FIG. 25.1 Vertebral anatomy. A, Sagittal view. B, Oblique view of the lumbar vertebrae showing the ligamentum flavum thickening in the caudad extent of the intervertebral space and in the midline. (From Miller RD, et al.: Miller’s anesthesia, ed 8, Philadelphia, PA, 2015, Elsevier.)
Thirty-one pairs of spinal nerves travel from the spinal cord and exit at their respective intervertebral foramina (C1-S5). There are 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal pair of spinal nerves. These nerves are blocked by the local anesthetic medication to produce anesthesia or analgesia. Spinal nerve roots vary in size and can be divided into dorsal roots (primarily sensory) and anterior roots (primarily motor).5,8,9
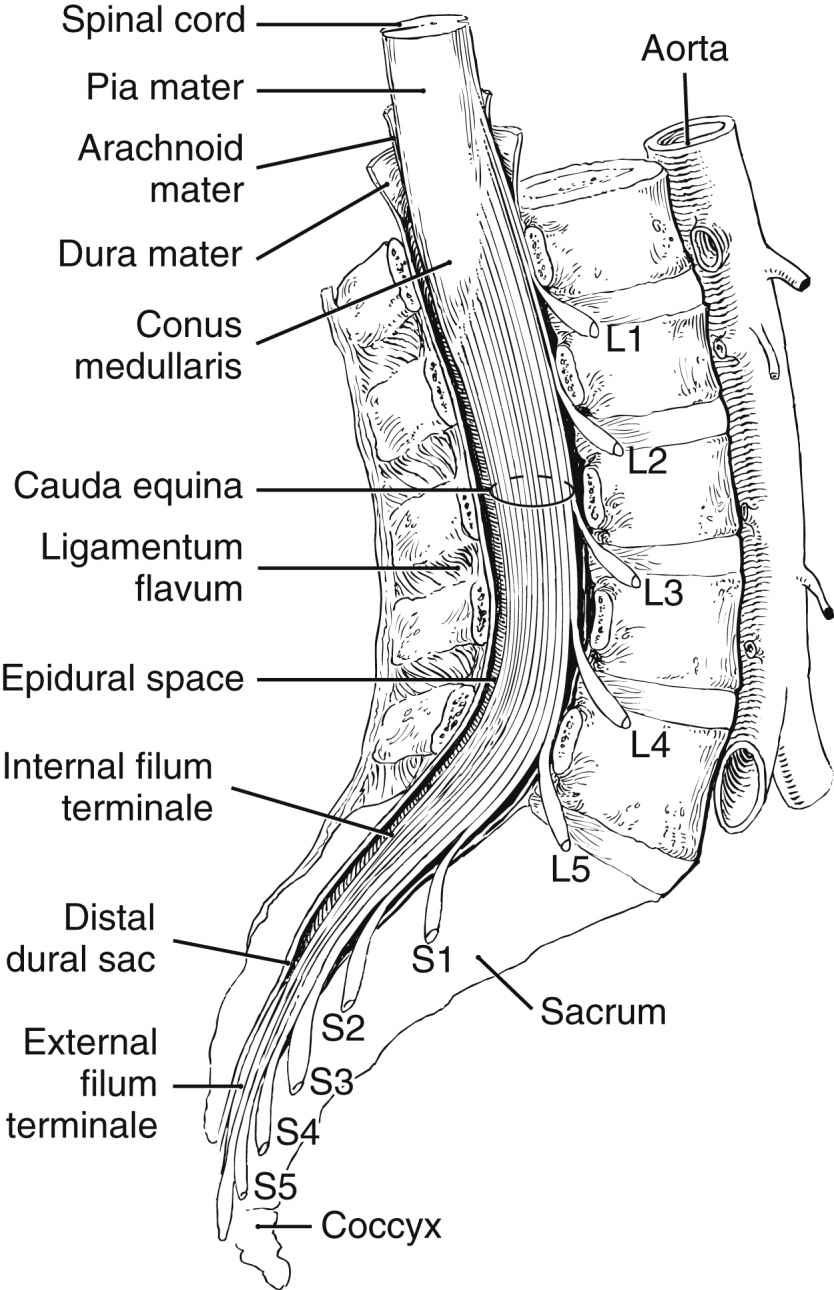
FIG. 25.2 Extension of the spinal cord to the second lumbar vertebra. (From Nagelhout JJ, Elisha S: Nurse Anesthesia, ed 6, St. Louis, MO, 2017, Elsevier.)
