Fig. 16.1
The flow of cryogen in a cryoprobe. The majority of the cryoprobe is protected by a shield, allowing the tip to extract heat from the surrounding tissue. The choice of cryogen determines the lowest temperature of the cryoprobe
Using continuous freeze/defrost cycles and a larger probe can maximize disruptions within the nerve, causing both osmotic and mechanical damage. The repeat cycles decrease the temperature at sites away from the target nerve and maximize the size of the ice ball on the nerve target. At −20 °C, all nerve fibers stop conducting impulses through the nerve, and lower temperatures may lead to Wallerian degeneration, leaving the myelin sheath, endoneurium, and Schwann cell basal lamina intact allowing for regeneration. The extent of the block depends on the duration of exposure and temperature of the probe. However, long-term effects are thought to be caused by autoimmune responses via the release of sequestered proteins at the site of the treated nerve [3].
Radiofrequency Ablation
Radiofrequency (RF) ablation is a minimally invasive percutaneous procedure that is thought to reduce pain by altering the transmission of pain impulses [4, 5]. Conventional RF ablation (CRFA) causes controlled tissue destruction by irreversible coagulative necrosis [6]. However, recent evidence demonstrates that CRFA provides only a transient sensory loss in contrast to a much longer duration of pain relief. Electric fields produced by RF current may induce changes in the nerve cells and alter pain processing mechanisms at various sites, particularly at the molecular level [4].
All RF ablation techniques involve the transfer of alternating RF current (450–1,200 kHz) through insulated needle electrodes. The electrode is insulated, except for 2–10 mm at the tip. RF needles tend to be smaller than cryoprobes (Fig. 16.2). The electrode is positioned close to the target using nerve stimulators and image guidance. In conventional RF neurotomy, the electrode is positioned parallel to the target as the electrode coagulates transversely. A generator produces an electric field concentrated at the uninsulated tip of the electrode. The transfer of energy generates molecular oscillations that produce ionic friction and heat within the tissues. Once the cells are heated above a certain temperature, controlled tissue destruction occurs causing a lesion surrounding the uninsulated tip [6]. Early studies claimed that RF coagulation destroyed Aδ and C fibers preventing nociception. However, subsequent studies have shown that RF coagulation is non-selective and disrupts all nerves [4–7].
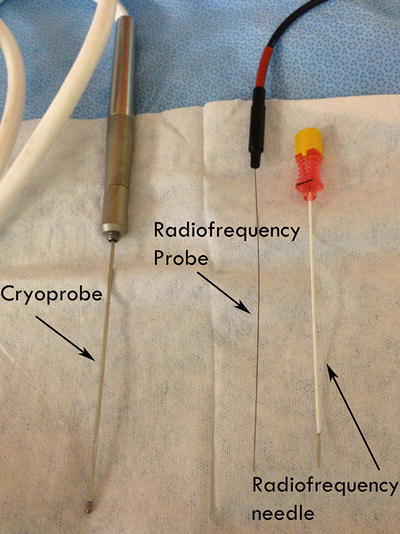
Fig. 16.2
Shown is a cryoprobe with a diameter of 1.7 mm, a RF probe with a much smaller relative diameter, and a 20-gauge RF needle that allows the probe to be introduced to the target
Pulsed Radiofrequency Ablation
Pulsed RF ablation (PRFA) was described by Slappendel et al. that compared the outcomes of cervical RF at the dorsal root ganglion (CRFA) in patients treated with lesions made at 40 °C to those at 67 °C [8]. While changing the temperature did not impact efficacy, it was believed that the RF current itself was therapeutic because of the overall electrical effects on the target nerve. The therapeutic effect of PRFA current is provided by applying brief bursts of RF energy and allowing the heat to dissipate at the target tissues, avoiding further damage to the nerve [9].
