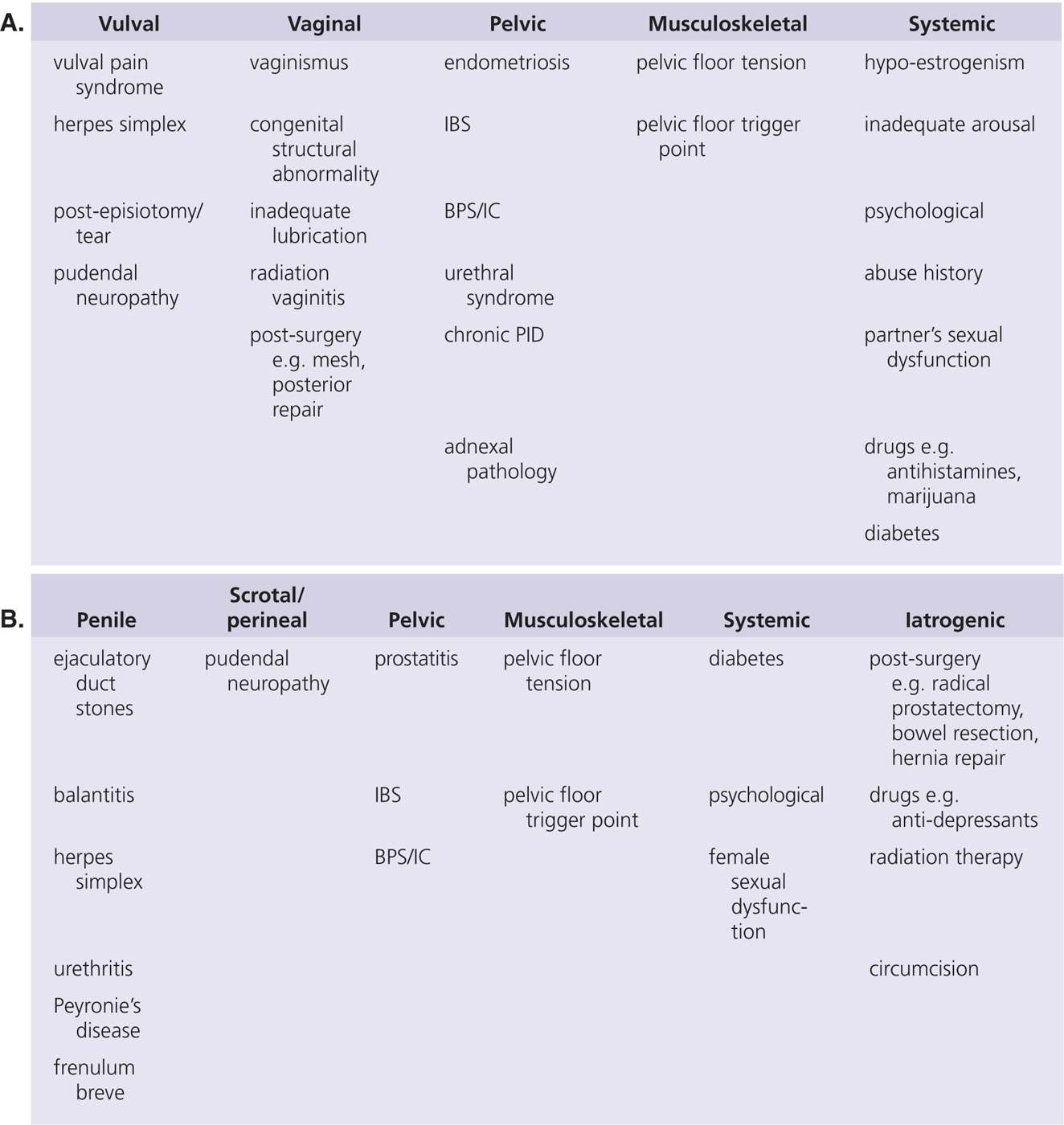
There are a wide variety of causes of pain with intercourse, many of which are reversible or subject to modification (Table 3). It is important that any assessment undertaken of a patient presenting with sex-related pain identifies or excludes these causes. Any pathology identified should be treated appropriately, however, the patient should then be carefully reassessed at a suitable interval post-treatment to ensure the pain has resolved. Many of the pathologies associated with sex-related pain are common (e.g. endometriosis, diabetes, drug use or abuse) and may therefore be an incidental finding rather than the cause of the pain. Alternatively, although they may not have been the initial cause, secondary factors such as musculoskeletal alterations and psychosexual issues may have taken over to maintain the pain such that treatment of the initial causative factor has no or minimal benefit.
