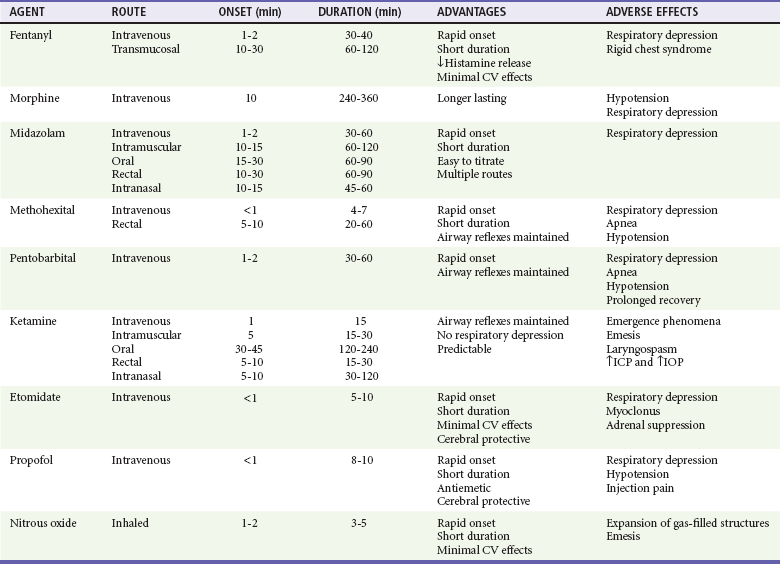
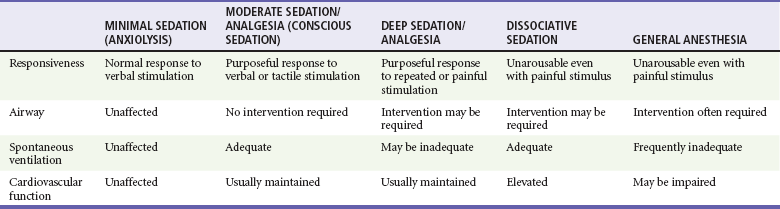
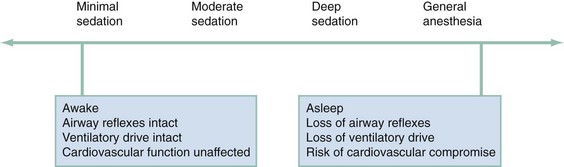
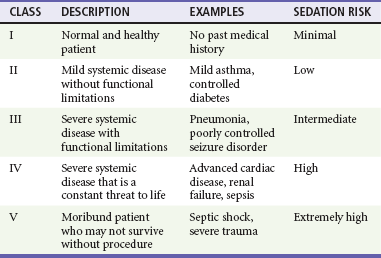
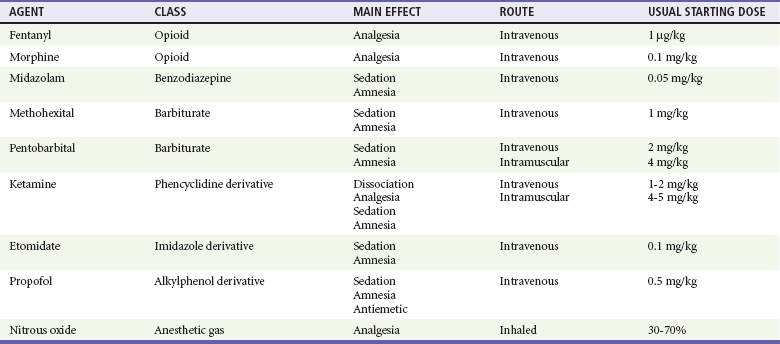
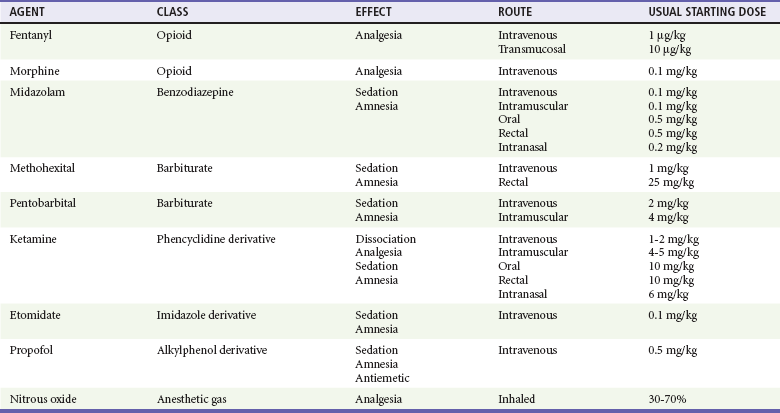
Chapter 4 The performance of painful diagnostic and therapeutic procedures is common in emergency care. Many of these are associated with significant anxiety, especially in children.1–5 Procedural sedation and analgesia (PSA) has therefore become a fundamental and required skill for emergency physicians and an integral part of the core training of emergency medicine residents.4–8 PSA improves the quality of patient care and satisfaction through relief of pain and anxiety and by facilitating the timeliness and success of therapeutic or diagnostic procedures.7,9–14 These include fracture or joint reduction, incision and drainage of abscesses, cardioversion, tube thoracostomy, lumbar puncture, complex wound repair, and imaging studies in young or uncooperative patients. Many of the agents used for PSA have the potential to cause significant respiratory, cardiovascular, or central nervous system (CNS) depression.15–25 The Joint Commission (TJC), the Centers for Medicare and Medicaid Services (CMS), the American College of Emergency Physicians (ACEP), and the American Society of Anesthesiologists (ASA) have produced expert consensus or evidence-based documents concerning its use26–28 (Box 4-1). Although significant controversy continues with respect to credentialing and oversight of PSA outside the operating room, the advent of these guidelines has led to PSA becoming a safe, common, and practical emergency department (ED) procedure.9,29 It has been further improved by the development of shorter-acting, more effective drugs and the use of noninvasive monitoring devices. Anxiolysis is a state of decreased apprehension concerning a particular situation in which the patient’s level of awareness does not change. Analgesia refers to the relief of pain without the intentional alteration of mental status, such as occurs in sedation. An altered mental state may be a secondary effect of the medications administered for this purpose. Dissociation is a trancelike cataleptic state induced by an agent such as ketamine and characterized by a profound analgesia and amnesia. Protective reflexes, spontaneous respirations, and cardiopulmonary stability are retained. Sedation is a controlled reduction of environmental awareness. Procedural sedation and analgesia is a technique of administering a sedative or dissociative agent, usually along with an analgesic, to induce a state that allows the patient to tolerate unpleasant procedures while maintaining adequate spontaneous cardiorespiratory function. It is intended to result in a depressed level of consciousness that allows the patient to maintain oxygenation and airway control independently and continuously. The drugs, doses, and techniques used are not likely to produce a loss of the protective airway reflexes.28 Prior terminology defined three levels of sedation: conscious sedation, deep sedation, and general anesthesia. The term conscious sedation was often misinterpreted, confusing, and imprecise. It was coined in 1985 to describe lightly sedated dental patients. It was then further incorporated into pediatric sedation guidelines to distinguish a level of sedation from which the patient is easily arousable from the more advanced techniques of deep sedation, in which patients are difficult to arouse, and general anesthesia, in which patients are not arousable.30–32 Despite the focused intent of these definitions, practitioners quickly labeled all levels of procedural sedation taking place outside the operating room as “conscious sedation.” In 2001 TJC adopted the ASA definition of sedation and analgesia that was created to better describe the continuum of sedation and analgesia33 (Fig. 4-1). Although this truly is