Spinal Versus Epidural Blocks
Spinal and epidural blocks are neuraxial blocks. Both block spinal nerve roots, and the site of administration differs as does the mechanism of action (Table 25.1). A spinal anesthetic blocks spinal nerve roots as they pass through the CSF, resulting in blockade of sensory, motor, and autonomic impulse transmission, whereas epidural anesthesia and analgesia block spinal nerve roots outside the subarachnoid space. Epidurals require a large dose of local anesthetic to allow for diffusion through anatomic barriers, such as the dura, and spreads horizontally and vertically within the epidural space. The epidural space is vascular, and there is a risk of local anesthetic toxicity (see Chapter 24). Spinal anesthesia is accomplished by administering a small dose of local anesthetic within the subarachnoid space. Spinal anesthesia is a single injection through a needle that reduces the time for administration but does not allow for repeated dosing. Epidural anesthesia is administered through a catheter placed through a needle and may require more time to place, may be dosed again, and may be used for postoperative analgesia. Spinal anesthesia is limited to placement in the lower lumbar region below the termination of the spinal cord. Epidural catheter placement can occur in the lumbar or thoracic region. Spinal anesthesia is rapidly achieved and produces an intense sensory and motor block. Rapid onset can lead to profound hypotension. Epidural anesthesia onset is gradual, blockade is less profound, and decreases in blood pressure are less intense.7,9
Table 25.1
Differences Between Spinal and Epidural Anesthesia
| Spinal | Epidural | |
| Site or mechanism of action | Nerve roots blocked as they pass through the CSF | Nerve roots blocked outside the cerebrospinal fluid |
| Site of administration | Lower lumbar below the termination of spinal cord | Lumbar or thoracic area |
| Dose of local anesthetic | Small | Large |
| Instrument for administration | Needle | Catheter |
| Ability to repeat dose | No | Yes |
| Onset | Rapid, intense blockade, may lead to hypotension | Gradual; may have less intense blockade, decrease in blood pressure is more gradual |
Contraindications
Absolute contraindications include patient refusal, cardiovascular diseases such as severe aortic–mitral stenosis and asymmetric septal hypertrophy, severe uncorrected hypovolemia, documented allergy to local anesthetic, increased intracranial pressure, infection at the site of injection, sepsis or bacteremia, and coagulopathy.1,5,7,9 Coagulation-altering medications should be reviewed and current recommendations should be followed to avoid the potentially catastrophic complication of a neuraxial hematoma.10 Current guidelines related to anticoagulation therapy and regional anesthesia can be accessed and reviewed at http://asra.com/publications-anticoagulation-3rd-edition-2010.php.10–12 Relative contraindications include preexisting neurologic disease, musculoskeletal abnormalities, prior back surgery, and untreated hypertension.1,5,7,9 Placing a neuraxial block through a tattoo is controversial.13 The perianesthesia nurse should alert the anesthesia provider to potential contraindications.
