Fig. 17.1
Hand and needle position for performing a trigger point injection of the abdominal wall
Local Anesthetic
Multiple combinations of local anesthetics and adjuvants have been described for trigger point injection. There is little evidence that any one local anesthetic is superior to another, or that injectate of any kind is superior to dry needling. Local anesthetics that have been used include: lidocaine, procaine, mepivacaine, ropivacaine, and bupivacaine. Additives such as methylprednisolone or triamcinolone can be added. The authors suggest using equal parts 2 % lidocaine and 0.75 % bupivacaine with 40 mg of triamcinolone per 10 mL of solution. Avoidance of epinephrine may be important as vasodilation at the site is thought to be beneficial in the treatment of the trigger point.
Anticipated Results/Possible Complications
The anticipated result is that pain at the trigger point will dissipate over 5–10 min as the local anesthetic takes effect. Long-term or permanent pain relief may occur following single injections; however, repeat injection may be required. Complications include intraperitoneal needle placement, hematoma formation, needle breakage, infection, vasovagal syncope, intravascular injection and local anesthetic toxicity, scarring and failure of the procedure.
Scar Injections
Peripheral Nerve Block Techniques
Intercostal Nerve Block (ICNB)
The dorsal and ventral roots of the spinal cord unite to form 31 paired spinal nerves. The spinal nerves then exit through the intervertebral foramen and divide into several branches including the ventral and dorsal primary rami. The dorsal rami supply the paravertebral area with motor and sensory functions. The anterior primary rami of T1 through T11 make up the intercostal nerves. T12 is technically a subcostal nerve as it does not run between two ribs, but rather under the twelfth rib. The intercostal nerves run in the subcostal groove on the inferior side of each rib. The nerve is inferior to the posterior intercostal artery, which is itself inferior to the intercostal vein. The intercostal nerves travel between the internal intercostal and the innermost intercostal muscles (Fig. 17.2). Each nerve gives off a lateral cutaneous branch just anterior to the mid-axillary line, which supplies the muscles and skin of the anterior and lateral torso. The intercostal nerves end as an anterior cutaneous branch. For the lower six intercostal nerves, which are applicable to abdominal pain, this branch terminates after piercing the rectus sheath to provide motor function and sensation to the anterior abdominal wall near the midline.
Fig. 17.2
Intercostal nerve block (ICNB): cross-sectional anatomy. Reprinted with permission from David L. Brown, Atlas of Regional Anesthesia, 4th edition, 2010, Elsevier
Procedure
An intercostal nerve block (ICNB) performed proximal to the take off of the lateral cutaneous branch will provide unilateral anesthesia/analgesia for the lateral and anterior thorax in a dermatomal pattern defined by the distribution of each specific nerve. Since spread to adjacent nerves is unlikely, each intercostal nerve must be blocked separately. This is a pure somatic block and no visceral coverage is provided.
Indications/Contraindications
ICNBs for abdominal pain are indicated when somatic pain arises from the muscles, nerves, or connective tissues of the abdominal wall. Therefore, they can be used to treat trigger points, intercostal neuralgia and herpes zoster pain, rib fractures, post-thoracotomy pain, hernia pain, tumor-related pain, and musculoskeletal pain of the abdominal wall. They can also be used to distinguish somatic pain from visceral pain.
ICNB are contraindicated in patients who may not tolerate a pneumothorax, such as those with severe underlying pulmonary pathology or previous contralateral pneumonectomy. Local infection and allergies to local anesthetics or adjuvant medications are also contraindications. Caution should be used for patients on anticoagulation; however, this is not an absolute contraindication and clinical judgment should be exercised.
Equipment
Skin marking pen, skin prep, gloves, and drape if desired.
Twenty-five gauge needle, 1.5 % lidocaine, and 5 mL syringe for skin wheel.
Twenty-one gauge short bevel 5 cm needle for block placement.
Extension tubing.
Syringe and local anesthetic for ICNB.
