1. Large prospective studies indicate that regional anesthetics have a high degree of safety and efficacy in pediatric patients, and can be used for intraoperative anesthesia, postoperative analgesia, and for a variety of painful conditions.
2. The performance of regional blocks under general anesthesia is as safe or safer than doing so while the patient is awake or sedated.
3. The utilization of ultrasound (US) guidance has enabled the widespread use of peripheral nerve blocks, both by single injection and with continuous catheter techniques. These blocks may be used in place of central neuraxial blockade in many circumstances. There is some evidence that US may result in improved safety and efficacy of peripheral nerve blocks and may in some circumstances allow a block to be performed with lower doses of local anesthetic (LA).
4. Strict attention to technique, including drug administration and drug dosing, is critical to ensuring both success and safety, as the scale of size in pediatrics imposes more stringent anatomic constraints and pharmacologic thresholds of drug toxicity, especially in infants and smaller children. A thorough understanding of the anatomy of the block is necessary.
5. As in adults, “lipid rescue” is now the mainstay of treatment for LA toxicity.
REGIONAL ANESTHESIA, INCLUDING PERIPHERAL and central neuraxial blockade, is indicated for a variety of surgeries as well as for the treatment of postoperative pain, trauma-related pain, palliative care, and many chronic pain syndromes. Regional anesthetics can decrease the detrimental hormonal stress response to pain, which is three to five times greater in neonates when compared to adults (1,2). It can also lessen the severity and prevalence of phantom limb pain after an amputation, provide better postoperative analgesia, and prolong pain relief for days to weeks after a surgical insult (3,4). Finally, regional anesthesia enables the reduction or elimination of systemic analgesic medications, thereby providing analgesia with fewer side effects. Its effective use, however, requires a thorough understanding of anatomy, equipment and technology, pharmacology and processes by which regional anesthetics are employed, and the appropriate indications and contraindications to blockade in infants and children.
GENERAL PRINCIPLES
There are several keys to successful pediatric regional anesthesia.
1. History and physical examination of the patient should be thorough, paying special attention to details that may dictate, mandate changes in, or contraindicate therapy. Examples include a patient who is or will be anticoagulated, a patient with infection at the block site, a patient with progressive neuromuscular disease, or one in whom neuromuscular function testing is required in the postoperative period.
2. Have a good knowledge of the patient’s anatomy and your equipment. The distance to the nerve from the skin is shorter in children, so it is important to use very slow, deliberate, fine movements.
3. Obtain informed consent, letting the parent and the patient know what to expect using age-appropriate language. List the most likely potential complications and allow family to ask questions so that they are active participants in the process.
4. Review the procedure, especially its technical aspects, and insist that all personnel and equipment are immediately available. Consultation with the surgeon may prevent miscommunication about the site and extent of the operation. This should include what structures are involved in the operation and what type of cast or dressing will be applied. Evaluate the equipment in advance, making sure that it is of appropriate size for the patient and is in good operating condition. It is a good idea to practice the procedure beforehand to develop knowledge of the subtle nuances in positioning and, in the case of US, visualization of structures. Have someone familiar with the block available to assist in the performance of your first few procedures.
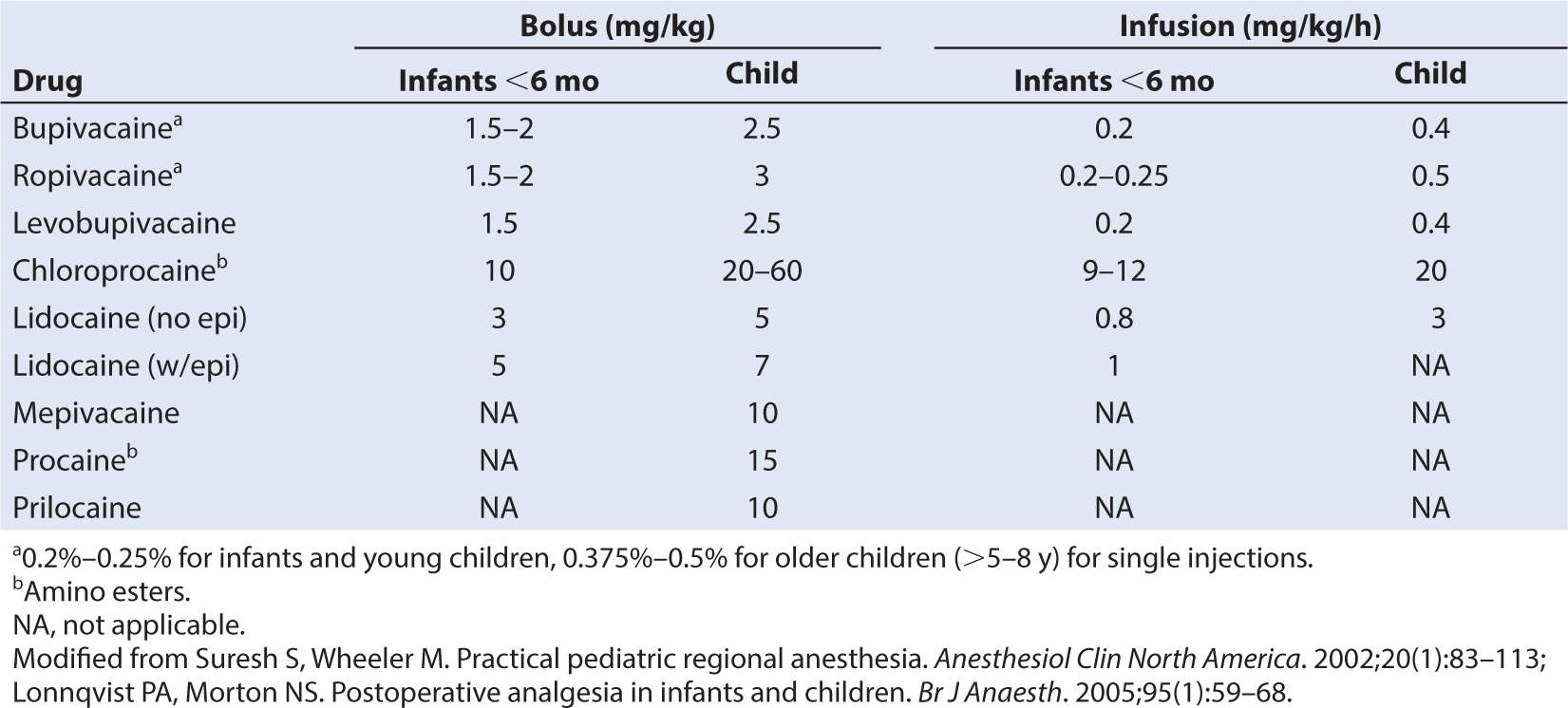
5. It is extremely important to administer the correct drug and dose. Calculating the dose and having this verified by pharmacy or a secondary source, and labeling the drugs, will minimize mistakes. Consult with the pharmacist, the literature, or an experienced colleague, especially in cases where a drug is unfamiliar to the operator. This is vital for patient safety. Check the drug and dose and the expiration date with a colleague, and label the vial or syringe when received or drawn up. Check these again before administration. (See Table 10.1 for the maximum allowable LA doses in children.) When performing multiple blocks (e.g., a sciatic and femoral block) be sure to add the total doses of drug administered in each block to determine if adjustments in LA concentration are required, and account for any LA that might be administered by the surgeon. When a particular volume per kilogram is necessary for a block, adjusting the concentration is the only way to reduce the risk of toxicity.