Spinal Anesthesia
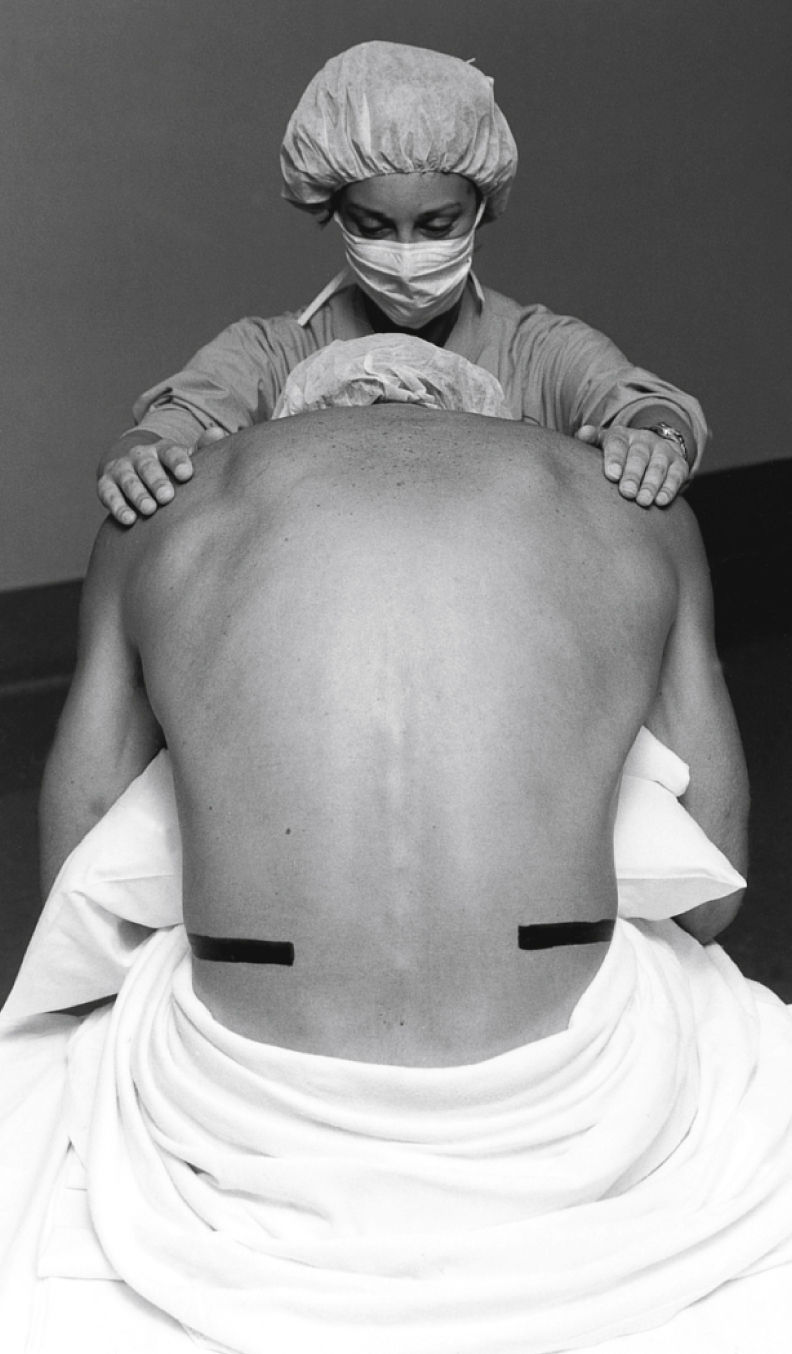
Universal protocol, as outlined by The Joint Commission, should be followed, and medications should be labeled before the procedure.14 An initial set of vital signs should be documented. Patients may be positioned in a lateral decubitus or sitting position with the back flexed to maximize the intervertebral opening (Figs. 25.3 and 25.4). Tuffier’s line is generally used to identify the third and fourth lumbar spaces but may not always be reliable.15 After the anesthesia provider has identified the desired interspace, he or she will follow sterile technique (mask, sterile gloves, hat) and proceed with preparing and placing sterile drapes. The perianesthesia nurse should maintain verbal contact with the patient to reassure and inform him or her of what to expect. Local anesthetic is used to anesthetize the skin and underlying tissue. A 25-gauge or smaller spinal needle is used in patients at risk for a post–dural puncture headache (PDPH): patients younger than 50 years, females, those who are pregnant, and those with a prior history of PDPH. Needle design is an important consideration in at-risk groups, with pencil-point needles being less likely to cause a PDPH.1,16 The spinal needle will transverse the supraspinous and interspinous ligaments, ligamentum flavum, and dura; this is noted by a change in the resistance. The stylet is removed and CSF is noted at the hub of the needle. Procaine, bupivacaine, or tetracaine are commonly used for spinal anesthesia. Epinephrine (0.1 to 0.2 mg) or phenylephrine (2 to 5 mg) can be added to increase duration of action. Small doses of opiates are commonly used to augment analgesia.9 Local anesthetic is administered, and the patient is positioned. Vital signs should be monitored at 1-minute intervals for the first 10 minutes and then, if stable, every 5 minutes. Blood pressure decreases of 20% or more should be treated with fluids and vasopressors (ephedrine or phenylephrine).1,5,7,9