Techniques
Landmark technique: For performance of the block the patient may be sitting, lateral, or prone. Most commonly, the block is performed at the angle of the rib just lateral to the sacrospinalis muscles, which is approximately 6–8 cm from the vertebral spines. Blockade at this location should anesthetize the intercostal nerve prior to the takeoff of the lateral cutaneous branch. Additionally, at this point the ribs are superficial making palpation easier and the intercostal spaces are thicker so the risk of pleural puncture is decreased. The distance from the midline also minimizes the chance of proximal spread into the neuraxis. A marking pen is used to mark the spinous processes that correspond to the ribs and intercostal nerves to be blocked. The rib is palpated laterally and marked 6–8 cm from the midline. The mark should be lateral to the sacrospinalis muscles at the inferior border of the rib of interest. The skin is prepped and 1 % lidocaine is injected for skin wheel. The short bevel needle with extension tubing and local anesthetic connected is placed through the skin wheel. The goal of the block is to place the needle just off the inferior edge of the rib while angling the needle cephalad 20°. To do so, the skin overlying the intercostal space is pulled superior to lie over the rib, the needle is inserted to contact the rib, and then the skin is released as the needle is “walked” inferiorly until it just slips off the inferior margin of the rib. The cephalad angulation of the needle must be maintained to maximize block success (Fig. 17.3). The needle is advanced approximately 3–4 mm past the rib. Negative aspiration is ensured and 3–5 mL of local anesthetic is injected.
Fig. 17.3
ICNB: stepwise technique (1–6). Reprinted with permission from David L. Brown, Atlas of Regional Anesthesia, 4th edition, 2010, Elsevier
Ultrasound technique: An in-plane ultrasound-guided technique can also be used to perform an ICNB. Ultrasound has been shown to be as equally effective as fluoroscopy for this procedure [7]. A linear ultrasound probe is placed on the patient’s back at a point that corresponds to the angle of the rib as described above. The probe is placed vertically over the ribs so that the ribs both above and below the intercostal space of interest can be seen (Fig. 17.4). Because of the caudal angulation of the ribs, the probe should be slightly oblique with the cephalad end of the probe being more lateral than the caudal end. In this fashion the probe will be perpendicular to the rib. The skin is anesthetized and the injection needle is inserted caudal to the probe and in-plane. It is advanced until it is 3–4 mm under the inferior border of the rib. Oftentimes, the pleura can be visualized as a bright white line deep to the ribs. As local anesthetic is injected, spread should be seen in the intercostal space posterior to the pleura. The major advantage of ultrasound for ICNB is a potential reduction in the risk of pneumothorax.
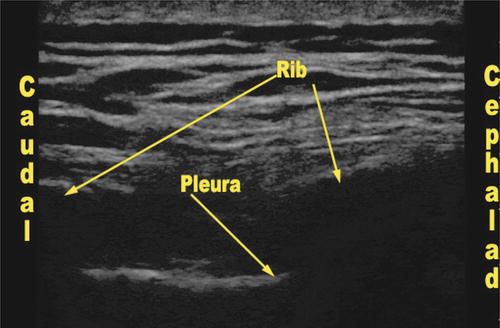
Fig. 17.4
Ultrasound view during intercostal nerve blockade with ultrasound transducer positioned vertically to show two adjacent ribs in cross-section
Local Anesthetics
An ICNB can be performed using a variety of local anesthetics. Bupivacaine 0.25–0.5 %, Ropivacaine 0.5–0.75 %, Lidocaine 1–2 %, and Mepivicaine 1–2 % can be used depending on the desired onset time and duration of block. For prolonged analgesia Bupivicaine or Ropivicaine are appropriate, while Lidocaine and Mepivicaine provide a shorter onset time. Epinephrine 1:200,000 or 1:400,000 should be added to the solution to reduce systemic absorption and as a marker for intravascular injection. It is important to note that systemic absorption following ICNB is higher than with any other nerve block, so maximal local anesthetic doses should not be exceeded and caution should be taken when multiple injections are being performed. Steroids may be added to the injectate solution if desired.