6. Prepare the equipment and the field early. Some blocks may require up to 30 minutes to set up, and novices might require extra time; so having a dedicated block room and other dedicated human resources is a great help to programmatic success.
7. The patient should be appropriately monitored using the same standard American Society of Anesthesiologists (ASA) monitoring guidelines used for general anesthesia.
8. Mark the patient and note any anatomical abnormalities that could influence treatment, such as pitting or blisters at the injection site. A “time out” confirmation of the patient, site, and laterality of the block should be performed with key members of the operative team present prior to the block’s placement (5).
9. Resuscitation equipment, an oxygen source, positive pressure ventilation delivery system, and suction must be immediately available.
10. Postprocedure, speak to the family about the procedure and inform them of any unexpected events. Provide them with a phone number to call for questions or problems. Follow up with the patient to detect any late complications or adverse events.
CONTRAINDICATIONS
Although regional blockade can be used safely in most infants and children, several contraindications must be remembered. These are similar to contraindications in adults.
1. The presence of infection in the region of needle placement precludes the use of a block.
2. Sepsis is a contraindication to the use of a catheter technique or central neuraxis blockade.
3. Central neuraxis blocks should also not be performed in patients with coagulopathy, thrombocytopenia, or in those who are anticoagulated.
LOCALIZATION AND TARGETING THE NERVE
There are two primary methods to determine the location of a specific nerve or nerves, both of which can increase the success and safety of regional anesthesia: US visualization and motor responses elicited with a nerve stimulator.
Fluoroscopy and CT are used only in special circumstances. Elicitation of a sensory paresthesia in the awake patient has been superseded by the techniques mentioned earlier, and is only of historical interest.
A high level of accuracy is required for localization of the nerve(s) in infants and children, due to the size of the pediatric patient. Therefore, the use of US and/or a nerve stimulator for peripheral blocks in children is highly recommended for most peripheral nerve blocks. Two meta-analyses of US versus nerve stimulation for peripheral nerve blockade concluded that US offered greater efficacy and a lower rate of vascular puncture (6,7).
A. Ultrasonography
The introduction of portable high-fidelity ultrasonographic equipment and its adoption by pediatric anesthesiologists is partly responsible for the resurgence of interest in pediatric regional anesthesia and appears to be related to the increased utilization of peripheral nerve blockade in children (8,9). Whenever possible, it should be used as the primary localizing technique for peripheral nerve blocks in children, and it has some role in neuraxial blockade as well (10).
1. Employing US has added the dimension of direct, noninvasive, real-time visualization when performing a regional anesthetic.
2. In addition to visualizing landmarks and nerves, US allows the operator to see the needle as it approaches the nerves, the injection of the LA solution, and it can be used to determine the proper positioning of a catheter.
3. Seeing the internal anatomic location of specific nerves and their surrounding structures may improve the accuracy, safety, and rate of success in performing pediatric regional anesthesia.
a. LA blocks the nerve, not the needle; the needle only needs to be near the nerve to deliver LA.
b. More rapid onset times, smaller volumes of drug, improved duration, and quality of blockade are some of the advantages that have been reported with the use of US (11–15).
c. The concern associated with performing a regional anesthetic on unconscious patients should be eased by the ability to visualize internal structures.
d. US may also identify previously unknown abnormalities or anatomic variations that are seen incidentally. However, what one does about an abnormal finding or if an abnormality is missed remains an ethical and legal question, particularly because an anesthesiologist is using the imaging for block placement and is not a diagnostic radiologist.
4. The needle may be introduced and advanced either in-plane (IP) (i.e., longitudinally oriented in the same plane with the US probe) or out of plane (oriented perpendicular to the US probe).
CLINICAL PEARL The IP approach is often easier and is most commonly used, as one can see the shaft of the needle and its trajectory, while in the out-of-plane approach one sees a transverse cut of the needle, which appears as an echogenic dot. However, there may be situations where the out of plane approach is more ergonomically advantageous to use.
B. Nerve stimulator
Nerve stimulation has mostly been supplanted by US image guidance, but it is still in use in some circumstances, primarily when US is not available. For the nerve to be stimulated, it must be depolarized. This leads to an action potential that generates a muscular contraction or a sensation.
1. Depolarization occurs more easily if the stimulator needle is negatively charged. Thus, the needle is attached to the negatively charged (cathode) lead: “N-to-N.”
2. The positively charged (anode) lead is attached to the patient: “P-to-P.”
a. The positive lead (pole) should be positioned distally along the nerve to be blocked and away from the heart.
b. Upto four times the current may be needed if the needle polarity is reversed.
3. Electrical current diminishes as a function of (1/R2), where R is the distance from the nerve.
a. The needle tip must be within a centimeter of the nerve to stimulate it, but needs to be a great deal closer to the nerve when injecting the LA for a good block to occur.
4. The nerve stimulator must have an adjustable output (0 to 10 mA) with a frequency capable of delivering 1 to 2 Hz.
a. As the needle tip approaches the nerve, the correct muscular contraction should be elicited with the minimal amperage 0.3 to −0.5 mA. Ignore direct muscle stimulation and only accept movement corresponding to the nerve that is being sought. A recent study suggests that achieving stimulation at amperage of 0.5 mA or even greater may produce equally effective blockade as lower-stimulating currents, and that refinement of needle position may be less important than generally thought (16).
b. If muscle contraction or a sensation is elicited at less than 0.3 mA, the needle is likely to be embedded in the nerve, and one should not inject. This is also true if there is a high resistance to injection; in both cases, the needle should be withdrawn immediately. Although intraneural injection has always been assumed to be a significant risk for nerve injury and has been associated with prolonged blockade, one study suggests that this is not necessarily so, and that direct intraneural injection does not always lead to injury (17). Nevertheless, intraneural injections should be assiduously avoided.
The needle should be insulated except at its very tip to improve the accuracy of localization, because this delivers maximum electrical intensity at the needle tip. This is not the case for uninsulated metal needles, where the current required for a response is higher.
1. Once the stimulated nerve is identified and needle position optimized, the drug is injected or, for continuous blocks, the catheter is passed through the needle.
2. Injection of even small volumes of LA or other fluid at this point may decrease or ablate the twitch response. This may be due to the physical movement of the nerve away from the needle caused by the injection of fluid, or to the action of the LA. Nevertheless, if one wishes to place an indwelling catheter into the nerve sheath, injection of several milliliters of fluid will dilate the sheath, making it easier for the catheter to pass.
a. Nerve stimulation is sometimes used in conjunction with US imaging, but adult studies have not demonstrated improved success or greater safety with the combination of both techniques compared with US alone.
b. In light of reports calling into question the accuracy of nerve stimulation to detect nerves, direct visualization with US may have distinct advantages over nerve stimulation (18).