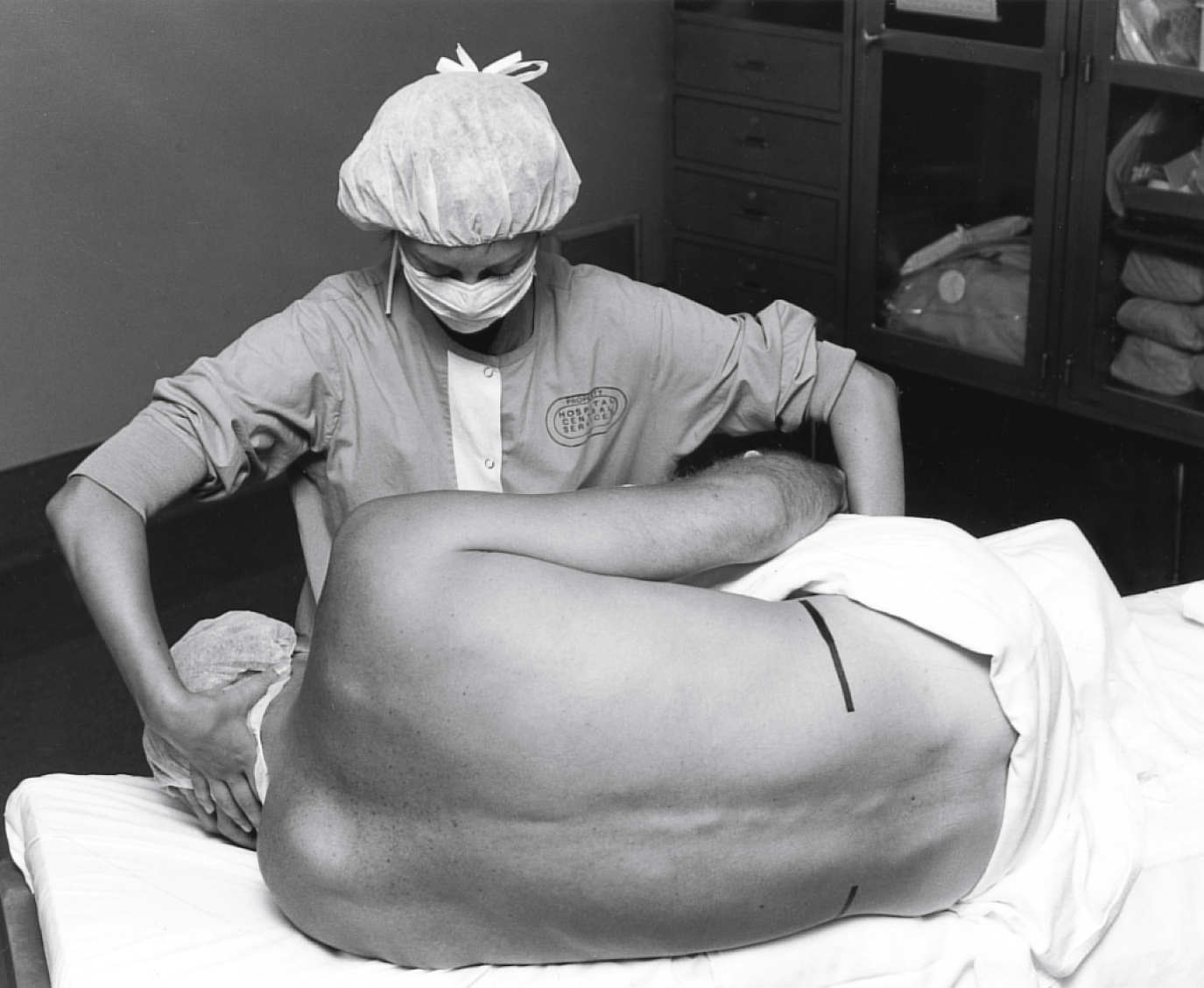
FIG. 25.3 Lateral decubitus positioning for a neuraxial block. The assistant can help the patient assume the ideal position of “forehead to knees.” (From Miller RD, et al.: Miller’s anesthesia, ed 7, Philadelphia, PA, 2009, Elsevier.)
Progression of onset is noted by loss of autonomic or sympathetic function, sense of temperature, pain, touch, movement, and proprioception. During recovery, function will return in the opposite order (Box 25.1). Spinal anesthetics are dosed for specific surgical procedures (Table 25.2). Level of anesthesia is monitored by dermatome level (Fig. 25.5). Monitoring regression of spinal anesthetic is aided with the knowledge of the dermatome level and can be assessed by the use of an alcohol wipe, a blunt needle that does not break the skin, something cold such as a small piece of ice, or a light pinch.5,6
Epidural Anesthesia
Epidural anesthesia or analgesia is similar to spinal anesthesia with regard to positioning, sterile technique, monitoring, progression, and assessment. Epidural anesthesia can be a single-shot technique (i.e., caudal anesthesia) or more commonly as an intermittent or continuous technique for anesthesia or analgesia. Anesthesia may be administered for the same types of surgical procedures as spinal anesthetics (see Table 25.2) but may be less effective for procedures of the perineum because of sacral sparing. Epidurals are versatile for analgesic purposes and may be used for labor and delivery or postoperative analgesia for surgical procedures ranging from the thorax to lower extremities. Epidural needles are larger than spinal needles to allow for the insertion of a catheter. The average needle is 9 cm and marked to indicate the depth of