Fig. 24.1
The often disturbing appearance of facial injuries tends to be distracting. Attention must be paid first to proper trauma management including stabilization of the c-spine and airway management
Fig. 24.2
The face is an “anatomically dense” region. A detailed secondary survey is aimed at identifying missed injuries and repairable structures such as nerves (yellow) and ducts (green)

Fig. 24.3
Injuries of the periorbita may be those of the frontal branch of the facial nerve (a) and lacrimal duct (c). Suconjuctival hemorrhage may suggest zygoma fracture or orbital floor fracture (b)
Fig. 24.4
(a) Cheek lacerations may involve the facial nerve or parotid duct (a). (b and c) A large dog bite to this baby’s cheek involved the facial nerve buccal branches at the anterior margin of the masseter muscle. They were repaired. (d) A chainsaw laceration to the left cheek involved the facial nerve and parotid duct. The duct can be repaired over a stent
A prerequisite for managing facial injury is adequate anesthesia. For major injuries and those injuries in sensitive areas such as the periorbita, particularly in children, general anesthesia should be used liberally: there is no excuse for doing a less than rigorous repair. In adults, even large repairs can be performed with regional blocks in nearly every part of the face. Useful regional blocks include those of the supratrochlear/supraorbital, infraorbital, and mental nerves block (Figs. 24.5, 24.6, and 24.7). A regional block should be placed first, and only then supplemented with local infiltration. The eyes should be protected during injection and repair.
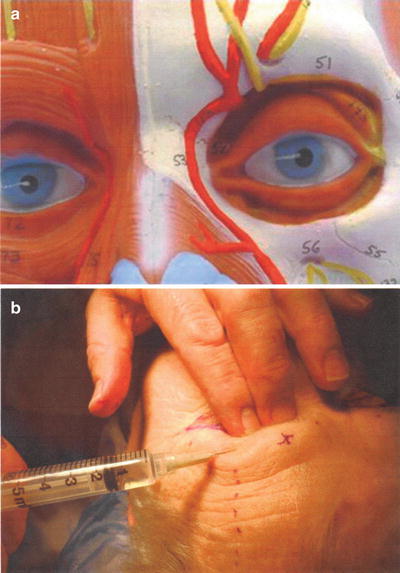
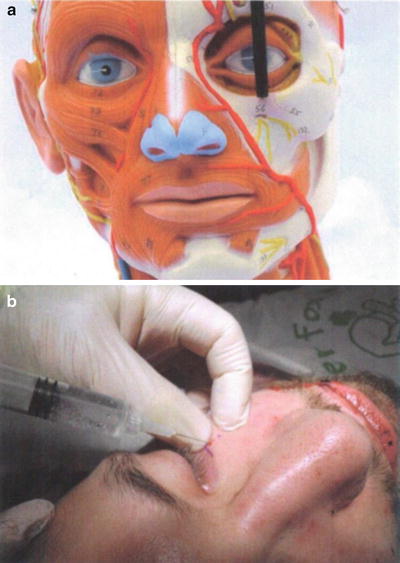
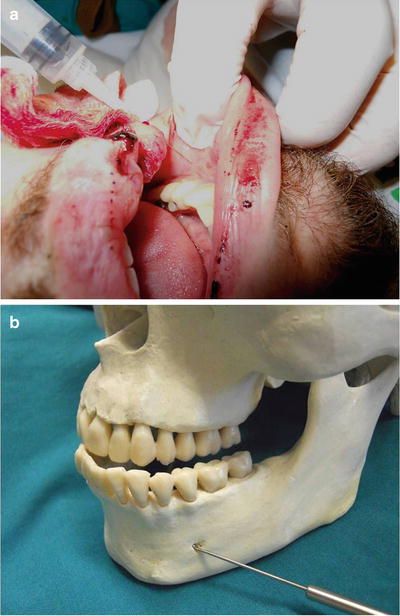
Fig. 24.5
(a) The supratrochlear and supraorbital nerves are blocked by injecting along the superior orbital rim. (b) While blocking the nerves, the supraorbital rim is palpated to protect the orbit. This block will block the forehead and anterior scalp
Fig. 24.6
(B) The infraorbital nerve is blocked by palpating and injecting the infraorbital foramen just below the inferior orbital rim. Alternately, the needle may be introduced at the alar base and directed up to the foramen. (A) The orbital rim is palpated while injecting at the foramen to protect the orbit. This block will anesthetize the upper lip and cheek 24 Repair of Soft Tissue Facial Injuries
Fig. 24.7



(a) The mental foramen is located below the second biscuspid. (b) It may be blocked by injecting just beneath the mucosa of the labial sulcus at the second bicuspid. This will block the lower lip but not the chin
Related posts:




Full access? Get Clinical Tree