TEST DOSE
LA must always be injected slowly and incrementally, with close monitoring for signs of toxicity. Test doses have been recommended to detect accidental intravascular injection of LA. Although a positive test dose is a strong indication that intravascular delivery of drug has occurred, a negative test dose is not unequivocal evidence that it has not (19). The false negative rate is unknown, but observational reports confirm that it is not zero (20). Nevertheless, the authors recommend administering a test dose of LA containing 5 µg per mL of epinephrine (0.1 mL/kg, maximum of 3 mL) to assist in detecting inadvertent intravascular injections when performing blocks requiring large volumes or doses, especially with epidural or caudal blocks. The direct visualization of LA injection with US may be an effective substitute for the test dose, but confirmatory data are lacking.
CLINICAL PEARL Single-injection caudal blocks appear to have the highest rate of accidental intravascular injection, while peripheral nerve blocks may have the lowest.
1. During general anesthesia, one cannot rely on heart rate response alone as an indicator of a positive intravascular test dose (21).
a. Although in the awake patient a rise in heart rate of 10 beats per minute or greater is a sensitive positive sign for intravascular injection, heart rate will not increase after an intravascular test dose injection in approximately one-fourth of anesthetized children.
2. A more sensitive indicator that should always be sought is a change in T-wave amplitude on electrocardiogram (ECG) (22) (Fig. 8.1).
a. T-wave height will increase substantially within 20 seconds of injection, and the effect may disappear within 60 seconds.
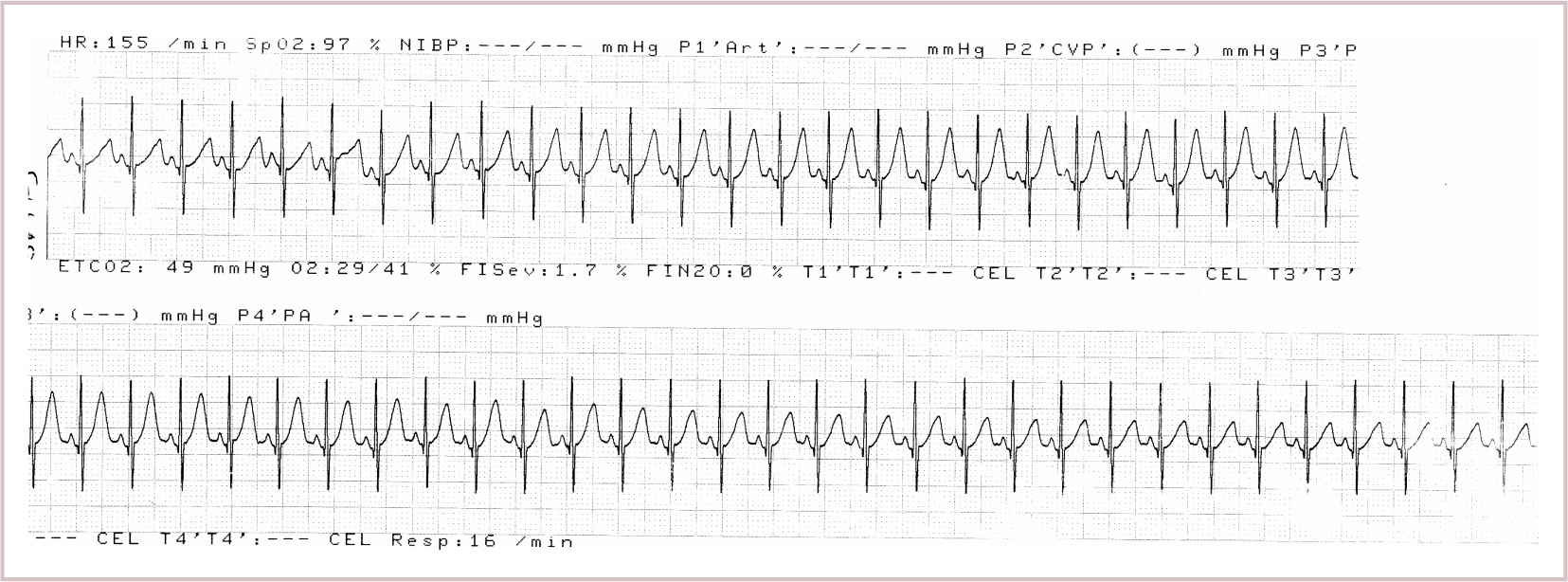
FIGURE 8.1 Elevation of t-waves following an intravascular injection of a test dose of bupivacaine with 1:200,000 epinephrine. Note the short duration of the ECG changes.
3. The type of anesthetic agent that the child is receiving will affect the results and reliability of the heart rate and ECG response to the test dose.
a. Halothane decreases the reliability of the test dose more than sevoflurane (23,24).
b. Atropine (0.010 mg /kg) improves the results of the test dose in the presence of halothane but not sevoflurane (21).
c. T-wave change is a highly reliable indicator with any type of inhalation anesthesia.
d. Intravascular injection during total intravenous anesthesia with propofol and remifentanil does not reliably change T-wave morphology or heart rate, and changes in blood pressure must be sought as an indicator instead (25).
LA TOXICITY
The toxic side effects from LAs, particularly the amides, can be life threatening (Table 8.1).
1. The ability to metabolize esters matures early in childhood; therefore, the ester LAs do not pose the same toxicity risk as amide LAs.
2. Accidental intravascular injection, excessive absorption, and excessive dosing are the most common causes of toxicity.
3. Cardiovascular collapse and central nervous system toxicity are associated with the intravascular injection of highly protein-bound, long-acting amide LAs.
a. Inhibition of ion channel function by the LAs causes the most severe clinical symptomatology, most importantly affecting the heart and the brain.
b. In the heart, the cardiac pacemaker cells, the cardiac muscle cells, and the cells of the cardiac conduction system can be profoundly affected by LAs.
c. Inhibition of sodium channel conductance in these cells diminishes the maximum rate of increase of the cardiac action potential; that is, the rate of depolarization is slowed.
d. The amides have a preference for open ion channels; so they exert more effect on cardiac cells during the rapid repolarization that occurs in phase 1 of the cardiac cycle.
4. The higher heart rates of children may predispose them to the perils of LA toxicity. Widening of the QRS complex, lengthening of the PR interval, early afterdepolarizations, decreased cardiac contractility, and torsades de pointe are all recognized manifestations of toxic levels of the amide LAs.
Sedation or general anesthesia can mask the early warning signs of LA toxicity in children.
1. In older, verbal, pediatric patients who are awake, restlessness, lightheadedness, muscle twitching, headache, irritability, metallic taste, perioral numbness, dysarthria, tinnitus, and fatigue can be elicited or observed.
2. With younger, preverbal children, signs of LA toxicity are not as easily discerned. Agitation, irritability, and restlessness can be mistaken for pain and treated with bolus doses of drug or infusion increases, thereby exposing the child to more drugs.