insertion. An epidural needle transverses the supraspinous and intraspinous ligament and is seated in the ligamentum flavum. A special loss-of-resistance syringe with preservative-free saline is attached to the hub, and the needle is advanced until a loss of resistance is noted upon entering the epidural space. An epidural catheter is then inserted to a desired depth. Epidural catheters are marked to indicate the depth of insertion.1,5,7,9,16,17 A 3-mL test dose of 1.5% lidocaine with 1:200,000 epinephrine is administered to help detect intravascular, subarachnoid, or subdural placement. If positive, the heart rate and systolic blood pressure will increase by at least 20 beats/min and 15 mm Hg but may not be reliable in the presence of beta-blockers, advanced age, and general anesthesia.9 A subarachnoid injection will result in a spinal anesthetic, whereas a subdural injection can result in an extensive block relative to a small dose of local anesthetic.18 Common local anesthetics used for epidural anesthesia include 2-chloroprocaine, lidocaine, bupivacaine, and ropivacaine. Epidurals are dosed based on the number of dermatomes to be blocked (1 to 2 mL per dermatome). Dosing occurs slowly, with no more than 5 mL of local anesthetic administered at a time because there is a risk of local anesthetic toxicity. Epinephrine (1:200,000) can be used to decrease absorption and prolong duration. Epidural catheters should be monitored for signs of drainage or dislodgment. The site is covered with a sterile dressing, and connections should be tight. The American Society of PeriAnesthesia Nurses’ position statement on safe medication administration19 and local institutional policy should be followed for the administration of medications. When initiating a continuous infusion, check dose and concentration of local anesthetic solution, and confirm the infusion rate.