Anticipated Results/Complications
An ICNB results in loss of both motor function and sensation in the distribution of the individual intercostal nerve. Several sequential ICNB may be needed as the distribution of neighboring nerves may overlap.
Complications include pneumothorax, hemothorax, nerve injury, local anesthetic toxicity, and hematoma formation. There is also risk of penetrating the peritoneal cavity and injuring underlying abdominal viscera. Rarely, spread of local anesthetic to the spinal space may occur from injection into the dural sheath.
Thoracic Paravertebral Block (TPVB)
The thoracic paravertebral space is a triangular-shaped area adjacent to the spinal column on both sides. Within this space are the spinal nerves, which have exited the intervertebral foramen, and the sympathetic chain. It also contains fatty tissue, dorsal rami, rami communicantes, and the intercostal vessels. The paravertebral space is bordered by the parietal pleura anterolaterally, the vertebral body and disk medially, and the costotransverse ligament, ribs and transverse process posteriorly (Fig. 17.5). Continuing laterally, the paravertebral space is continuous with the intercostal space. Medially, it is continuous with the epidural space. The paravertebral space runs from the cervical region to the origin of the psoas muscle at the twelfth thoracic vertebrae.
Fig. 17.5
Anatomy of the thoracic paravertebral space. Reprinted with permission from Samer N. Narouze, Atlas of Ultrasound-Guided Procedures in Interventional Pain Management, 2010, Springer
Procedure
The thoracic paravertebral block (TPVB) can be thought of as unilateral epidural blockade as it results in unilateral blockade of sympathetic and somatic nerves and resultant ipsilateral dermatomal anesthesia. The injection of local anesthetic into this space results in analgesia/anesthesia of the spinal nerves. It has the potential advantage of minimizing autonomic dysfunction that accompanies neuraxial techniques, thus making it an attractive option for treatment of unilateral pain of the abdomen. Because the paravertebral space at one level may be continuous with the paravertebral spaces both above and below, a single injection of local anesthetic may result in blockade of multiple levels [8]. However, dependent on the patient’s anatomy and the injection site, local anesthetic injection may be more confined [9]. Potential spread may also depend on the volume of local anesthetic injected.
Indications/Contraindications
The indications for a TPVB include rib fractures, upper abdominal wall pain both acute and chronic, herpetic neuralgia, acute herpes zoster, intercostal neuralgia, liver capsule pain, post-thoracotomy pain, and sympathetic blockade such as for the treatment of hyperhidrosis [10].
Contraindications include local and systemic infection and allergies to local anesthetic or adjuvants. Because there is also a risk of pneumothorax, this block should be avoided in patients who would not tolerate such complication. While anticoagulation is not an absolute contraindication for paravertebral blockade, the risk of bleeding and potential epidural hematoma formation are present, thus careful consideration should be given when performing this block in patients who are systemically anticoagulated.
Equipment
Marking pen, skin prep, gloves, and drape. Equipment specific for the technique.
1.5 in. 25 gauge needle, 5 mL syringe, and 1.5 % lidocaine for local skin wheel.
Needle: For single injections a 17–22 gauge Tuohy needle may be used. Alternatively, a 90–100 mm short bevel needle or a 22 gauge 3.5 in. Quincke needle may be used. For the placement of an indwelling catheter, a 17 gauge Touhy needle is needed depending on catheter size.
Local anesthetic of choice, extension tubing and syringe.
