Key Clinical Questions
What information do pulmonary function tests provide in addition to the history and physical examination?
What specific tests might you order to evaluate the acutely ill hospitalized patient and how does each test influence diagnostic evaluation or management?
What operations require preoperative pulmonary function tests as part of the preoperative evaluation?
What are the predictors of increased postoperative risk?
Introduction
Pulmonary function tests (PFTs) objectively assess lung function. Along with measurement of arterial blood gases, PFTs are used to evaluate how much a patient’s symptoms or known lung disease impairs daily activities and the tests are helpful in management, such as when to treat a patient and in what setting. The purpose of PFTs is to evaluate dyspnea by assessing the mechanical function of the respiratory system, to quantitate the loss of lung function, and to monitor disease progression and response to treatment. PFTs also predict postoperative risk of pulmonary complications and which patients will likely have adequate pulmonary function after lung resection. Serial evaluations monitor respiratory muscular strength in progressive neuromuscular diseases such as Guillain Barre, myasthesia gravis, and muscular dystrophy.
Volumes or the ability of the lungs to fully expand (TLC, FRC, RV)
Flow rates or the rate of inflow and outflow of air (FEV1, forced expiratory flow [25–75%])
Maximum voluntary ventilation or airflow through major airways by rapid inspiration and expiration maneuvers (MVV)
Maximum inspiratory and expiratory pressure, a measure of respiratory muscle strength (Pi[max], Pe[max])
Diffusing capacity (DLCO) or measurement of the ability of oxygen to get into the blood.
Interpretation will be (1) normal, (2) obstructive, (3) restrictive, or (4) combined obstructive and restrictive. For the majority of PFTs to be meaningful, patients must be able to physically perform the tests and to follow instructions. With the exception of oximetry, arterial blood gases (ABGs), and simple spirometry, PFTs are usually performed in the outpatient setting. Hospitalists should be able to (1) recognize patterns of pulmonary involvement when they review outside medical records, (2) know when to order specific tests to evaluate acutely ill patients, and (3) avoid unnecessary ordering of PFTs when they are of limited utility in hospitalized patients.
Components of Testing
PFTs will detect significant increased resistance to airflow (airway obstruction) and increased resistance to expansion (parenchymal disease, weakness of respiratory muscles or abnormalities of the chest wall or diaphragm). ABGs supplement PFTs by measuring the effect of pulmonary and other illnesses on oxygenation and ventilation (Figure 103-1).
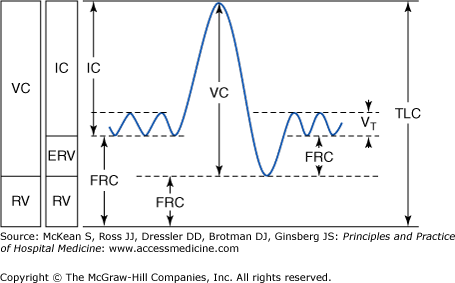
- TLC = Total lung capacity or the total volume of gas within the lungs after a maximal inspiration
- RV = Residual volume or the volume of gas remaining in the lungs after a maximal expiration
- VC = Vital capacity or the volume of gas expired after a maximal inspiration followed by a maximal expiration
- FRC = Functional residual capacity or the volume of gas within the lungs at the end of expiration during normal tidal breathing at rest
To quantitate VC, ask the patient to breathe into a spirometer and obtain a spirometric tracing. To quantitate RV, FRC, and TLC, other methods such as dilution tests or body plethysmography are needed to measure the amount of air left in the lungs. These measurements require significant expertise on the part of the respiratory therapist in the PFT laboratory and maximal patient cooperation and ability to follow instructions. Inert gas dilution may underestimate lung volumes when there is airflow obstruction in patients who have air spaces such as bullae within the lung that do not communicate with the bronchial tree. Body plethysmography may overestimate lung volumes in airflow obstruction but may provide a more accurate measurement of intrathroacic gas volume in patients with noncommunicating airspaces within the lung.