3. Although studies appear to suggest that at least in adults, high systemic levels of ropivacaine are better tolerated than bupivacaine, the data for children are lacking.
4. Animal studies suggest that the levoenantiomers have a 30% increase in safety as compared with racemic LAs.
5. Seizures, cardiac arrest, and death from LA toxicity are rare events but are also probably under reported.
Treatment of LA toxicity with lipid rescue promises dramatically improved effectiveness and outcomes compared with earlier therapies (26).
1. A variety of treatment options, including the administration of midazolam, phenytoin, clonidine, lidocaine, and amrinone, have been suggested in the past. These have all now been superseded by the use of lipid emulsion. Although there are extensive animal data, and robust anecdotal human data, lipid rescue therapy has not been subjected to rigorous investigation in humans due to obvious concerns about patient safety (27).
a. Securing the airway and stopping the administration of the inciting drug are the first steps necessary to treat LA toxicity.
b. Additional personnel should be sought to assist in the resuscitation.
c. Standard cardiopulmonary resuscitation measures should be started immediately if cardiac arrest or inadequate perfusion is present. The use of only low doses of epinephrine, if needed, is recommended; amiodarone is the preferred anti-arrhythmic. High doses of epinephrine and vasopressin have been associated with poor outcome compared with lipid rescue (28,29).
d. Seizures should be treated with a benzodiazepine.
e. A 20% intravenous lipid emulsion should be administered immediately at the first sign of LA toxicity (30).
i. This appears to be the most important advance in the treatment of LA cardiac toxicity (31,32).
ii. The lipid partitions, scavenges, extracts, and binds lipophilic LAs from tissue and plasma (33).
iii. The current recommended dose is 1.5 mL per kg over 3 minutes, repeated as needed up to 3 mL per kg, followed by an infusion of 0.25 mL/kg/minute until hemodynamic stability is achieved.
iv. Prolonged resuscitative efforts may be needed with the longer-acting LAs.
v. The infusion rate can be increased as needed to 0.5mL/kg/minute; however, a maximum rate of 10 mL per kg over 30 minutes should not be exceeded, nor is more likely to be effective.
vi. One must not use propofol instead of the lipid emulsion because of the negative cardiovascular properties of the drug coupled with its lower lipid content (34).
2. A good working knowledge of the anatomy and physiology of the patient, fractionation of loading doses, and slow administration of LA, along with the appropriate equipment and dosing, will increase the margin of safety for these drugs and procedures.
CLINICAL PEARL Any patient care location where regional anesthetics are administered should have a LA toxicity kit containing a supply of 20% intravenous lipid emulsion so that therapy can be promptly initiated.
OPIOIDS AND ADJUNCTIVE AGENTS
The administration of opioids, either alone or in combination with LAs through the caudal, epidural, or spinal routes, has been shown to produce striking postoperative analgesia.
1. The close proximity of the opioid receptors in the spinal cord to the subarachnoid space and the epidural space allows for the administration of much smaller doses of drug to achieve an analgesic effect.
2. The advantage of epidural or intrathecal opioids used alone is that they can produce profound analgesia while preserving motor function, touch, and hemodynamic stability.
3. Side effects include respiratory depression, pruritus, nausea and vomiting, and urinary retention. These can be effectively treated with low doses of opioid antagonists or mixed agonist antagonists, and some authors have reported success with 5-HT blockers for pruritus (35,36).
4. Intrathecal morphine produces long-lasting analgesia.
a. Injection can be performed through lumbar puncture, or, during posterior spinal fusion surgery, can be administered by the surgeon under direct vision.
b. Because of the cephalad spread of the hydrophilic opioids, respiratory depression is a risk that requires careful postoperative monitoring (37).
c. A morphine dose of 5 to 7 µg per kg is usually used, approximately one-tenth to one-fifth of the epidural dose. This will provide 10 to 18 hours of analgesia.
5. Epidural morphine is most commonly used as a single injected dose, due to its long duration of action in the central neuraxial space (38).
a. Although a wide range of morphine doses, up to 100 µg per kg, have been used, higher doses are associated with more respiratory depression and other side effects, and the optimal balance between side effects and duration of action has been reported as 33 µg per kg (39). This produces approximately 8 hours of analgesia.
b. Other epidural opioids are not used as commonly as single-injection agents due to relatively short durations of action and are favored for infusion. This is discussed in detail in Chapter 10 on pain management.
Clonidine has been used as an adjunctive agent for epidural and caudal blockade.
1. Most studies have found that it doubles the duration of analgesia compared with LA alone (8 vs. 3.9 hours with a single caudal injection) (40,41). This appears to be because of local action on the spinal cord (42).
2. A dose of 1 µg per kg is most commonly recommended. Clonidine has the potential to cause hypotension or sedation, but does not produce pruritus or urinary retention. Larger doses may produce respiratory depression in infants (43).
3. Clonidine has also been studied as a single agent in comparison to a combination regimen with LAs and found to have comparable efficacy to neuraxial opioids following major abdominal and thoracic surgery in children (44).
Ketamine, midazolam, neostigmine, dexmedetomidine, dexamethasone, and other agents have been used as adjunctive agents. Nevertheless, with the possible exception of preservative-free ketamine (not yet available in the US) and dexamethasone in peripheral nerve blocks, we cannot recommend their routine use in regional anesthetics until further animal and human studies are performed to exclude the possibility of neurotoxicity. Continued use of epinephrine to increase the duration of a single shot block and bicarbonate to speed onset in peripheral blocks is warranted, and preservative-free dexamethasone appears to have safety and efficacy in prolonging peripheral block duration (45). A recent randomized and blinded study, however, found that intravenous and perineural dexamethasone have equal efficacy in prolonging block duration (46).
SAFETY AND COMPLICATIONS
There are prospective data from several large collaborative studies that demonstrate the high level of safety of regional anesthetics in infants and children. The British National Pediatric Epidural Audit (2007), a prospective analysis of 10,633 cases over 5 years, found a low rate of complications (47). The investigators noted only one case of persistent injury after 1 year of follow-up, a cauda equina syndrome that developed after a drug dosing error. There were 3 deep infections and 25 superficial infections, emphasizing the need for strict aseptic technique and careful monitoring of the catheter site. Pressure sores developed in 33 children; strict attention to positioning and nursing care is mandatory if any degree of motor blockade is present with any kind of regional block. The two prospective studies of the French Language Society of Pediatric Anesthesia (ADARPEF) were conducted over 2005 to 2006 and 1993 to 1994, and together comprise nearly 55,000 regional blocks (48,49). They detected no serious complications and no sequelae, and noted that the overall incidence of adverse events was 0.12%. Significantly, the complication rate was six times higher in neuraxial blocks compared with peripheral nerve blocks. The Pediatric Regional Anesthesia Network (PRAN) has published several observational studies from their prospective multicenter database. In the initial study of nearly 15,000 blocks of all kinds, complication rates were found to be similar to those in the European studies, and no serious adverse events were noted (50). PRAN also performed the first prospective analysis of the safety of regional blocks under general anesthesia from a cohort of 53,564 blocks, which showed that regional blocks performed under general anesthesia were at least as safe as when performed in awake children, and that the risk of neurologic symptoms was seven times higher for children who were awake or sedated than those who were anesthetized (51). No long-term sequelae were noted in any subject. Additional studies from PRAN have looked at caudal and transversus abdominis plane (TAP) blocks, with similar findings of safety (52,53).