a continuum, the ASA divided PSA into four distinct subgroups: minimal sedation, moderate sedation, deep sedation, and general anesthesia. A fifth category, dissociative sedation, has since been added34 (Table 4-1). This new nomenclature is more intuitive, clear, and logical. Minimal sedation (anxiolysis) is a drug-induced state during which patients respond normally to verbal commands. Although cognitive functions and coordination may be impaired, ventilatory and cardiovascular functions are unaffected. Moderate sedation/analgesia (formerly called “conscious sedation”) refers to a drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. Reflex withdrawal from the painful stimulus is not considered a purposeful response. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is always maintained. Dissociative sedation is a trancelike cataleptic state induced by the dissociative agent ketamine and characterized by profound analgesia and amnesia, while protective airway reflexes, spontaneous respirations, and cardiopulmonary stability are maintained. Deep sedation/analgesia describes a drug-induced depression of consciousness during which patients cannot be easily aroused but respond purposefully after repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained. General anesthesia is a drug-induced loss of consciousness during which patients are not arousable even with painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive-pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired. To date, no outcome-based studies have demonstrated clear benefit from extensive evaluation beyond vital signs, mental status, and airway and cardiopulmonary assessment before PSA.35,36 Despite this, consensus guidelines suggest that an increased risk of adverse events may exist in select subsets of patients. These include patients at the extremes of age, patients with difficult facial or neck anatomy or any other reason for potential intubation or bag-valve-mask ventilation difficulty, and patients with underlying significant disease states.15,16,25,36 A patient’s general physical status is conventionally categorized according to the ASA’s classification system37 (Table 4-2). Most practice guidelines require that a history and focused physical examination be performed and documented before PSA. There is no literature to support the need for routine diagnostic testing other than diagnostic testing driven by the patient’s current status, including comorbidities. The need for preprocedural fasting in PSA remains controversial.38–49 Currently the ASA recommends a period of 2 hours after ingestion of clear liquids, a period of 4 hours after ingestion of breast milk, and a period of 6 hours after ingestion of other liquids (infant formula, nonhuman milk) or solids before PSA, but there are no outcome studies to support these recommendations.50 These guidelines are based on expert consensus and extrapolated from data describing circumstances in which patients received sedation to the level of general anesthesia followed by the manipulation of the airway during intubation and extubation.20 PSA in the ED attempts to avoid both of these specific situations. Many studies fail to support the notion that gastric emptying has any effect on the incidence of complications or outcome with PSA. There have been no published studies demonstrating an increased risk of aspiration after a liquid or solid meal and no studies showing a benefit of fasting before PSA. In one large study of nearly 5000 children and 18,000 adults, no clinically significant differences with airway complications, emesis, or other adverse effects were observed between various groups of patients classified by their preprocedural fasting status.4,40 During PSA, the combination of vomiting and the loss of the airway protective reflexes is an extremely rare occurrence. Furthermore, most episodes of vomiting and aspiration occur during airway manipulation, which