Most diffuse lung disease is associated with decreased lung volumes. Restrictive PFTs means limitation to full expansion of the lungs. Volumes are decreased but flow rates are normal. Interstitial lung disease has reduced lung compliance and a restrictive defect. PFTs will reveal a decreased TLC, FRC, and RV. Although FEV1 and FVC may be decreased secondary to decreased volumes, the FEV1/FVC ratio is normal or increased. When the TLC and VC are decreased, the differential diagnosis includes restrictive lung disease (pulmonary fibrosis) or loss of lung volume (surgery, diaphragmatic paralysis, or skeletal problems). Decreases in the TLC, RV, and FRC can be interpreted as mild (60% to 80% reduction), moderate (40% to 60% reduction) or severe (<40% reduction). Marked decreases in the VC may also occur in certain neuromuscular diseases, and serial testing may be used to monitor disease progression in Guillain Barre Syndrome, myasthenia gravis, and muscular dystrophy.
Measurement of flow rates requires that the patient breathe into a spirometer as hard and as fast as possible from TLC down to RV. The information can be displayed as a flow versus volume graph or a volume versus time graph. The volume expired during this test is the forced vital capacity or FVC. The amount expired during the first second is the forced expiratory volume in 1 second, or FEV1. This maneuver also reports the forced expiratory flow between 25% and 75% of VC (FEF 25–75%), also referred to as the maximum midexpiratory flow rate (MMEFE or MMFR), which is the rate of airflow during the middle one-half of the expiration capacity. It is not effort or technique dependent (Figure 103-2).
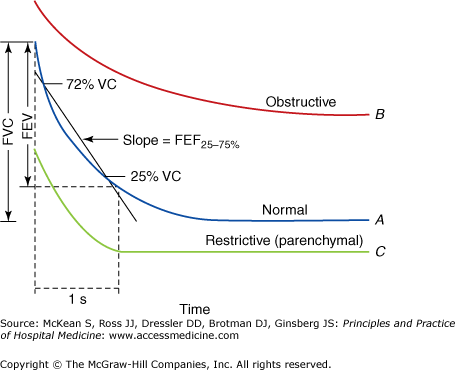
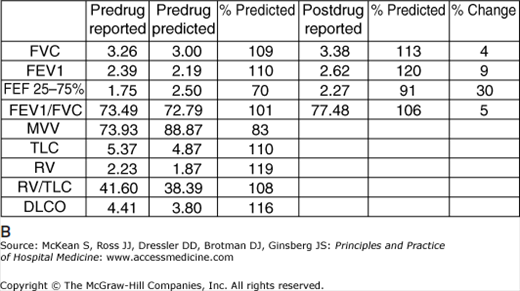
Obstructive lung disease such as chronic obstructive pulmonary disease (COPD) is a spectrum of disorders that have in common impairment in expiratory flow. Diagnosis is made by spirometry showing a permanent reduction in FEV1/FVC ratio below 75%. The slow vital capacity or SVC will be greater than the FVC when the FVC is decreased in the setting of obstruction. Decreases in both FEV1 and FVC and a normal FEV1/FVC would suggest restrictive disease. Spirometry can be used to determine the degree of reversibility of the airways to bronchodilators and adequacy of treatment of obstructive airway disease. An increase in FEV1 of 200 cc or 12% is considered a significant response to bronchodilators and inadequately treated obstructive lung disease.
In addition to spirometry, flow rates may be measured using peak flow meters. Peak flow rates usually occur in the very early stages of the FVC maneuver and may be useful in measuring obstructive airway disease. Although a very simple test easily performed without too much training on the part of the operator or the patient, measuring the peak flow is very effort dependent and is not accurate enough to replace spirometry. The predicted values are rather nonspecific and the previously described prediction of severity of disease does not apply to these values. However, in the hospital it allows for a very simple, objective way of monitoring a patient’s obstructive airway disease and response to therapy. Measuring the peak flow is a simple way for patients with asthma to objectively measure the degree of obstruction, starting in the hospital in preparation for discharge home when patients should monitor their peak flow and understand when they need to return for medical evaluation before they are so ill that they need to be rehospitalized. A peak expiratory flow calculator using age, sex, and height may be found at the link http://www.dynamicmt.com/PEFform.html.