Additionally, the history should establish the frequency of painful episodes and whether the pain can also occur at times not related to sex, and if it is provoked or occurs spontaneously. Such facts are important for two reasons, firstly they may point towards specific causes or potential pain mechanisms and secondly they may influence both the treatments that are considered by the clinician and those that may be acceptable to the patient. For example, a young woman whose pain only occurs with intercourse and gynaecological examinations who does not currently have a partner may consider a daily medical treatment unnecessary, whilst a woman whose pain is additionally provoked by sports and wearing tight clothes and occurs without provocation is likely to be highly motivated to try such a treatment.
Vaginismus is a common cause and consequence of sex-related pain both in women who suffer with pain and in the partners of men with sex-related pain [17,35,57]. Without identifying and treating this component, it is unlikely that pain-free intercourse will be achieved even if any other underlying factors are treated successfully. Similarly an assessment of the psychological/cognitive state of the patient and potentially their partner may point towards the need for a psychological or behavioural component within the treatment package.
Treatment of Sex-Related Pain
As described already, as with any chronic pain condition, treatment strategies should be individualized and multidisciplinary, including treatment of: any underlying physical causes; vaginismus if present; psychological distress (in either partner). Associated issues such as fertility and contraception should be addressed and the value of support groups should not be under-estimated [35]. However, there is sparse data from which to inform an evidence-based treatment plan.
There have been small trials of gabapentin [11], lamotrigine [41], desipramine and topical lidocaine [23], and BOTOX [49] in women with vulval pain, although, the results have not been particularly convincing. However, this may represent under-powered studies with a heterogenous sample rather than poor efficacy of the medication being investigated and therefore in a patient complaining of unprovoked pain or frequent episodes of provoked pain, particularly if “neuropathic” descriptors are used it would be reasonable to consider a regular pharmacological option.
Cognitive behavioral therapy (CBT) has been shown to be effective at reducing pain both in the context of provoked vulval pain [12,38] and in vaginismus [60,63]. Even more impressive, however, are the results of studies assessing the effectiveness of an Exposure-based treatment in women with lifelong vaginismus (e.g. women who have never been able to have intercourse). This program involved a maximum of three 2 hour sessions during one week, during which the women performed vaginal penetration exercises on herself initially in the presence only of a female therapist and then subsequently with her partner. Only ten women participated in the original study, however, nine of these women had intercourse after treatment and in 5 of these this was possible within the first week of treatment [58]. Moreover, the results remained at one year follow up. The authors then went on to perform a larger waiting-list controlled trial recruiting 70 women. In this study, 89% of the treated women reported intercourse by the end of the 5 week follow up period as opposed to only 11% of the control women over the 3 month control period [59]. Women in the treatment group in this study also reported significant reduction in coital fear, coital pain and sexual distress.
Special Cases
Male Ejaculatory/Post-Orgasmic Pain
Pain with or after ejaculation/orgasm in men is surprisingly common: reported in up to 4% of otherwise healthy men and up to 58% of men with another pelvic condition [36]. Perhaps unsurprisingly, however, 88–91% of men experiencing this symptom consider it to be a serious problem [34]. The pains associated with ejaculation/orgasm are varied, being located in the abdomen, pelvis or genitals [8,9] and lasting from minutes to 24 hours [8,9]. Although the aetiology of the condition is not completely understood, there are a number of known associations, including post-radical prostatectomy, ejaculatory duct stones, use of anti-depressants and pudendal neuropathy [34]. Treatment can be medical, physiotherapy or interventional. Good responses have been demonstrated with reboxetine, tamsulosin and topiramate [34], however, only tamulosin has been subjected to a placebo controlled randomized trial [42]. Similarly good results have been shown with physiotherapy, specifically treatments targeting pelvic floor trigger points [4]. Alternatively, if ejaculatory duct obstruction is present this can be relieved by dilation or resection of the ducts or if there is any evidence of a pudendal neuropathy or pudendal entrapment the nerve can be injected or surgically released [34].
Female Orgasmic Pain
In contrast to pain associated with male orgasm/ejaculation there is little to no literature on female orgasmic pain (dysorgasmia), despite the fact that an internet search will reveal copious personal descriptions of this problem. Whilst there is no published evidence to support any aetiological theories, it is plausible that both musculoskeletal factors and neuropathic mechanisms could be involved in generating the pain. In support of this, a very small case series (n=3) found a response to amitriptyline in all the women studied [2]. Other non-peer-reviewed documents also suggest the use of NSAIDs and physiotherapy. However, the one recent study implicating the use of low dose combined oral contraceptive pills (COCPs) [Rosenblum et al., unpublished] was flawed in a number of ways and therefore, to date there is no convincing evidence supporting a hormonal imbalance in the aetiology of dysorgasmia and thus no rationale to consider hormonal therapies.
Sexual Headache


Full access? Get Clinical Tree