is also very unlikely to occur during PSA. TJC and most institutional policies suggest that PSA providers should have adequate training to administer the agents effectively and safely, the skills to monitor the patient’s response to the medications given, and the expertise needed to manage all potential complications.51–56 This generally implies that PSA in the ED should be supervised by an emergency physician or other appropriately trained and credentialed physician. It is also recommended that a qualified support person (nurse, respiratory therapist) be present for the continuous monitoring of the patient. Such support persons should focus on the patient’s status and not take part in the procedure. They should also be able to recognize and respond to the complications of PSA. They may assist with minor, interruptible tasks; however, they should have no other responsibilities that would interfere with the level of monitoring and documentation appropriate for the planned level of sedation. They should be free to monitor the patient from the start of the procedure through the completion of the recovery phase.28 PSA may result in an allergic reaction, oversedation, respiratory depression, or, rarely, cardiopulmonary arrest. The incidence of these complications depends on patient selection, the drugs used, the rate and dosage of administration, and specific patient sensitivities. Consequently, appropriate equipment to monitor the patient’s condition at all times; to manage airway complications, allergic reactions, and drug overdoses; and to treat respiratory or cardiopulmonary arrest should be readily available. Supportive equipment includes oxygen, suction, patient-monitoring devices, basic and advanced airway management equipment, a monitor/defibrillator, advanced life-support medications, reversal or rescue agents, and vascular access equipment (Box 4-2). The requirement for supplemental oxygen, and its benefits during PSA, have not been well studied and remain somewhat controversial.56–62 Supplemental oxygen may prevent hypoxemia in many patients; however, significant respiratory depression in these patients may not be detected because of their normal oxygen saturation. This may delay the recognition of respiratory compromise and hypercarbia when capnography is not used. On the other hand, transient hypercarbia is not harmful, and maintenance of adequate oxygen saturation is much more important. The use of capnography eliminates this issue, because ventilatory status is displayed continuously. We recommend the use of supplemental oxygen in administering PSA to a patient in the ED. The most important aspect of monitoring during PSA is the visual observation and assessment of the patient. The patient’s ability to follow commands in response to varied levels of stimulation is useful in quantifying the level of consciousness. Furthermore, the patient’s ventilatory rate may be readily assessed by direct observation, although depth of respiration (tidal volume) is much harder to estimate clinically. Other components of monitoring, which should be documented, include respiratory rate, heart rate, blood pressure, oxygen saturation, and perhaps cardiac rhythm and capnometry.63–67 Pulse oximetry is a reliable and important monitoring modality, used in conjunction with close and continuous observation of the patient and the response to medications and procedures. There is no evidence that cardiac monitoring during PSA is of any benefit, but it certainly is not harmful, is readily available, and is inexpensive to use.68–70 We recommend continuous electrocardiographic monitoring in older patients and in patients with a history of cardiovascular disease, hypertension, or dysrhythmia. In young healthy patients without underlying significant disease, this may be safely replaced by continuous pulse oximetry, which also displays the heart rate, but, in most circumstances, monitors capable of