Techniques
Landmark Technique: Patients can either be sitting or lateral during performance of a paravertebral block. As the block can be uncomfortable, especially if multiple injections are being performed, sedation is often necessary making the lateral position attractive. The spinous processes are identified and marked. Helpful landmarks for identification of specific spinous processes include the inferior angle of the scapula at T7. It is important to recall that because the spinous processes of the thoracic vertebrae are angled caudally, the spinous process of one vertebrae overlies the transverse process of the vertebrae below it. For example, the spinous process for T8 overlies the transverse process of T9. From the cephalad border of the spinous process of interest, a mark is made 2.5 cm laterally. This location is the needle insertion site for the block. After prepping the skin, and injecting local anesthetic for a skin wheel, the procedural needle is inserted perpendicular to the skin in all planes to contact the transverse process. The depth of this bone is variable depending on the thoracic level being blocked, but is deepest at the upper and lower thoracic spine (5–8 cm) and shallowest in the mid-thoracic spine (2–4 cm). After contacting the transverse process the needle is redirected caudally to walk off its inferior edge. The needle is advanced 1 cm past the depth at which the transverse process was located. Occasionally, a pop will be felt as the needle passes through the costotransverse ligament; however, this is unpredictable. After negative aspiration for cerebrospinal fluid (CSF), blood, and air, local anesthetic is injected. If a catheter is to be placed, it can be inserted through the Tuohy needle and threaded 3–4 cm.
Loss or Resistance Technique
The thoracic paravertebral space may also be located using a loss of resistance (LOR) technique. The procedure is identical to the landmark-based approach, except that it is routinely performed with a Tuohy needle and LOR syringe. After contacting the transverse process the needle is redirected inferior to the transverse process. The LOR syringe is then connected using either saline or air, depending on operator preference. The needle is slowly advanced while periodically checking for a LOR as the needle passes through the costotransverse ligament. This LOR can be subtle and can be difficult to appreciate, especially for those with less experience performing this technique. The LOR should occur within the first centimeter past the transverse process, and if it is not found within this distance the needle should be withdrawn, the landmarks checked, and the block procedure repeated. Once LOR is obtained, local anesthetic can be injected and a catheter can be placed if desired.
Ultrasound Technique
Various ultrasound-guided approaches to thoracic paravertebral blockade have been described [11–13]. Ultrasound can be used to locate and mark both the midline and transverse process in order to facilitate the landmark, or LOR technique, as well as to perform blockade in real-time. With the patient supine or lateral, a linear probe, or curvilinear probe for obese patients, is placed on the patient’s back in a horizontal orientation and used to locate the spinous process adjacent to the level of interest. The probe is then moved laterally to locate the transverse process as a hyperechoic structure with acoustic shadowing. The probe is then slid caudally into the intercostal space to obtain a view of the parietal pleura. This often requires a slightly oblique orientation of the ultrasound probe since the ribs angle inferiorly as they move laterally. With the transverse process and parietal pleura in view, the procedure needle is inserted in-plane from the lateral side of the ultrasound probe (Fig. 17.6). The needle is advanced into the paravertebral space just posterior to the parietal pleural and, following negative aspiration, local anesthetic is injected. Catheter placement can follow if desired.
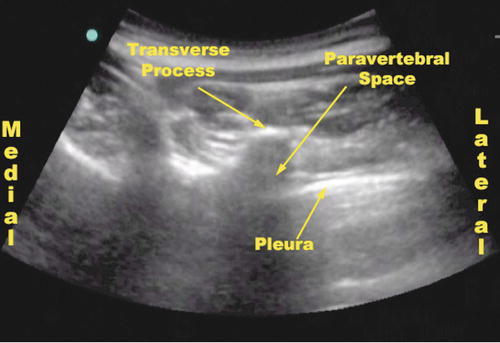
Fig. 17.6
Ultrasound view of the thoracic paravertebral space with the ultrasound probe oriented horizontally, and placed lateral to the midline
Local Anesthetic
The choice of local anesthetic for thoracic paravertebral blockade will vary depending on the indication for nerve blockade. For diagnostic blocks a short acting local anesthetic such as lidocaine or mepivicaine is sufficient. However, in cases where longer duration of analgesia is desirable, 0.25–0.5 % bupivacaine or 0.5–0.75 % ropivicaine should be used. Epinephrine 1:200,000 or 1:400,000 should be added as a marker for intravascular injection and to potentially slow systemic absorption of the local anesthetic. When multiple levels are being blocked 4–5 mL per level should be used to minimize the overall dose of local anesthetic. When a single level injection is performed, a similar volume can be used if spread to adjacent nerve roots is not required. Volumes of 15–25 mL can be used for single level injections and may increase the spread of the block to multiple dermatomes.