These multicenter prospective studies demonstrate a remarkably low incidence of adverse events and complications, but despite the large numbers of subjects, one cannot infer that regional anesthesia in children is without risk. Rare catastrophic events, often of unknown etiology, can indeed occur and have been reported by highly experienced pediatric anesthesiologists employing the most careful and meticulous techniques (54,55).
UPPER EXTREMITY BLOCKS
These blocks provide an excellent means of delivering high-quality pain relief. A successful block can decrease a patient’s opiate requirement and provide immobility to the extremity if needed. Patients who have upper extremity surgery or fractures, who require reimplantations, or who are in need of increased blood flow to an upper extremity may benefit from one of these blocks. They have also been used in the treatment of complex regional pain syndrome (CRPS) of the upper extremity. Note that the recommended volumes of LA are largely based on reports using nerve stimulation, and that with US guidance considerable reductions of these values (between 30% and 50% less in some studies) may be possible (12,56,57). Large pediatric series with strong confirmatory data, showing the need for less LA for regional blocks under US in children are unfortunately limited.
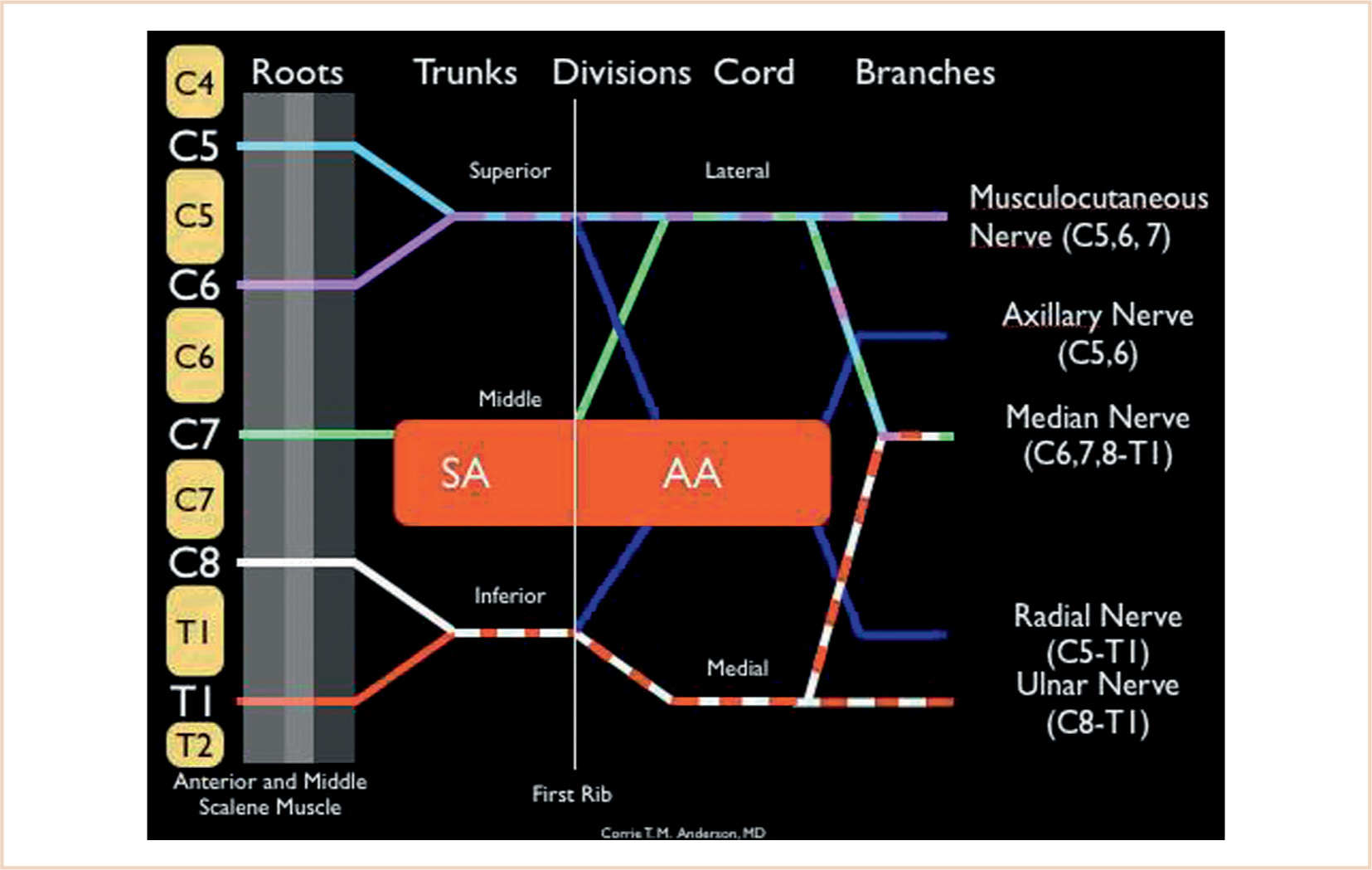
1. Branches of the brachial plexus innervate the upper extremity (see Table 8.2). It is formed by the anterior portions of the C5-T1 nerve roots; in a smaller segment of the population, the C4 and T2 roots also contribute to the brachial plexus. The dermatomal distribution of these nerve roots is mapped in Figure 8.2. The plexus undergoes a number of divisions that ultimately generate terminal nerves supplying sensory and motor innervation to the upper extremity (see Fig. 8.2).
2. Blocks along the entire aspect of the brachial plexus and from a number of different anatomic approaches have been described (Fig. 8.3). In cases where there is an inadequate neurologic examination, especially following trauma or where assessment of neurologic function is essential, an alternative technique of pain relief might be considered.
INTERSCALENE BLOCK
This block is indicated for surgery of the shoulder, upper arm, on the lateral aspect of the humerus, and of the forearm. Movement of the wrist and fingers with the nerve stimulator heralds a successful interscalene block. In up to 50% of the cases, the ulnar nerve is missed (Fig. 8.4).