showing heart rate, blood pressure, and pulse oximetry will also easily facilitate cardiac rhythm monitoring. Capnometry or capnography measures end-tidal carbon dioxide (CO2) partial pressure and has been shown to detect cases of inadequate ventilation earlier than clinical assessment or detection of hypoxemia by oximetry.60,62,71–80 Several studies have demonstrated this, but none have shown an effect on clinical outcome to date. In July 2011, the ASA updated its procedural sedation standards to include capnography during moderate or deep sedation to evaluate the adequacy of ventilation in addition to continual observation of qualitative clinical signs.81,82 Capnography should be used when deep sedation is planned, as respiratory depression is common in patients undergoing deep sedation. It is optional when only light sedation is planned, but even in such cases, it will help the observer recognize unintended oversedation with respiratory depression. The Bispectral Index (BIS) is monitored via a noninvasive device attached to the patient’s forehead and derives a depth of sedation level via frontal lobe electroencephalographic measurements. It has been used in the operating room as an objective measure of sedation depth.83–85 Studies have shown that it may be beneficial in preventing oversedation in PSA and reducing the time to discharge.86 These investigations have also suggested that its use may better guide the depth of sedation endpoint than traditional sedation scales have, and it may have further benefit for PSA in children, as they frequently require deeper levels of sedation for prevention of movement.87–90 Early ED studies for its use in PSA to discriminate between mild-to-moderate and moderate-to-deep levels of sedation have not been reliable, nor has it been shown to be predictive of patients sedated to the point of general anesthesia from those with lesser degrees of sedation. BIS monitoring may have a beneficial role for emergency medicine use and PSA in the future but requires more investigation before its possible uses and benefits can be completely defined. The highest risk of serious adverse events generally occurs within 5 to 20 minutes of receiving the last dose of intravenous medication and at the completion of procedures, when the patient remains sedated but is no longer receiving the painful stimulus. Similarly, patients undergoing prolonged procedures in which deeper sedation is desired to reduce motion (e.g., magnetic resonance imaging [MRI]) are also at an increased risk.16–19,23,36,91 Patients should continue to be monitored closely at these times, and this should continue until clinical recovery has occurred. Before discharge, baseline cognitive and motor function should be achieved. The patient should be able to follow commands, speak clearly, and ambulate or sit unassisted (infants). Vital signs and respiratory status should be back to baseline and within normal limits. Residual pain should be addressed. Nausea should be minimal, and vomiting should be resolved. It is preferable that all patients, including adults, be sent home with a responsible adult, but if this is not possible, the patient remains in the ED until normal baseline has been achieved.4,92–96 Patients should be advised not to drive or participate in other dangerous activities for 12 to 24 hours. Despite the short clinical duration of most of the agents used, many people may exhibit subtle signs of cognitive deficits and mild drowsiness.94,97 It is therefore preferable that they remain in the company of a responsible adult at home for 4 to 8 hours. For children, light play at home should be the extent of activities, with no bicycle riding, swimming, or other complex motor activity until the next day. An antinauseant and progressive diet is helpful if nausea or vomiting is experienced. Standard discharge instructions should also be provided for the presenting complaint, and all patients should be