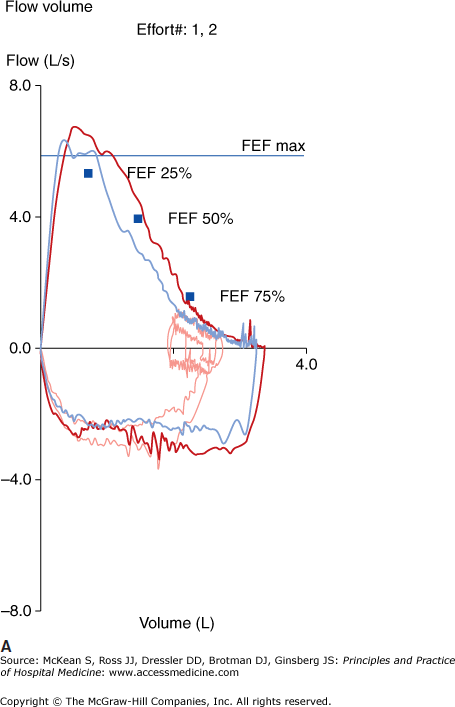
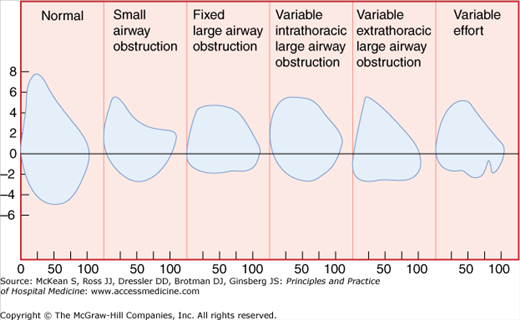
The flow volume loop graphically records the maximal inspiratory and maximal expiratory maneuvers with flow on the Y axis and volume on the X axis. The patterns of the flow volume loops can be diagnostic of various types of obstruction including intra- and extrathoracic obstruction, or fixed or variable obstruction. Although the beginning of a forced expiratory maneuver depends on effort, the latter part of forced expiration primarily reflects the mechanical properties of the lung and the resistance to airflow. The evaluation of the flow volume loop may be a qualitative visual analysis of the shape and concavity of the expiratory portion of the curve or a quantitative analysis comparing observed flow rates at specified volumes with predicted values.
In a fixed obstruction, changes in pleural pressure do not affect the degree of obstruction, and the inspiratory and expiratory portions of the curve reveal a plateau, reflecting a limitation in peak airflow of both inspiration and expiration.
In a variable obstruction the location of the lesion and the effect of alterations in pleural and airway pressure with inspiration and expiration determine the amount of obstruction. If the lesion is intrathoracic, the flow volume loop will demonstrate airflow limitation during expiration. If the lesion is extrathoracic, the flow volume loop will demonstrate airflow limitation during inspiration (Figure 103-3).
In obstructive disease the flow volume loop demonstrates a decrease in the expiratory loop, especially at the later part of the expiration (Figure 103-4).
This is the measurement of the maximum amount of air a patient can move in 12–15 seconds, using a spirometer. The results are expressed in liters/min. Because MVV tests airflow through major airways and muscle strength, consider weakness of respiratory muscles, especially the diaphragm, if MVV is low and flow rates are normal. Major airway lesions and neuromuscular disease result in a decreased MVV. Obstructive disease may also have a low MVV (MVV = FEV1 × 33). In theory, isolated restrictive disease should have a normal MVV; however, it is a nonspecific test and reductions are seen in pulmonary diseases (restrictive and airway obstruction) and in neuromuscular disease (loss of coordination, diminished cognitive function, and overall deconditioning).
Between 10% and 30% of patients with Gullian Barre Syndrome will require ventilatory support. Patients most likely requiring mechanical ventilation present within 7 days of onset of symptoms, FVC < 60% predicted, maximal inspiratory pressure (MIP) < 30 cm H2O, or an expiratory pressure < 40 cm H2O. These patients are at great risk of requiring mechanical ventilation and should be monitored carefully with serial FVC and inspiratory pressure measurements.
This is a good estimate of muscle strength, which would be presumed to be normal with a normal maximum inspiratory and expiratory pressure. Patients must be able to cooperate with the test.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