Anticipated Results/Complications
Both motor and sensory blockade result from a TPVB as a result of anesthetizing the individual spinal nerves after they exit the intervertebral foramina. The number of dermatomes affected depends on both the number of levels blocked and also the spread of local anesthetic within the paravertebral space. Somatic coverage is expected, but some visceral coverage may result as well [14–16].
The complications of this block include: pneumothorax, bleeding, hemothorax, local anesthetic toxicity, autonomic dysfunction, and hypotension and nerve injury. There is also the possibility of local anesthetic spread to the epidural, subdural, and subarachnoid spaces.
Lumbar Paravertebral Block/Lumbar Somatic Block (LPVB)
The lumbar paravertebral space is a potential space formed by the vertebral body, intervertebral discs and intervertebral foramen medially, the psoas major muscle anterolaterally, and the transverse processes and intertransverse ligaments posteriorly. There is no costotransverse ligament in the lumbar region. The lumbar spinal nerve roots run through the paravertebral space and continue through the psoas major muscle where they form the lumbar plexus. Because the lumbar paravertebral space does not routinely communicate with the thoracic paravertebral space, local anesthetic injected into one region cannot be expected to spread to the other.
Procedure
Similar in concept to the TPVB, the lumbar paravertebral block (LPVB) aims to anesthetize the individual lumbar spinal nerve roots shortly after they exit the vertebral foramen. If small volumes of local anesthetic solution are injected, individual nerve roots may be blocked to aid in the diagnosis of pain originating from specific lumbar nerves. Upper lumbar nerves can often be blocked without resultant motor weakness. However, if spread occurs to the L2 nerve root or below, motor weakness may occur as a result of obturator or femoral nerve blockade. Just as with thoracic paravertebral blockade, epidural spread can occur in the lumbar region. Additionally, sympathetic blockade may occur as a result of local anesthetic injected into this area.
Indications/Contraindications
The indications for lumbar paravertebral nerve blockade include somatic lower abdominal and groin pain. Selective blockade of individual spinal nerves can help localize the origin of abdominal pain to specific lumbar nerve roots. This may be beneficial for the diagnosis and treatment of spinal and foraminal stenosis. Additionally, they may be used to assist in the diagnosis and treatment of chronic abdominal pain that results from nerve entrapment after inguinal herniorrhaphy.
Contraindications for this block are similar to those for TPVB. These include both local and systemic infection as well as an allergy to either local anesthetic or adjuvant medications. Because the needle is in close proximity to the epidural space and because this block is performed in a non-compressible area, caution should be used when performing this block on patients who are on anticoagulant medications.
Equipment
Marking pen, skin prep, sterile drape, and gloves.
1.5 in. 25 gauge needle, 5 mL syringe, and 1.5 % lidocaine for local skin wheel.
Eighteen to twenty-two gauge Tuohy needle or a 22 gauge Quincke needle for single injection.
Local anesthetic of choice, extension tubing and syringe.
Technique
LPVB can be performed with the patient either sitting or lateral. If the block is to be performed in the lateral position, the side to be blocked should be in the up position. The spinous processes are identified and marked. Important landmarks in this region include the iliac crests, which correspond to L3–L4 interspace. From the superior edge of the spinous process of interest, a mark is made 2.5 cm lateral to the midline. If lower lumbar nerve roots are to be blocked, the distance from the midline can be 2 cm as the transverse processes in the lower lumber region are shorter. The skin is prepped and a skin wheel of local anesthetic is raised at this mark. The injection needle of choice is then inserted through the skin wheel and kept perpendicular to the skin in all planes. The needle is advanced to contact the transverse process, which will normally be located in lumbar region at the depth of 4–8 cm depending on the patient’s body habitus, and the lumber level being approached. The needle is then withdrawn and redirected to walk caudally under the transverse process and advanced 1 cm past the depth at which the transverse process was located. After negative aspiration for CSF and blood, local anesthetic is injected.