instructed to immediately return if any confusion or respiratory symptoms arise. The specific agents for PSA and dosage recommendations for adult patients are provided in Table 4-3 and for pediatric patients in Table 4-4. Benefits and adverse effects are provided in Table 4-5. Individual agents are discussed in greater detail in the following sections. Table 4-5 Procedural Sedation and Analgesia Agents—Benefits and Adverse Effects CV, cardiovascular; ICP, intracranial pressure; IOP, intraocular pressure. Route of administration should also be determined by the procedure and the specific patient. In most situations, intravenous titration to the desired level of sedation and analgesia provides the safest, most rapid, and most predictable results. Drugs given by the intramuscular, oral, transmucosal, intranasal, or rectal route generally have a slower onset of action, are difficult to titrate, have unpredictable results, and may lead to prolonged sedation. These routes are virtually never used for PSA in adults. In children, however, ketamine has been shown to provide consistent and predictable results when given intramuscularly (IM).98–100 Nitrous oxide has predictable behavior when used as a sole inhalational PSA agent in children but is also frequently used as an analgesic adjunct to a sedating agent.101–104 In pediatric patients, the benefits of intravenous drug administration may be outweighed by the difficulty and distress to the patient in obtaining intravenous access. In this situation, drugs given by the alternative routes may be preferred. Drugs should be administered by titrated slow intravenous bolus to minimize hypotension or respiratory depression in many situations. It is important to allow adequate time between doses to achieve and assess peak effect before an additional dose is given. Lower initial doses should be chosen in sensitive patients or when drugs from multiple classes are being administered. One exception is ketamine. Unlike the other agents described, it possesses a threshold response rather than an additive dose-response continuum. Smaller doses of ketamine cause analgesia and disorientation. Dissociation occurs when a dosage threshold of 1 to 1.5 mg/kg IV in adult patients or 2 to 2.5 mg/kg in younger pediatric patients is reached. Higher doses do not enhance or deepen the sedation.105 Fentanyl has many advantages as an analgesic agent for PSA, given its rapid onset of action, short duration of activity, lack of histamine release, and favorable cardiovascular profile.62,106–110 Fentanyl rapidly crosses the blood-brain barrier and produces analgesia in as little as 90 seconds. Serum levels rapidly decline from peak concentrations because of extensive tissue uptake followed by hepatic metabolism. It has a duration of action of 30 to 40 minutes and a serum half-life of approximately 90 minutes. These properties permit the administration of multiple small doses that can be easily titrated to the desired clinical effect. Because fentanyl readily creates a reservoir in the adipose tissue, accumulated large doses may result in a progressively increasing duration of effect. This does not generally occur in doses less than 10 µg/kg.111–113 Respiratory depression is more likely at higher doses, when the drug is given rapidly, or when it is combined with other CNS depressants such as benzodiazepines or alcohol. Other side effects may include vomiting and pruritus, although these are less common than with other opioids. Hypotension and bradycardia are rare but may occur with high doses. Chest wall rigidity and glottic spasm, which may make ventilation difficult, are unique complications seen with high doses (anesthetic) of fentanyl given rapidly (generally more than 7 µg/kg).114 Many of these adverse effects may be readily reversed by naloxone. The exception to this is chest wall rigidity, which may not reliably be antagonized and may necessitate neuromuscular blockade