The sciatic nerve provides sensory and motor innervation to the lower extremity. Its articular branches innervate the hip joint through the posterior capsule, the posterior knee joint, and the ankle joint [14, 18, 26]. Its muscular branches innervate muscles in the gluteal area (gluteus maximus, medius, and minimus muscles) and the thigh (adductor magnus, long and short heads of biceps femoris, semitendinosus, semimembranosus). Distally, the sciatic nerve provides innervation to the leg, ankle, and foot.
Ultrasound-Guided Block Technique
This chapter will limit the description of ultrasound-guided sciatic nerve block techniques to approaches in the gluteal, infragluteal, and the proximal thigh regions.
Gluteal Approach
Patient Positioning
(a)
Place the patient in the semiprone (Sims) position with the hip and knee flexed and the operative side up.
(b)
Identify the greater trochanter (GT) of the femur, the posterior superior iliac spine (PSIS), and the sacral hiatus (SH) (Fig. 60.2).
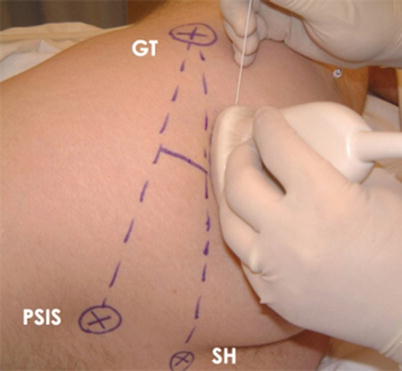
Fig. 60.2
Gluteal approach surface landmarks. GT greater trochanter of the femur, PSIS posterior superior iliac spine, SH sacral hiatus (Figures are reproduced with permission of www.USRA.ca)
Sonographic Imaging
(c)
Sterilize the skin and scan with a low-frequency curvilinear 2–5-MHz ultrasound transducer covered by a sterile adhesive dressing.
(d)
Place the transducer in the transverse plane on the buttock at approximately the level of the ischial tuberosity.
(e)
Optimize the machine setting to capture a short-axis view of the sciatic nerve. A depth >4 cm is usually required.
(f)
Start by moving the transducer cephalad from the ischial tuberosity level to identify the internal bony landmark ischial bone which casts a wide bony acoustic shadow. The most medial aspect of this bone is the ischial spine.
(g)
Often another bony landmark, the greater trochanter or the hip joint, is seen lateral to the ischial bone.
(h)
Next locate the muscular landmarks, the gluteus maximus muscle (the outer muscle layer) and the superior and inferior gemellus muscles (the inner muscle layers) that are all superficial and posterior to the ischial bone.
(i)
The sciatic nerve is expected to be visualized deep (anterior) to the gluteus maximus muscle layer and superficial (posterior) to the superior and inferior gemellus muscles as well as the ischial bone.
(j)
The sciatic nerve in the gluteal region is usually hyperechoic (bright), wide and thin in the cross-sectional (short-axis) view (Fig. 60.3).
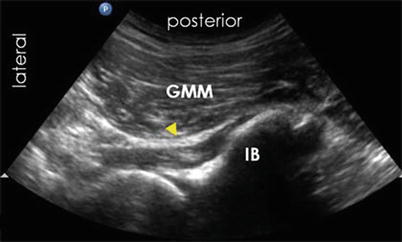
Fig. 60.3
Gluteal approach sonographic appearance. Arrow designates sciatic nerve. IB ischial bone, GMM gluteus maximus muscle (Figures are reproduced with permission of www.USRA.ca)
(k)
The pulsatile inferior gluteal artery is often visualized in close proximity to the sciatic nerve in this region. Use color Doppler to confirm.
(l)
It may also be possible to locate the internal pudendal vessels (artery and vein) near the ischial spine that are significantly medial to the sciatic nerve.
(m)
Scan the nerve proximally and distally to follow its course and confirm its identity in both the short-axis and long-axis views.
Needling
(n)
Ultrasound-guided gluteal sciatic nerve block is considered an advanced block technique.
(o)
The gluteal sciatic nerve block is amenable to both in-plane (IP) and out-of-plane (OOP) approaches. One may prefer the OOP approach for blocking this nerve in this deep location because the block needle travels the shortest skin to nerve distance. Also, the OOP approach is often used for catheter insertion. For single-shot injection, following local anesthetic skin infiltration, an 80–100-mm 22G insulated block needle is inserted often under combined ultrasound and nerve stimulation guidance because ultrasound alone may not always visualize accurately the needle tip or nerve location. After obtaining a satisfactory ultrasound and nerve stimulation response endpoint, a bolus of local anesthetic, 15–20 mL, is injected incrementally for postoperative analgesia. A dilute bupivacaine (0.25 % or less) or ropivacaine (0.5 % or less) solution is the local anesthetic of choice to achieve analgesia without a prolonged foot drop.
(p)
For the IP approach, the block needle is advanced in a lateral-to-medial direction through the gluteus maximus muscle, along the long axis of the transducer, in the plane of the ultrasound beam. This allows needle visualization in real-time during needle advancement.
(q)
The technical challenge with this block often relates to needle-tip visualization which is hampered by the steep angle of needle insertion. Hydrolocation, i.e., injecting small volumes of local anesthetic (1–2 mL) is recommended to serve as a surrogate marker of the needle-tip position.
(r)
Another technical challenge is to visualize the nerve in short axis since it may appear thin and wide. In this case, it is helpful to rotate the transducer 90° to locate the nerve in the long-axis view which can show a hyperechoic longitudinal structure running cephalad and caudad.
(s)
Electrical nerve stimulation to elicit twitches in the muscle groups innervated by the tibial nerve and/or peroneal nerve further confirms needle-to-nerve contact.
(t)
The ideal endpoint for local anesthetic injection is to achieve a circumferential spread pattern around the sciatic nerve. Needle-tip position may be adjusted as needed to achieve this endpoint. However, it is not always practical or possible to deposit local anesthetic deep to the nerve and one must be cautious to avoid multiple needle attempts and the potential risk of needle trauma to the nerve.
(u)
For the OOP approach, the sciatic nerve image is aligned at the midpoint of the transducer and the block needle is inserted inferior to the transducer to reach the nerve target.
Subgluteal Approach
Patient Positioning
(a)
Place the patient in the semiprone (Sims) position with the hip and knee flexed and the operative side up.
(b)
Identify the GT of the femur and the ischial tuberosity (IT) (Fig. 60.4).