Local Anesthetic
The choice of local anesthetics for lumbar paravertebral blockade is essentially the same as those for thoracic paravertebral blockade. Short acting fast onset local anesthetics can be used for diagnostic purposes, while local anesthetics with a longer duration can be used for the treatment of pain. Steroids may be added to the local anesthetic mixture if so desired and may be beneficial in the treatment of certain conditions, such as foraminal stenosis.
Anticipation/Complications
Lumbar paravertebral blockade will provide unilateral dermatomal anesthesia corresponding to the specific nerve root(s) that are blocked. With small volumes of local anesthetic (2–3 mL), local anesthetic may remain isolated to a single nerve root; however, larger volumes (>5 mL) may spread to adjacent nerve roots. For this reason small volumes should be used for diagnositic purposes to minimize the chance of spread if this is not desired.
Complications include hematoma formation, retroperitoneal bleeding, intra-abdominal needle placement and visceral injury, infection, local anesthetic toxicity, nerve injury and epidural, subdural or subarachnoid spread of local anesthetic. These last three could lead to undesired motor block, sympathectomy, and hypotension. Motor weakness may also occur as a result of nerve root blockade below L2 as a result of femoral or obuturator nerve anesthesia.
Ilioinguinal/Iliohypogastric Nerve Blocks
Both the ilioinguinal (II) and iliohypogastric (IH) nerves are components of the lumbar plexus. The L1 nerve root forms the II nerve, while the T12 and L1 nerve roots form the IH nerve. After these nerve roots exit the vertebral foramen they travel through the paravertebral space and contribute to the formation of the lumbar plexus posterior to the psoas major muscle. As the II and IH continue laterally, they pass through the transversus abdominis muscle to lie between it and the internal oblique muscle. As they continue around the abdominal wall towards the midline, they will at some point separately pass through the internal oblique muscle to lie between it and the external oblique. The points at which the nerves traverse the internal oblique muscle are variable. However, when the block is performed posterior to the anterior iliac spine as described below, the nerves lie between the internal oblique and transversus abdominis muscles in the vast majority of patients [17, 18]. The II nerve supplies cutaneous sensation to the upper and medial thigh and upper part of the genitalia. The IH nerve supplies some motor function to the lower abdominal musculature as well as cutaneous sensation to the suprapubic region and a small segment near the iliac crest.
Procedure
By placing local anesthetic between the internal oblique muscle and the transversus abdominis muscle, both the II and IH nerves can be anesthetized using ultrasound guidance. Although landmark-based techniques have previously been described, accurate placement of local anesthetic is inconsistent and success rates are low [19]. The result of successful blockade is ipsilateral anesthesia of the lower abdomen and inguinal region. No visceral coverage is supplied by blockade of these nerves.
Indications/Contraindications
For chronic pain, II and IH nerve blocks are commonly performed during the diagnosis and treatment of lower abdominal/inguinal pain/neuralgia. One major reason for chronic abdominal pain in this area is previous inguinal hernia repair [20].
The contraindications for II/IH nerve blockade are limited, but include local infection at the block location, implanted material in the area of the injection such as mesh and allergies to local anesthetics or adjuvants.
Equipment
Gloves, marking pen, chlorhexidine, or alcohol for prep and sterile drape if desired.
1.5 % lidocaine and syringe for skin wheel.
Twenty-one gauge short bevel needle or 22 gauge Quincke spinal needle.
Extension tubing and 10–20 mL syringe for local anesthetic.
Local anesthetic for procedure.
Ultrasound machine and linear probe.