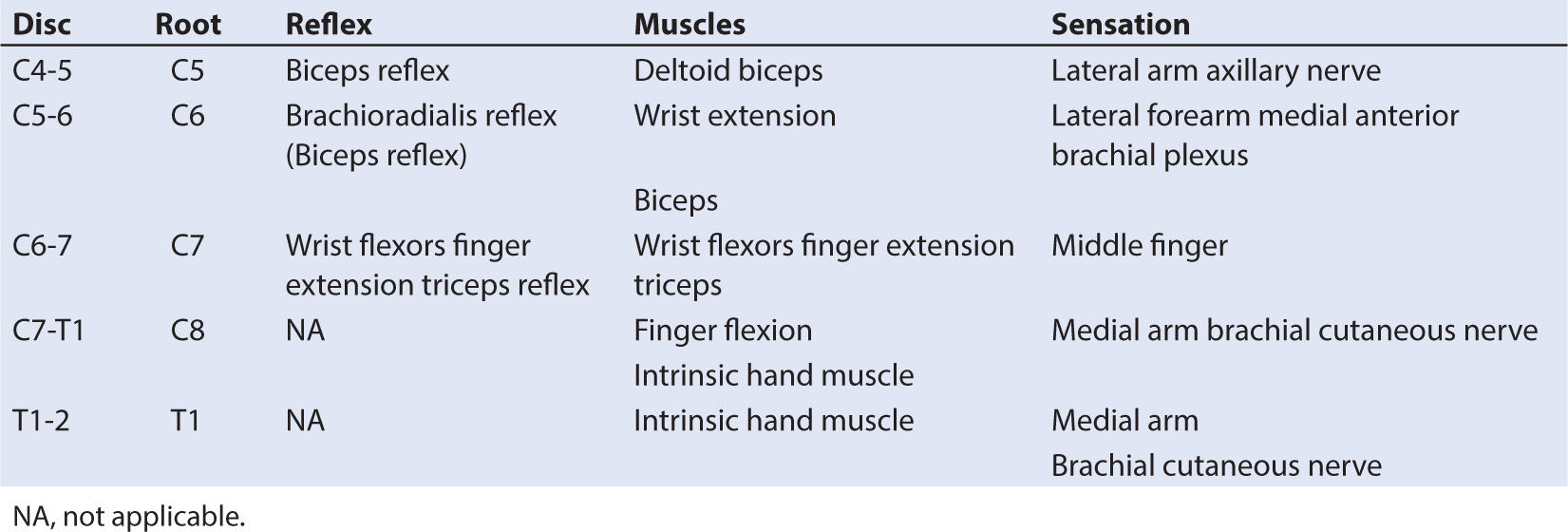
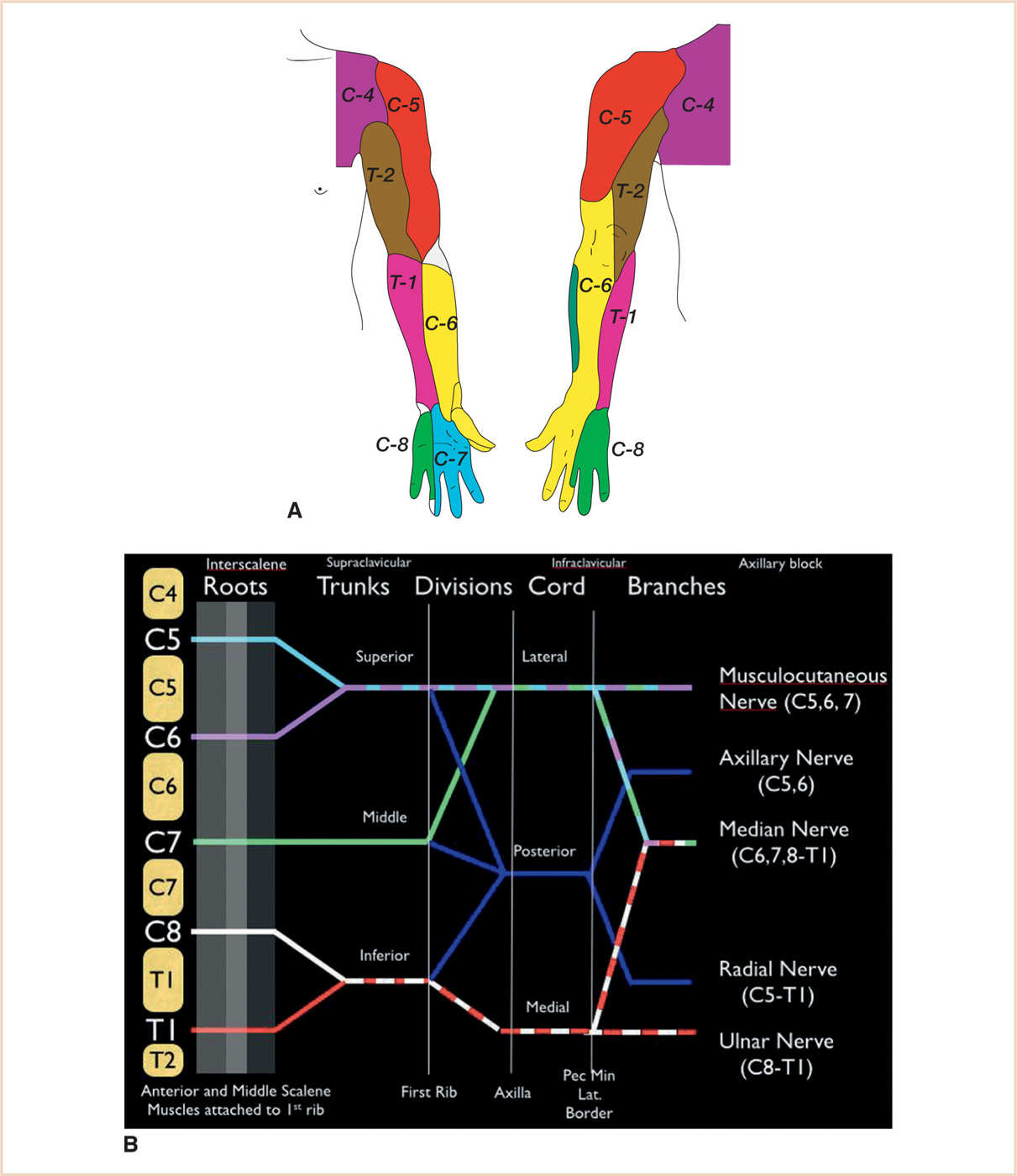
FIGURE 8.2 A: Sensory dermatomes of the upper extremity. B: Brachial plexus with subdivisions and terminal branches. The labels at the top of the figure, interscalene, supraclavicular, infraclavicular and axillary refer to specific regional anesthetic blocks and where they are performed along the brachial plexus.
1. For surgery on the proximal shoulder, the addition of a superficial cervical plexus block and an accessory nerve block will provide better pain relief. Separate T1-2 blockade may be needed for anterior incisions of the shoulder, and supplemental blockade of the ulnar nerve may be needed since this nerve is spared in up to 50% of cases.
2. Adult data shows that this block produces partial or complete phrenic nerve block and hemidiaphragmatic paresis in almost all cases, so many experts suggest that it not be performed in patients with respiratory compromise and should never be performed bilaterally (58). The incidence of hemidiaphragmatic weakness in children appears to be less than in adults, but caution is still warranted, especially in young children. Diaphragmatic paresis can also be reduced by using lower volumes of LA, which can be facilitated by US guidance (59,60).
a. The anterior body of the sternocleidomastoid muscle (SCM) is palpated with the head turned partly to the side (see Fig. 8.5).
b. The interscalene groove can be felt just posterior to the muscle in the posterior cervical triangle, medial, and cephalad to the midpoint of the clavicle.