In PRFA, a current of 50,000 Hz is usually delivered in 20-msec pulses at a frequency of 2 per second (other protocols have been described). The electrode temperature is limited to 42 °C preventing any thermal lesion [8, 10]. The current is densest distal to the tip of the electrode and in contrast to CRFA, the electrode is applied perpendicular to the target nerve. Laboratory studies show that heating a nerve to a lower temperature (40–45 °C) causes reversible conduction blocks, but no pathologic lesion is produced [9, 11]. The distance of the electrode from the nerve target influences tissue damage in both CRFA and PRFA. Within 500 μm from the electrode, both CRFA and PRFA protocols produced tissue damage. Between 500 and 1,000 μm, tissue damage occurred with CRFA protocols, but not in PRFA protocols. Electron microscopy shows that ganglia treated with CRFA causes significant neuronal damage, whereas the ganglia treated with PRFA leaves nuclear membranes intact. However, studies demonstrating the efficacy of PRFA is limited as truly randomized clinical trials are lacking [8, 11].
Cooled RF Ablation
Cooled RF ablation (cooled RFA) is a newer RF technique used to treat various pain syndromes. The mechanism of pain relief is similar to CRFA. An electrode is placed close to the target nerve and conduction is disrupted relieving the pain. Cooled RFA utilizes a specialized electrode which is actively cooled by a continuous flow of water at ambient temperatures. This prevents the electrode from acquiring high surrounding tissue temperatures and increases the overall exposure to the RF current, heating larger tissue volumes with a higher thermal lesion. Similar to conventional RF, the lesion size depends on the size of the probe, the electrode temperature, and the duration of RF current that is applied [12]. Perhaps by delivering larger amounts of RF current to the target nerve, cooled RFA can be used in treating pain syndromes where conventional RF is unsuccessful [13, 14].
The Neuroanatomy of the Viscera
Most painful stimuli from abdominal viscera are transmitted by unmyelinated C fibers found in muscle, periosteum, mesentery, peritoneum, and viscera. The pain is characterized as dull, cramping, burning, gnawing, and gradual in onset. Secondary autonomic effects such as sweating, restlessness, nausea, vomiting, perspiration, and pallor can accompany the visceral pain. Abdominal visceral nociceptors respond to both mechanical and chemical stimuli. Visceral pain tends to be midline as sensory afferents are sent to both sides of the spinal cord. It is also poorly localized since the innervation is multi-segmental and the number of nerve endings is minimal [15]. The afferent fibers that mediate abdominal visceral pain usually follow the distribution of the autonomic nervous system, and consequently, the autonomic ganglia are the main targets for pain relief.
Sympathetic Nervous System
The sympathetic nervous system originates from the spinal cord in the thoracolumbar region, arising from the T1 to L3 levels. The preganglionic sympathetic fibers have cell bodies in the intermediolateral columns. From these cell bodies, nerve fibers continue to paired sympathetic chains, unpaired distal plexuses, or collateral ganglia near target organs. The paired sympathetic chains form 22 paired ganglia that lie on either side of the vertebral column. The preganglionic fibers leave the cord in the anterior nerve roots, join the spinal nerve trunks that connect the ganglia to each other, and enter the ganglion through the white ramus at their respective level. Additionally, the gray rami communicans connect the ganglia to the spinal nerves [15].
In the upper abdominal cavity, preganglionic fibers from T5 through T9 join together to form the greater splanchnic nerves serving the celiac ganglia. In the middle abdomen, nerve fibers from T10 and T11 form the lesser splanchnic nerves serving the aorticorenal ganglia. In the lower abdomen, nerve fibers from T12 form the least splanchnic nerves serving the superior mesenteric ganglia and nerve fibers from L1 through L3 form the lumbar splanchnic nerves serving the inferior mesenteric ganglia. The postganglionic fibers from the celiac, superior, and inferior mesenteric plexuses innervate the viscera of the abdomen and pelvis. Postganglionic fibers arising from synaptic links of the thoracic, lumbar, and pelvic sympathetic fibers form numerous plexuses, such as the cardiac, celiac, hypogastric, and plevic plexuses. Lastly, ganglia of the third type, the terminal or collateral ganglia, form near their target organs (e.g., adrenal medulla) [16, 17].
