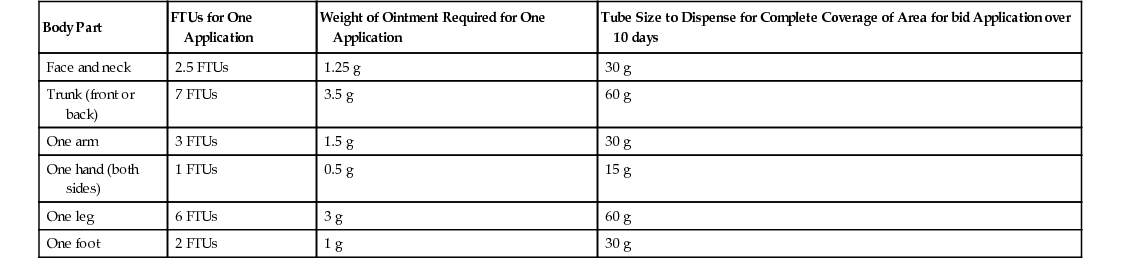
Kathryn K. Ellis, Kathryn R. Colcher The critical first step in treating any dermatologic condition is accurate diagnosis. Other important components are the type of lesion to be treated, the medication, the vehicle of the active medication, and the method used to apply the medication. A thorough history is the most important step in the assessment of dermatologic problems. In dermatologic therapy, the type of lesion guides therapy. Moist, weeping lesions are treated with Burow solution to hasten drying while providing soothing relief. Wet dressings are beneficial when treating exudative skin diseases because they help to suppress inflammation through vasoconstriction of superficial vessels as well as promote drying of lesions and wound debridement.1 In dry dermatitis, therapeutic agents incorporated into creams or ointments increase moisture in the skin and provide relief from pruritus. The skin is the largest organ of the body. The primary function of the skin is to provide a barrier to passage of substances into the body and to maintain internal homeostasis.2 Three main layers form this barrier.2 The stratum corneum is the most superficial section of the epidermis, or outer layer. The stratum corneum consists of enucleated keratinocytes, which are filled with keratin and an interfilamentous matrix. The middle layer is the vascularized dermis, which contains connective tissue and skin appendages. The innermost layer is the hypodermis, or subcutaneous layer, composed of adipose tissue. The thickness and permeability of the stratum corneum vary on different areas of the body. When the stratum corneum is irritated and inflamed, the protective skin barrier is interrupted. These characteristics have clinical implications for dermatologic therapy because they affect drug absorption. The skin structure in older adults is dryer, thinner, and less elastic, which needs to be considered in prescribing for the elderly population. Several variables affect the pharmacologic response when dermatologic agents are applied to the skin.2,3 The first variable is the regional variation in drug penetration, which is based on the thickness of the stratum corneum. There is an inverse relationship between the thickness of the stratum corneum and drug concentration. Therefore in areas such as the face, scalp, axilla, and scrotum, the stratum corneum is more permeable. There is also increased permeability when the skin is broken down by disease, trauma, and chemicals (soaps and detergents).2 In addition, the concentration of the dermatologic medication affects its absorption in the skin. Finally, because the principal transport mechanism is passive diffusion, increasing the concentration gradient increases absorption. Because of the physiology of the skin, the local half-life of a topical medication is extended to allow once-daily administration. In addition to the type of medication, important elements to include in topical prescription writing are the vehicle, concentration, amount, and application instructions.2 Consideration needs to be given to the size of the area to be treated, frequency of application, and expected time to healing. One gram typically covers an area of 10 × 10 cm; ointments cover a slightly larger area.2 For example, the amount needed for a single application for the entire body is approximately 30 g. Another practical way to measure topical application is the fingertip unit (FTU). A FTU is defined as the amount of ointment expressed from a tube with a 5-mm nozzle to cover from the tip of the index ringer to the distal skin crease. This is approximately 0.5 g.1 Table 40-1 contains additional information about the number of FTUs needed to treat a particular body part. Prescribing the appropriate amount of medication will prevent unnecessary cost, waste, and inconvenience to the patient. The base in which the active medication is delivered (the vehicle) affects the drug’s ability to permeate the skin. The vehicle may also provide important therapeutic effects to the skin, such as hydration. Drug absorption may be enhanced up to 10 times with the application of occlusive dressings. The most common vehicles are combinations of powders, oils, and liquids in varying proportions. Powders aid in absorbing moisture, decrease friction, and help cover wide areas. Oils provide an emollient function and, because of their occlusive properties, often enhance drug absorption. Liquids provide a cooling, soothing sensation by evaporation while helping exudative lesions to dry. With variations in skin thickness, body hair, and type of lesion, it is important to choose the most appropriate vehicle. Table 40-2 contains additional information. TABLE 40-2 Common Vehicles for Topical Pharmacotherapeutic Preparations
Principles of Dermatologic Therapy
Definition and Epidemiology
Skin Structure
Medications
Variables to Consider in Prescribing
Dermatologic Vehicles
Type of Preparation
Properties
Lotion
Cools and dries as it evaporates; useful for treating moist or pruritic skin.
Cream
Helps retain water; cosmetically appealing; useful in high-humidity environments; easily washed off.
Gel
Becomes liquid on contact; cosmetically appealing; avoid on acutely inflamed skin because alcohol base may cause stinging.
Ointment
Helps retain water, hydrating; avoid use in exudative, infected lesions; may be greasy; complications include folliculitis, maceration, and miliaria.
Emulsion
Water-in-oil preparation that is less occlusive than ointment.
Paste
Less greasy than ointment, with some drying action; good as protective barrier.
Wet dressing
Open
Anti-inflammatory action and vasoconstriction helpful in decreasing edema and removing crust; offers relief of pruritus through evaporation and cooling.
Closed
Retains heat and causes maceration.
Bath soaks
Temperature should be lukewarm, not hot; limit to 20-30 minutes; oils may make tub slippery.
Powder
Promotes drying; increases surface area; decreases maceration and moisture; avoid in open wounds.
Fixed
Proper application aids in decreasing edema; leave the dressing in place for 1 week, then remove by soaking in warm water. Related posts:

Full access? Get Clinical Tree


Principles of Dermatologic Therapy
Chapter 40