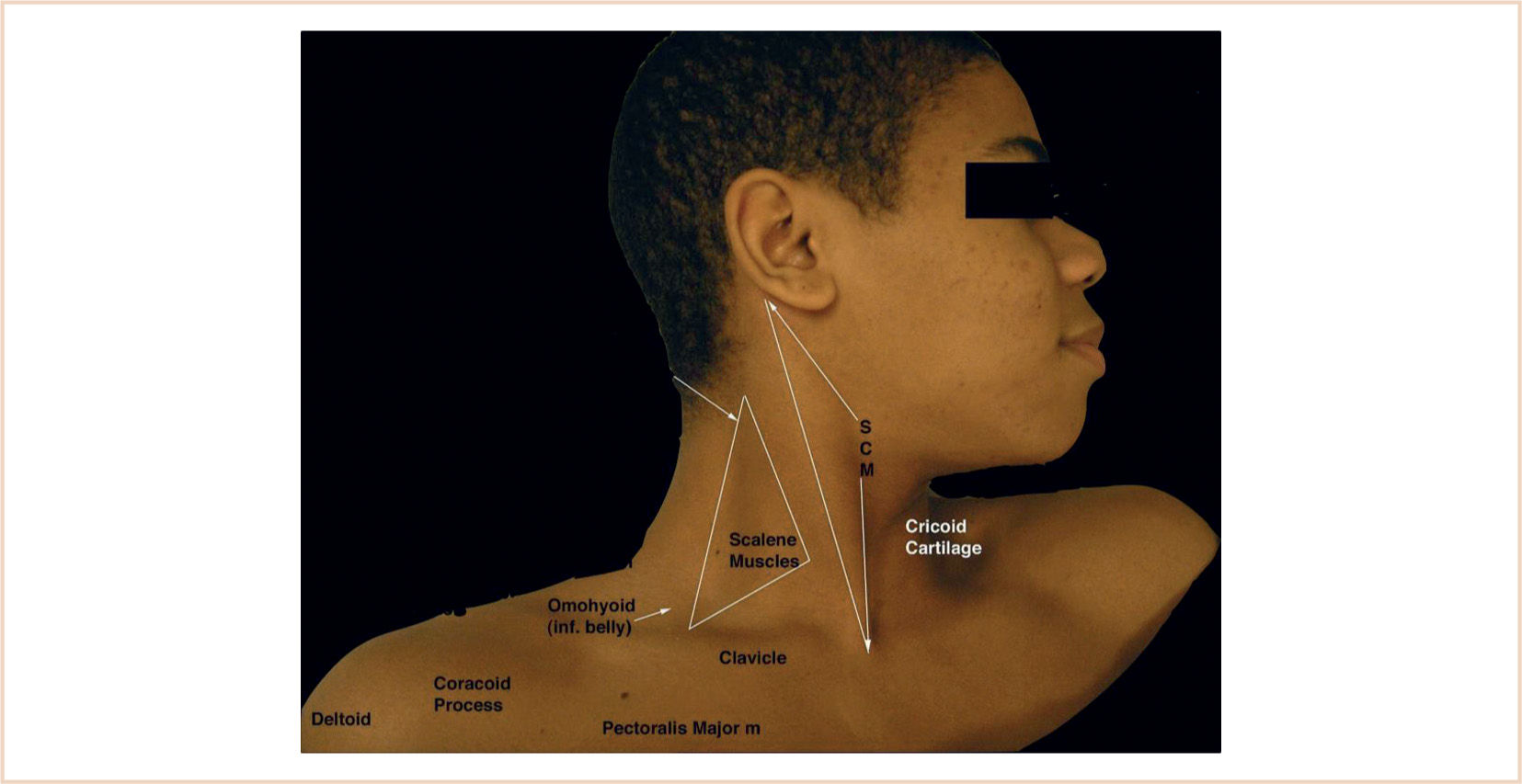

FIGURE 8.5 The sternocleidomastoid muscle (SCM) and the surface anatomy of the neck for interscalene block. Inf, inferior; m, muscle.
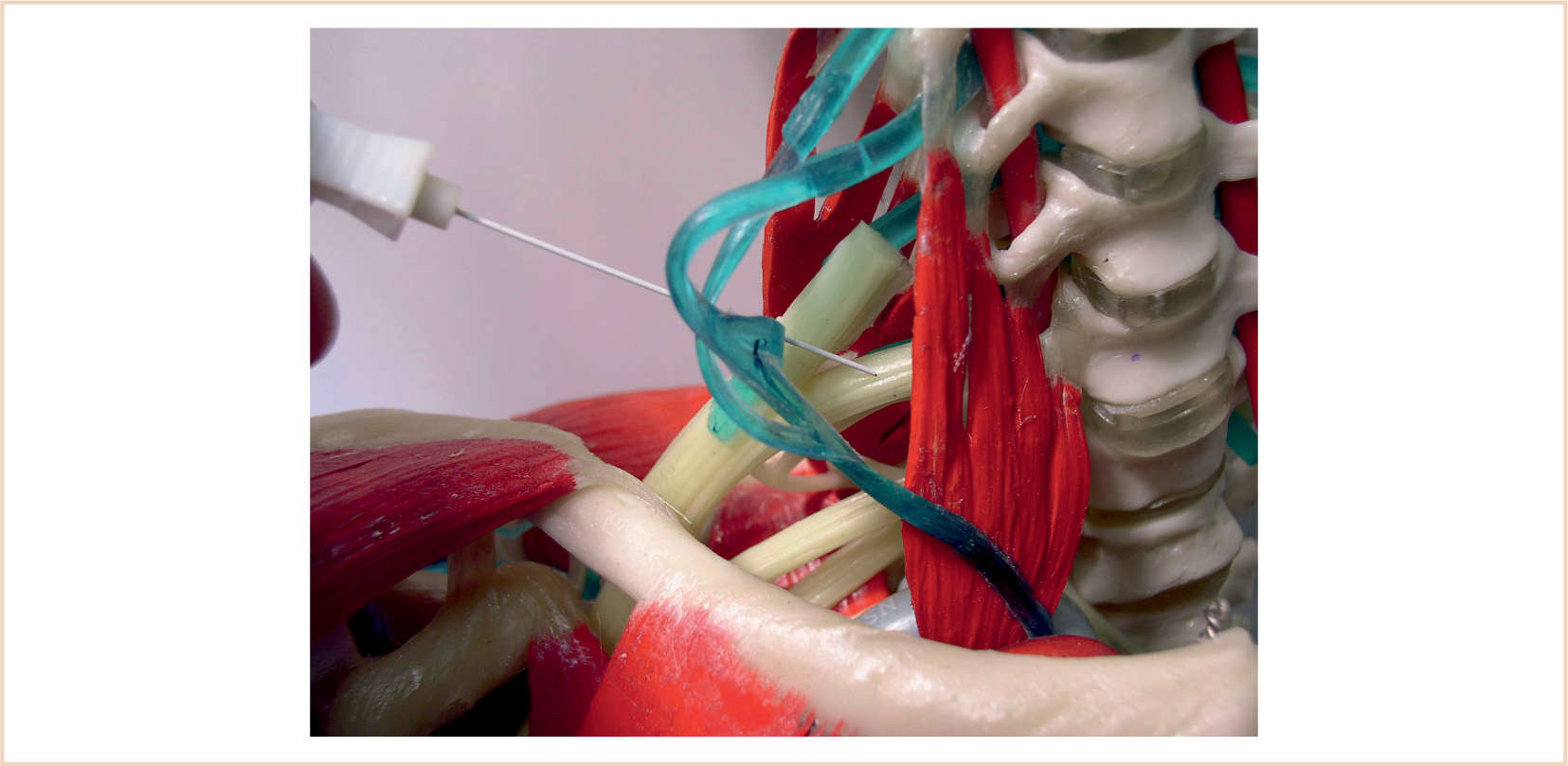
c. A 22-gauge 1-in. needle (insulated if nerve stimulation is employed) attached to a short length of extension tubing is used. The needle is inserted IP along the long axis of the probe approximately at the C6 level (see Fig. 8.6).