Parasympathetic Nervous System
The parasympathetic nervous system arises from cranial nerves III, VII, IX, and X and from the sacral spinal cord. The vagus nerve supplies the heart, tracheobronchial tree, liver, spleen, kidney, and entire gastrointestinal tract except for the distal part of the colon. Most vagal fibers do not synapse until they arrive at small ganglia on and about the thoracic and abdominal viscera. The preganglionic fibers are long, but the postganglionic fibers are short. The second through fourth sacral nerves form the pelvic splanchnic nerves. They synapse in terminal ganglia associated with the rectum and genitourinary organs also known as the ganglion impar [15].
Enteric Nervous System
The enteric nervous system (ENS) consists of a network of neurons within the walls of the gastrointestinal tract, the pancreas, and the gallbladder. The ENS functions independently from the sympathetic and parasympathetic systems as seen when digestion and peristalsis occur after spinal cord transection [18]. While not directly involved in pain sensation, secretory and neuronal mediators can cause signaling along the autonomic nervous system, which may be perceived as discomfort.
Referred Pain
Stimulation of the autonomic nervous system in the viscera may lead to referred pain, defined as a sensation perceived at a remote area from the site of the stimulus. Referred pain results from visceral and somatic afferent neurons converging on second-order neurons in the spinal cord. The best-known example is the pain experienced during a myocardial infarction. The damaged myocardium transmits pain signals via visceral afferent neurons to the T1–T4 levels of the spinal cord on the left side. These signals “converge” with somatic afferent neurons of the left chest and left arm at the same level. Thus, damaged myocardium is perceived as left chest and arm pain [19]. Similar pain is seen with pancreatic cancer (mid-back pain) and renal disease (groin and testicular pain) (Table 16.1).
Visceral pain location | Somatic referral pattern |
|---|---|
Esophagus | Upper back and left chest |
Pancreas and duodenum | Epigastric and mid-thoracic back |
Liver disease and capsular pain | Right shoulder and right upper abdomen |
Splenic disease and capsular pain | Left shoulder and left upper abdomen |
Kidney and bladder | Flank pain, groin pain, testicular pain |
Ovary | Groin and flank pain |
Distal colon | Left lower abdominal quadrant |
Testicular, prostate | Flank and groin pain |
Autonomic Targets for Visceral Pain
Thoracic Sympathetic Block [20]
Indications: Pain related to lung and esophageal cancer, post-herpetic neuralgia, thoracic vertebral pain
Anatomy: Since the thoracic somatic nerves are close to the thoracic sympathetic chain, both neural pathways may be neurolyzed when approaching the thoracic sympathetic ganglion. The lower cervical ganglion and first thoracic ganglion are fused to make up the stellate ganglion at the level of the 7th cervical vertebrae. In moving caudad, each upper thoracic ganglia lie just beneath each rib. The lower thoracic ganglia are more anterior to the upper thoracic ganglia and lie along the posterolateral surface of each vertebral body. The pleural space is in close proximity and lies lateral and anterior to the thoracic sympathetic chain.
Technique: Usually the sympathetic chain is targeted using fluoroscopic or CT guidance. The needle is usually directed to the tip of the transverse process and redirected inferiorly to the inferior margin of the transverse process. After verifying the correct position, the needle is aspirated to ensure no blood or CSF and neurolysis is performed.
Complications: Pneumothorax, hemothorax, intrathecal neurolysis
Celiac Plexus Block [21, 22]
Indications: The celiac plexus block is used to treat pain related to pancreatic cancer, bile duct cancer, gastric cancer, or primary liver neoplasm; as well as chronic pancreatitis and chronic abdominal pain.
Anatomy: The plexus is located at the level of the upper part of the 1st lumbar vertebra and surrounds the celiac artery. It lies in between the suprarenal glands, in front of the crura of the diaphragm and abdominal aorta, and behind the stomach and omental bursa.
Related posts:
 Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
 Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
 Peripheral Nerve Stimulation for Chronic Abdominal Pain
Peripheral Nerve Stimulation for Chronic Abdominal Pain
 The Epidemiology of Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain

Full access? Get Clinical Tree