and intubation to enable adequate ventilation. This complication is extremely rarely reported with the doses of fentanyl used for PSA.114 In children, oral or transmucosal fentanyl has been used widely as a premedication for anesthesia and intravenous placement. It has also been used for PSA when intravenous access is not feasible. This is generally in the form of a fentanyl-impregnated, sweetened matrix in lozenge form on a holder—the “fentanyl lollipop.” Transmucosal delivery allows rapid onset of action by avoiding first-pass metabolism in the liver. It has been shown to decrease activity and relieve pain in 10 to 30 minutes, resulting in scores similar to those after comparable intravenous doses of fentanyl.110,115,116 Despite this fairly rapid onset, transmucosal delivery does not allow for easy titration. The general dose is 10 to 15 µg/kg. Larger doses have been shown to cause more nausea and vomiting without improving analgesia or activity scores. The combination of transmucosal fentanyl and transmucosal midazolam has not been shown to have additional benefit over either agent used singularly for laceration repair in the ED and has been shown to increase adverse events.117 Its use before other agents such as propofol has not been studied well. The use of transmucosal fentanyl for PSA has largely been limited by unacceptable levels of nausea and vomiting, which approach 20 to 40% of patients.118 Benzodiazepines are potent amnestic, hypnotic, and anxiolytic medications. They also have anticonvulsant and purported muscle relaxant properties but do not have analgesic effects. Because of this, they are commonly coadministered with an analgesic agent such as fentanyl or morphine. They may be given IV, IM, orally (PO), intranasally (IN), or per rectum (PR) but are virtually always used IV for PSA in adults.119–121 Midazolam is the most commonly used agent because of its favorable pharmacokinetics. Midazolam has many advantages for PSA, given its rapid onset of action and short duration of activity compared with other benzodiazepines. Its amnestic properties also appear to be superior to many of the others.122 The starting intravenous dose is 0.05 mg/kg. Children may need slightly higher doses. Onset of sedation is generally within 1 to 2 minutes, and the duration of action is 30 to 60 minutes. Alternatives to the intravenous route are often used in children, particularly when sedation alone, without analgesia, is desired as for performance of a radiologic study. With intramuscular administration the same doses may be used, but the onset of action is delayed and the duration of effect is increased. Oral doses are often used in children, with a recommended starting dose of 0.5 mg/kg. Sedation is generally achieved within 30 minutes. Rectal administration may also be useful with doses of 0.5 mg/kg. The response when the drug is given by this route may be less predictable, and the rectal route is generally not accepted by older children. Intranasal administration may be useful but is irritating and often difficult in older children as well. The starting dose for this route is 0.2 mg/kg and results in sedation in 10 to 15 minutes. Of note, 1% of children younger than 5 years may experience a paradoxical reaction and become excited and agitated when given midazolam. If necessary, the agitated state is reversible by flumazenil. Midazolam has been shown to be an extremely safe and effective agent for PSA, both alone and when used in combination with fentanyl.123–125
Procedural Sedation and Analgesia
Perspective
Terminology
Approach to Procedural Sedation and Analgesia for Procedures
Preprocedural Fasting
Personnel
Supplies and Equipment
Monitoring
Discharge Criteria and Instructions
Pharmacology
Route of Administration
Fentanyl
Benzodiazepines
Midazolam

Full access? Get Clinical Tree


Procedural Sedation and Analgesia
Only gold members can continue reading. Log In or Register to continue