Table 25.2
Dermatome Level and Surgical Procedure
| Sensory Level | Surgical Procedure | Cutaneous Level |
| Above T4 | Pinky, inner arm, apex of axilla | |
| T4 | Cesarean section, upper abdomen, uterine | Nipple |
| T6-7 | Lower abdomen | Xiphoid |
| T7-8 | Tourniquet pain | |
| T10 | Hip and genitourinary | Umbilicus |
| L1-3 | Lower extremities | |
| S2-5 | Perineal region (genitalia/buttocks) |
Modified from Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, phase I and phase II PACU nursing, ed 3, St. Louis, MO, 2015, Elsevier.
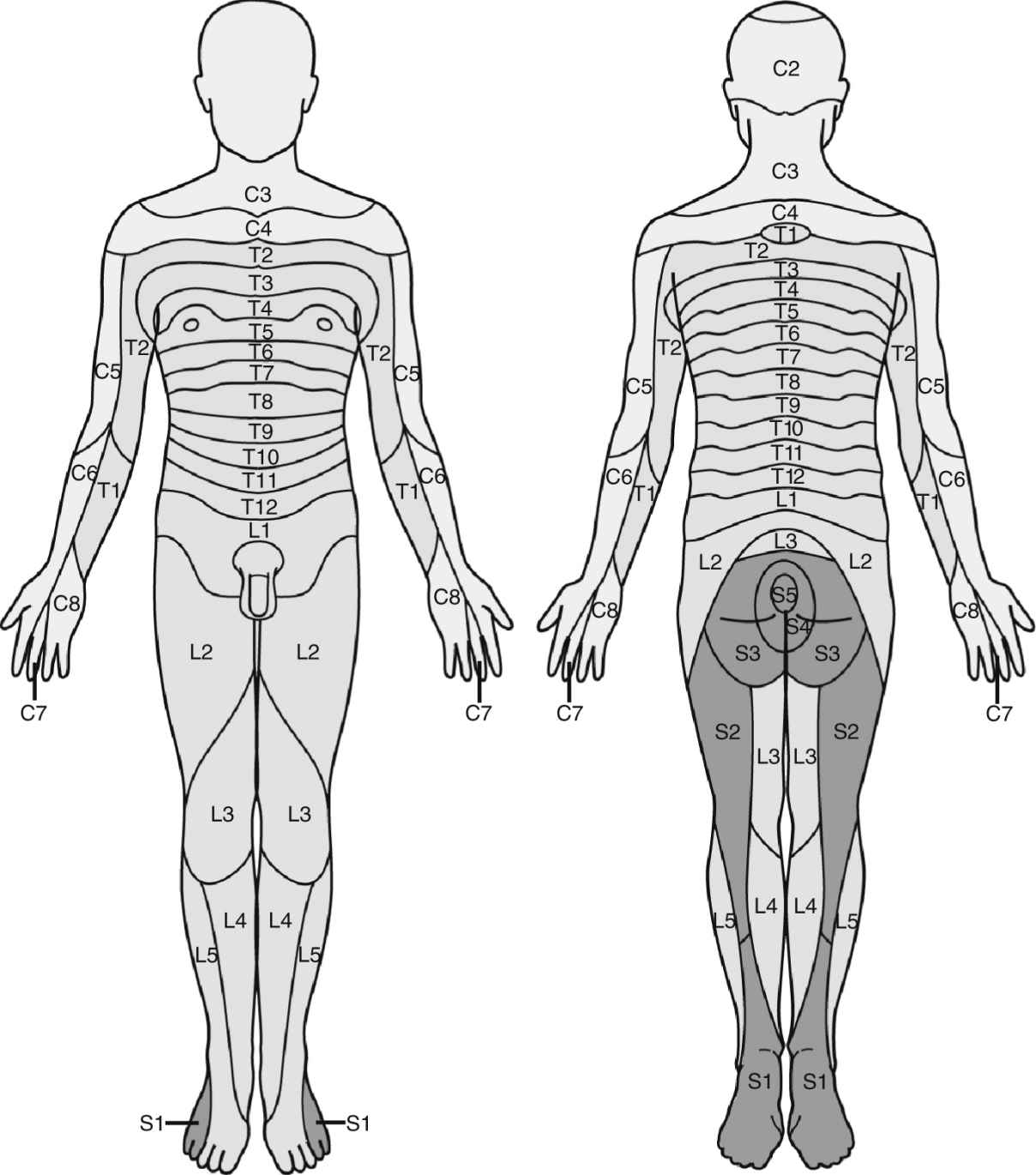
FIG. 25.5 Dermatomes. (From Nagelhout JJ, Elisha S: Nurse Anesthesia, ed 6, St. Louis, MO, 2017, Elsevier.)