Technique-(Ultrasound)
With the patient supine, the anterior superior iliac spine (ASIS) is located and marked. The ultrasound transducer is placed horizontally on the patient’s abdomen slightly superior and lateral to the ASIS. The lateral edge of the probe should be just over the iliac crest so that it can be seen on the edge of the ultrasound screen as a hypoechoic structure. The probe is then oriented obliquely so that the lateral edge is slightly caudal compared to the medial edge. This helps align the ultrasound beam perpendicular to the nerves. The ultrasound image will show three distinct muscles layers at this location, corresponding from superficial to deep to the external oblique muscle (EO), internal oblique muscle (IO), and transversus abdominis muscle (TA) (Fig. 17.7). Normally, the II and IH nerves can be seen between the IO and TA muscles as one or two hyperechoic structures. The nerves may be one structure or two separate structures depending on the patient’s anatomy. The deep circumflex iliac artery, or a branch of it, usually accompanies the II nerve at this location and can be used as a landmark. Doppler can be used to assist in identifying the artery. Occassionaly, the nerves can’t be identified between the two muscles layers, but local anesthetic can still be injected into the plane between the two muscles. Once the plane between the IO and TA muscles has been identified, the skin is prepped and a skin wheel is raised medial to the probe. The procedure needle is then brought in-plane from medial to lateral with a shallow angle and passed through the EO and IO muscles. Once the needle tip is between the IO and TA muscles and adjacent to the II and IH nerves, negative aspiration is verified and local anesthetic is injected.
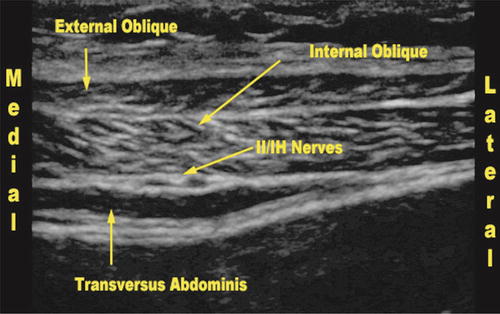
Fig. 17.7
Ultrasound view for ilioinguinal/iliohypogastric nerve blockade
Local Anesthetic
Because prolonged pain control is usually desired, long acting local anesthetics are primarily used for II and IH nerve blocks. Epinepherine should be routinely added to the local anesthetic as a marker for vascular injection secondary to the presence of the deep circumflex iliac artery and the possibility of intravascular injection. Bupivacaine 0.25 %, bupivacaine 0.5 %, or ropivacaine 0.5 % may all be used, with the latter two providing a denser block. 5–10 mL of local anesthetic can be used per side with lower volumes being adequate when accurate needle placement is obtained.
Anticipation/Complications
The II and IH nerves are usually blocked together as a method of selective blockade has not been proven. Blockade of these two nerves results in ipsilateral cutaneous anesthesia of the lower abdomen, genital region, and upper thigh. The distribution of sensory anesthesia for each nerve is variable, thus it is difficult to discern which nerve is the source of pain or relief following blockade [21].
Complications from II/IH nerve blocks include infection, nerve injury, intravascular injection and local anesthetic toxicity, abdominal hematoma formation, intra-abdominal needle placement and visceral injury, pelvic hematoma, femoral nerve block, and bowel puncture.
Rectus Sheath Block
The rectus abdominis (RA) muscles are paired anterior abdominal muscles, which run vertically on either side of the midline. They are separated at the midline by the linea alba and are bordered laterally on both sides by the linea semilunaris. The rectus sheath is comprised of the RA muscles and the aponeuroses of the internal oblique (IO), external oblique (EO), and transversus abdominis (TA) muscles. Which aponeuroses travel anterior to the RA muscle and which travel posterior to it depends on the location relative to the arcuate line. The aponeuroses of all three lateral abdominal wall muscles travel anterior to the RA muscle below the arcuate line. Above the arcuate line the aponeurosis of the IO muscle splits around the RA muscle. The RA muscle also normally contains three transverse tendinous intersections which compartmentalize the rectus muscle. However, these are usually incomplete and do not attach to the posterior rectus sheath [22].