Fig. 60.4
Infragluteal approach surface landmarks. GT greater trochanter of the femur, IT ischial tuberosity (Figures are reproduced with permission of www.USRA.ca)
Sonographic Imaging
(c)
Sterilize the skin and scan with a low-frequency curvilinear 2–5-MHz ultrasound transducer covered by a sterile adhesive dressing.
(d)
Place the transducer oblique over the subgluteal region of the buttock to capture a cross-sectional view of the sciatic nerve.
(e)
Optimize the machine setting to proper depth; 3–4 cm is often required.
(f)
Identify the internal bony landmarks, the greater trochanter (GT) laterally, and the ischial tuberosity (IT) medially.
(g)
Identify the muscular landmarks, the gluteus maximus muscle (GMM), the outer muscle layer, and the quadratus femoris muscle (QFM), the inner muscle layer.
(h)
The sciatic nerve often appears hyperechoic and elliptical in the subgluteal region. It is expected to be visualized in the fascial plane between the GMM and the QFM (Fig. 60.5).

Fig. 60.5
Infragluteal approach sonographic appearance. GMM gluteus maximus muscle, GT greater trochanter of the femur, IT ischial tuberosity, QFM quadratus femoris muscle. The sciatic nerve is indicated by the arrow (Figures are reproduced with permission of www.USRA.ca)
(i)
The sciatic nerve is also expected to be found between the GT laterally and IT medially.
(j)
Scan the nerve proximally and distally to follow its course and confirm its identity.
(k)
If nerve visualization is difficult in the short axis, it is helpful to turn the patient prone and scan to visualize the sciatic nerve in long axis.
Needling
(l)
Ultrasound-guided subgluteal sciatic nerve block is considered an intermediate level block technique. The sciatic nerve in this region is often less deep compared to the gluteal and proximal thigh regions.
(m)
The subgluteal sciatic nerve block is amenable to both in-plane and out-of-plane approaches. The block requires a shorter needle, e.g., a 50- or 80-mm 22G insulated block needle, and a total volume of 15–20-mL volume of local anesthetic is used for postoperative analgesia.
(n)



Visualization of the sciatic nerve in this region can also be challenging because of the required depth of beam penetration and the attenuation of ultrasound energy by the overlying adipose tissue layers.
Related posts:






Full access? Get Clinical Tree