Combined spinal-epidural is a versatile technique that allows for the administration of a spinal anesthetic for immediate anesthesia and an epidural to extend the duration of the anesthetic or provide for postoperative analgesia. It is similar to spinal-epidural anesthesia with regard to positioning, sterile technique, monitoring, progression, and assessment.
Neuraxial Complications
Complications related to neuraxial blockade can range from minor to life-threatening. Anticipation, recognition, and prompt intervention are essential roles of the perianesthesia nurse.20
High Spinal Block
Excessive spread of local anesthetic that occurs with spinal or epidural anesthesia is a high spinal block. Signs and symptoms include high sensory block resulting in upper extremity sensory and motor changes, nausea and vomiting, loss of consciousness, anxiety, hypotension, bradycardia or asystole, respiratory distress, or apnea. Treatment is dependent on extent of spread. Airway, breathing, and circulation are primary considerations. Supplemental oxygen, assistance with a bag-mask-valve device, or intubation may be required. The patient may be aware of the surrounding environment, and verbal reassurance is important to reduce anxiety. Hypotension is caused by an extensive sympathectomy and treated with fluid bolus, elevation of the legs, and vasopressors (see Chapter 11), which may include phenylephrine, norepinephrine, ephedrine, or epinephrine. Bradycardia is treated with ephedrine or atropine. Phenylephrine and norepinephrine administration can cause reflex bradycardia and should be used with caution in the setting of significant bradycardia. Asystole is treated with established advanced cardiovascular life support (ACLS) protocol. High spinal blocks are generally self-limiting, and the patient will improve as the concentration of local anesthetic declines.1,5,7,9
Local Anesthetic Systemic Toxicity
See Chapter 24.
Hypotension
Postoperative hypotension can be caused by sympathectomy and can occur with spinal or epidural anesthesia. Treatment consists of raising the legs, fluid bolus, and vasopressors (i.e., ephedrine or phenylephrine). Refractory hypotension can be treated with a continuous infusion of phenylephrine, norepinephrine, or low-dose epinephrine. It is important to rule out other causes of hypotension during stabilization including hemorrhage or cardiovascular complications (see Chapter 29).1,5,7,9
Nausea and Vomiting
Urinary Retention
Urinary retention is often caused by autonomic blockade of the sacral nerves that results in a hypotonic bladder. Other causes such as surgical genitourinary trauma, pain, opioids, and renal failure should be ruled out. Patients may exhibit restlessness and incoherence. A neurologic insult, electrolyte disorders, hypoxia, pain, and abnormal glucose levels should also be ruled out. A bladder scan can help to confirm retention, and insertion of a urinary catheter is the treatment.9,21
Hypothermia
Regional anesthesia results in centrally mediated vasodilatation and inhibits peripheral vasoconstriction, transferring body heat from the core to the periphery through radiation, convection, conduction, and evaporation. Recognition of hypothermia and initiation of measures to return the patient to a normal temperature are important considerations22 (see Chapter 53).
