CHAPTER 27 Psoas block
Clinical anatomy
The lumbar plexus is formed by the ventral rami of the first three lumbar nerves and the greater part of the ventral ramus of the fourth, with a contribution from the twelfth thoracic nerve root in 50% of cases. It lies in front of the transverse processes of the lumbar vertebrae, deep within the psoas major muscle (Fig. 27.1). The nerve roots of the lumbar plexus lie in a ‘cleavable’ space in the psoas major muscle (Fig. 27.2). The space is limited superiorly by the insertion of psoas major on the body of the vertebrae; posteriorly by the lumbar transverse processes and peridural space; and anteriorly by the aponeurotic continuation of the fascia iliaca. The erector spinae (medial) and quadratus lumborum (lateral) muscles are superficial to and posterior to the psoas muscle.
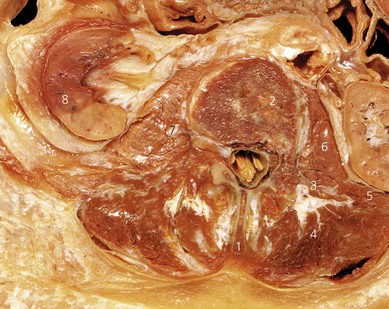

Anatomically, the psoas muscle is regarded as one mass and there is no ‘compartment’ as such within the muscle. Nevertheless, injectate does infiltrate the muscle (Fig. 27.3) and covers the lumbar roots and nerves running within the muscle. The roots join and form the lumbar plexus within the psoas muscle. Branches of the plexus include the femoral, obturator, and lateral cutaneous nerves of the thigh.
Surface anatomy
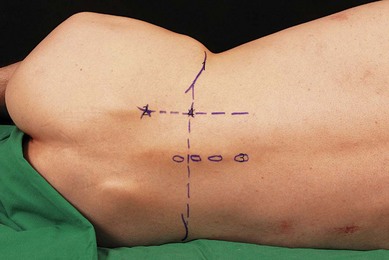
Important landmarks for the psoas block include the iliac crests, the posterior superior iliac spine, and the vertebral column (Fig. 27.4). The posterior superior iliac spine is the bony prominence at the posterior end of the iliac crest. It is directly below the ‘sacral dimple’ (dimple of Venus), a dimple in the skin visible above the buttock, close to the midline.
Sonoanatomy
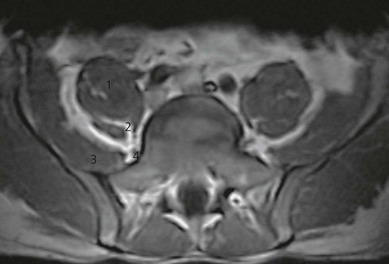
Ultrasonographic visualization of the psoas muscle in adults requires a low frequency transducer (5–8 MHz) due to the depth of the lumbar plexus (5–8 cm). A high frequency transducer can also be used, particularly in children. For longitudinal sonograms, the transducer is placed 3 cm lateral to the spinous processes (Fig. 27.5). This allows for identification of the transverse processes. The transverse processes produce bright hyperechoic signals, with signal loss distally. The psoas muscle is seen deep to these structures (Fig. 27.6). The transducer is advanced caudally and then cranially to identify the respective lumbar interspaces. The sacrum is identified as a continuous hyperechoic line. The longitudinal sonographic pattern of the psoas muscle demonstrates a hypoechoic background interspersed with hyperechoic bands (dots on transverse view) representing fibrous structures within the muscle. Unlike the sonoanatomy in children, visualization of the lumbar plexus in adults is substantially impaired by these structures, and often is impossible to identify. The kidneys are visualized as oval shaped structures usually at the level of L2 or L3, and therefore can be avoided during ultrasound-guided psoas compartment block. The kidneys can also be seen to move with respiration. The more hyperechoic, wedge-shaped, psoas muscle lies medial and deeper to the kidneys. At the interspace of L4–L5, the transducer is rotated 90° into the transverse plane (Fig. 27.7).
< div class='tao-gold-member'>








Full access? Get Clinical Tree