d. With US, the subclavian artery and the brachial plexus are seen in cross section. The trunks of the brachial plexus are aligned in a linear manner and appear round and hyperechoic with the appearance of a string of pearls (see Fig. 8.7).
e. If nerve stimulation is used, the nerve stimulator is set at 0.5 mA; the needle is inserted perpendicular to the skin and advanced until motor paresthesias are elicited in the distribution of the radial, ulnar, or median nerves. Refinement of the needle position is sought so that the stimulating current can be reduced to 0.3 mA.
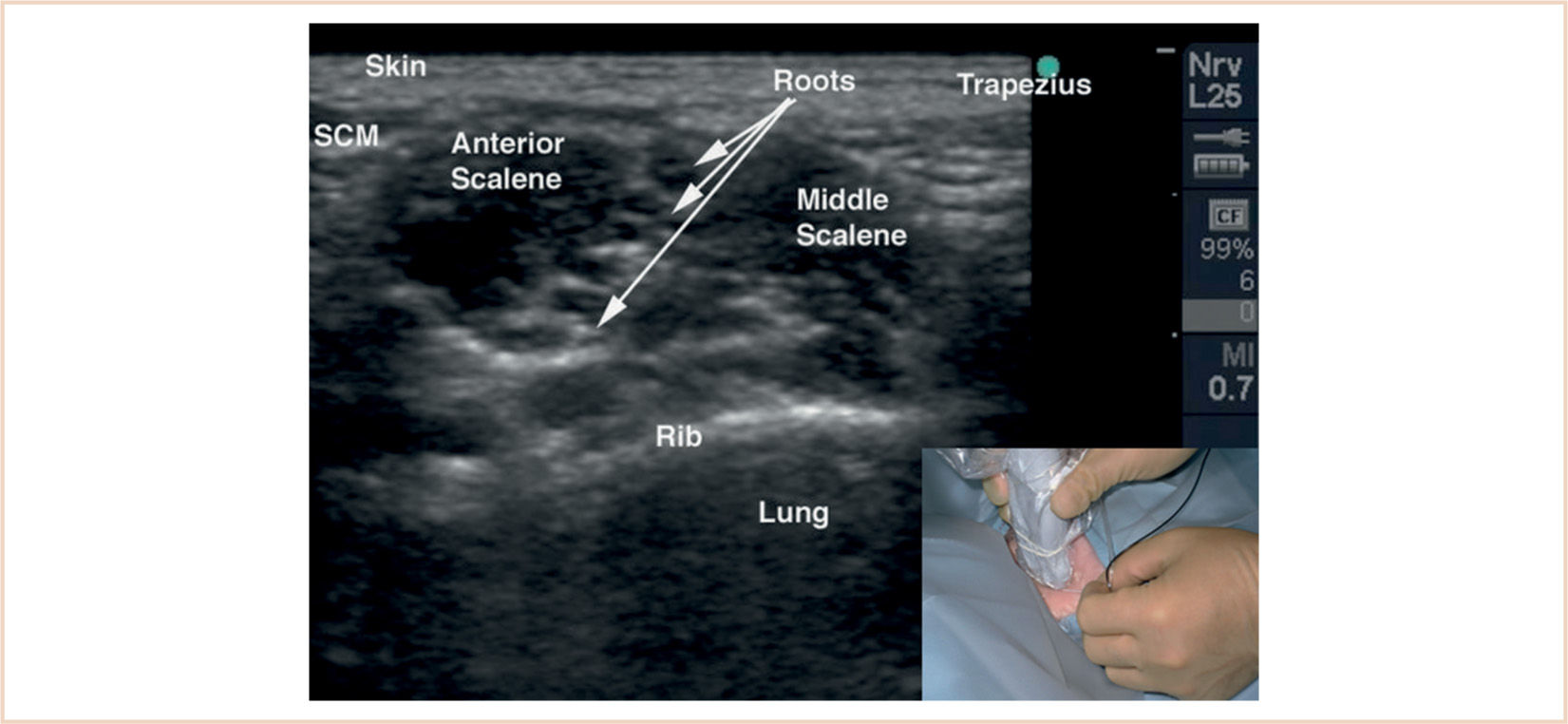
FIGURE 8.7 US imaging of the interscalene view of the brachial plexus. The nerves of the brachial plexus are aligned in a linear fashion between the anterior and middle scalene muscles.
f. As with all regional blocks, incremental injection and frequent aspiration are used to avoid intravascular injection.
g. Resistance to injection (or stimulator threshold less than 0.3 mA when a nerve stimulator is used) may be a sign of intraneural needle placement; in such a case, injection should immediately stop and the needle must be repositioned.
h. A superficial cervical plexus block may be performed with subcutaneous injection of 1 to 2 mL of LA perpendicular to the SCM to provide broader coverage.
i. A catheter can be placed for continuous infusion of LA for prolonged analgesia.
j. In addition to the usual complications of regional blockade, potential complications of this block include pneumothorax, subdural, epidural and subarachnoid puncture, recurrent laryngeal nerve blockade, Horner syndrome, and vagal and phrenic nerve blockade.
SUPRACLAVICULAR BLOCK
This block, which is indicated for almost all procedures on the arm and hand, was once rarely performed in the pediatric population because of the risk of causing a pneumothorax. The most recent data show that this is now the most commonly performed upper extremity block in children (49,50). Its popularity has increased because of the growing use of US. There is a higher risk of pneumothorax, limb ischemia, and vascular penetration but a lesser chance of a high spinal, dural puncture, and vertebral artery cannulation compared with the interscalene approach.
CLINICAL PEARL US guidance is greatly preferred for this block, as it increases safety and efficacy, and may permit the use of lower volumes of LA. Although nerve stimulation can be used, an axillary approach should be considered if US is not available.







Full access? Get Clinical Tree