Procedure
The anterior cutaneous branches of the lower intercostal nerves enter the rectus sheath from the posterior and lateral side to provide sensory innervation to the anterior abdominal wall and motor supply to the abdominal muscles [23]. There is no visceral coverage provided by this somatic block. The goal of a rectus sheath block is to place local anesthetic posterior to the rectus abdominis muscle and immediately anterior to the rectus sheath and transversalis fascia. In this location, the local anesthetic will be in close proximity to the anterior cutaneous branches of the intercostal nerves.
Indications/Contraindications
As the rectus sheath block only provides anesthesia or analgesia of the anterior abdominal wall with close proximity to the midline, its indications are limited to pain in this distribution. It may be utilized to treat and define pain that stems from nerve entrapment or pain following midline surgeries or hernia repairs. It can also be used to treat neuropathic pain such as that from post-herpetic neuralgia [24].
Contraindications are limited but include allergies to local anesthetics or adjuvants and local infection. Caution should be used when performing this block on anticoagulated patients; however, this is not an absolute contraindication.
Equipment
Gloves, chlorhexidine or alcohol for skin prep, and drape if desired.
Five mL syringe, 25 gauge 1.5 in. needle and 1.5 % lidocaine for skin wheel.
Extension tubing and 20 mL syringe.
Local anesthetic for procedure.
Twenty-one gauge 9 cm short bevel needle or 22 gauge Quincke needle.
Ultrasound machine and linear probe.
Technique
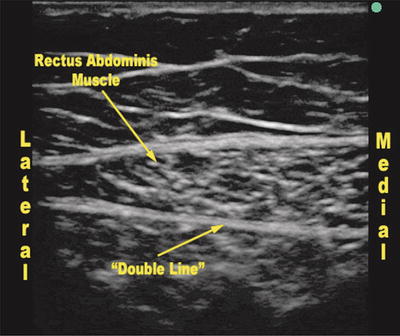
Although a landmark-based approach relying on tactile feedback has been described, the possibility of peritoneal needle placement and visceral injury are concerns [25]. As a result, ultrasound can be used to perform the block. The ultrasound probe is oriented horizontally on the abdomen in short-axis to the RA. Both in-plane and out-of-plane needle approaches are possible, but an in-plane approach allows for view of the entire needle. As the RA runs from the xiphoid process to the pubic symphasis, a rectus sheath block can be performed anywhere along this course depending on the location of pain and the underlying pathology. The block is most easily performed above the arcuate line, which is roughly 1/2 way between the umbilicus and pubic symphasis, as the posterior rectus sheath is more substantial above this point. With the patient supine, a linear ultrasound probe is placed adjacent to the location of the patient’s pain so that the rectus muscle, posterior sheath, and underlying abdominal contents can be seen. Since branches of the intercostal nerves enter the RA muscle from the posterior and lateral side, this is the area that should be targeted. The RA muscle will appear as an oval muscular structure deep to the subcutaneous tissue. Deep to this a double hyperechoic line can be seen (Fig. 17.8). The more superficial of these two lines represents the aponeuroses of the lateral abdominal muscles. The second, deeper, line is the transversalis fascia. Under these structures are pre-peritoneal fat, the peritoneum, and viscera. After skin prep and injection of local anesthetic for skin wheel, the procedural needle is inserted in-plane. The objective of the block is to place the needle tip and local anesthetic between the posterior wall of the RA muscle and the aponeuroses of the lateral abdominal wall muscles. The local anesthetic should “lift” the RA muscle off the double hyperechoic line. Of note, if the block is being performed below the arcuate line, only a single hyperechoic line may be seen as the rectus muscle is lying directly on the transversalis fascia as all aponeuroses from the lateral abdominal wall muscles go anterior to the rectus muscle. The approach can be either from the medial or lateral side of the probe. Depending on the extent of desired abdominal coverage, multiple injection sites may be chosen.
 Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
 Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
 Peripheral Nerve Stimulation for Chronic Abdominal Pain
Peripheral Nerve Stimulation for Chronic Abdominal Pain
 The Epidemiology of Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain



Related posts:
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Peripheral Nerve Stimulation for Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain
Full access? Get Clinical Tree