Postdural Puncture Headache
This condition is caused by leaking CSF through the dura, which can occur with spinal anesthesia or inadvertent dural puncture with an epidural. Symptoms usually occur 24 to 48 hours after dural puncture. Symptoms include a headache in the occipital-frontal region that intensifies when upright and declines when supine, nuchal rigidity, visual and auditory disturbances, and nausea and vomiting. Significant neurologic complications such as meningitis, intracranial tumors, and hemorrhage should be ruled out. Treatment is initially symptomatic and includes bed rest, fluids, caffeine, and analgesics. If persistent, an epidural blood patch is the definitive treatment and is highly successful (95% success rate). The anesthesia provider accesses the epidural space at one space below the dural puncture; 15 to 20 mL of the patient’s blood is drawn aseptically and administered through the epidural needle. The patient remains on bed rest for 30 to 60 minutes before ambulation. Complications include back pain, fever, meningitis, and arachnoiditis.5,9,16,23
Neurologic Complications
The overall incidence after neuraxial blockade is 0.04%, and permanent injury is rare.20 Palsies, paralysis, or pain should be reported immediately to the anesthesia provider and surgeon. This complication may be related to traumatic needle placement, bleeding or hematoma formation, surgical trauma, or injury related to a portion of the body being insensate. A neurologic consultation may be required to help diagnose and manage the patient’s condition.5,9,24
Possible causes of postoperative neurologic deficits are given in Box 25.2.
Transient Neurologic Symptoms
These symptoms are most often associated with spinal lidocaine, although it can occur with any local anesthetic. Signs and symptoms usually appear within 24 hours of block resolution and consist of low back pain with radiation to the lower extremities. Risk factors include lidocaine, obesity, and lithotomy position.20 It is important to rule out other more serious causes. It is generally self-limiting, with full recovery occurring in 2 to 7 days.25 Factors that do not increase the risk of transient neurologic symptoms after lidocaine spinal anesthesia are given in Box 25.3.
Cauda Equina Syndrome
Cauda equina syndrome is associated with lidocaine and continuous spinal microcatheters. It manifests with low back pain with radiation to the lower extremities as well as sensory and motor changes. Prospects of recovery are poor.9 Infectious complications such as meningitis, epidural abscess, and arachnoiditis can occur but are extremely rare.5,9
Spinal or Epidural Hematoma
Spinal or epidural hematoma is rare but devastating. It is more likely to occur in patients with altered homeostasis. Symptoms include low back pain, motor changes, and bowel or bladder dysfunction. Treatment is emergent decompression, but recovery is poor if surgery is delayed more than 8 hours. Awareness of coagulation-altering medications and notification of anesthesia personnel may prevent this complication from occurring.5,9,10
Care of Patients After Neuraxial Blockade
In addition to routine postanesthesia care unit (PACU) Phase I care for patients receiving sedation, the perianesthesia nurse should perform a continual assessment for complications as outlined. Rapid intervention is required for hypotension or bradycardia. Care should be taken not to rapidly change the patient’s position as this may cause hypotension related to residual sympathectomy. Ensure the patient’s insensate limbs are positioned in correct anatomic alignment and padded to prevent injury.26 Any concerns should be reported to the anesthesia provider. Before discharge, the patient should meet the standards for discharge criteria applicable to all patients recovering from anesthesia. Additional concerns include a less than 10% decrease in blood pressure with position change and a sensory level equal or less than T10 with evidence that the block is receding by at least two sensory segments. There is no required minimum stay time, but length of stay should be tailored to the individual patient’s needs.27 Each institution must develop policies to determine the safe discharge criteria of a patient after a neuraxial block. Sensory and motor regression should be defined so recovery can be assessed.






Full access? Get Clinical Tree


