Fig. 62.1
Tibial and common peroneal (fibular) nerve in the popliteal area. (1) Iliotibial tract, (2) biceps femoris muscle, (3) semimembranosus muscle, (4) semitendinosus muscle, (5) gracilis muscle, (6) sartorius muscle, (7) gastrocnemius muscle, (8) common peroneal(fibular) nerve, (9) tibial nerve, (10) lateral sural cutaneous nerve (originates from peroneal nerve), (11) medial sural cutaneous nerve (originates from tibial nerve) (With permission from Danilo Jankovic)
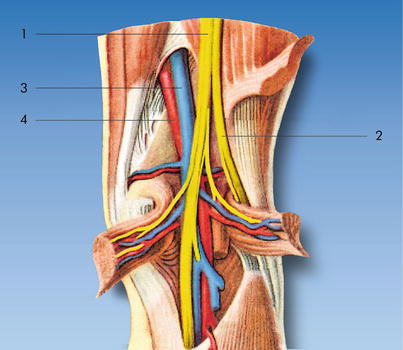
Fig. 62.2
Tibial and common peroneal (fibular) nerve in the popliteal fossa. (1) Tibial nerve, (2) common peroneal (fibular) nerve, (3) popliteal artery, (4) popliteal vein (With permission from Danilo Jankovic)
Tibial Nerve
The tibial nerve is the larger of the two sciatic divisions, being almost twice as thick as the common peroneal (fibular) nerve. It traverses the popliteal fossa lying posterior and slightly lateral to the popliteal vessels.
It then passes between the two heads of the gastrocnemius muscle to the upper edge of the soleus muscle, giving off the medial sural cutaneous nerve which unites with the lateral sural cutaneous nerve (a branch of the common peroneal nerve) to form the sural nerve. The tibial nerve continues distally between the posterior tibial muscle and the soleus muscle and runs together with the posterior tibial artery through the calf musculature, between the medial malleolus and the calcaneus, and to the medial side of the foot joint (Anatomy Fig. 62.3). It divides into its two end branches, the medial and lateral plantar nerves, behind the medial malleolus. These pass under the flexor retinaculum to the sole of the foot and provide it with its sensory innervation.
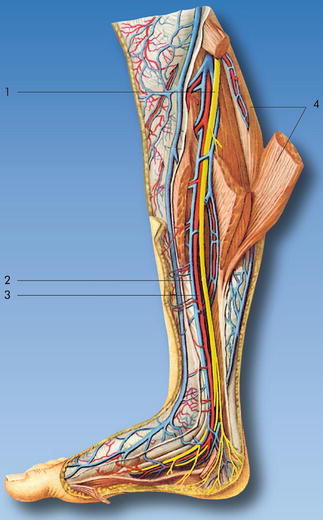
Fig. 62.3
The course of the tibial nerve through the leg and foot. It runs with the posterior tibial artery through the calf to lie behind the medial malleolus, where it divides into the medial and lateral plantar nerves. (1) Tibial nerve, (2) posterior tibial vein, (3) posterior tibial artery, (4) gastrocnemius muscle (With permission from Danilo Jankovic)
Common Peroneal (Fibular) Nerve
After separating from the tibial nerve, the common peroneal (fibular) nerve runs along the medial edge of the biceps femoris muscle over the lateral head of the gastrocnemius muscle to the lateral angle of the popliteal fossa. At the neck of the fibula, it passes to the lateral surface of the bone. Before entering the peroneus longus muscle, which originates here, it divides into the superficial peroneal nerve (which is mainly sensory innervation of the foot) and the deep peroneal nerve (mainly motor innervation of the foot).
Up to the point at which it divides, its small branches supply the short head of the biceps femoris muscle, the lateral and posterior parts of the joint capsule, and the tibiofibular joint.
The common peroneal nerve also gives off the lateral sural cutaneous nerve (Anatomy Fig. 62.1). The anterior branch of the lateral sural cutaneous nerve runs subcutaneously on the lateral surface of the lower leg as far as the lateral malleolus and supplies sensory innervation to the posterior and lateral aspects of the lower leg. Its posterior branch unites with the medial sural cutaneous nerve (branch of the tibial nerve) in the middle of the lower leg to form the sural nerve, although it can also occasionally continue as a separate branch as far as the lateral malleolus.
Sonoanatomy of the Sciatic Nerve in the Popliteal Fossa
The sciatic nerve is imaged by placing the ultrasound probe in a transverse orientation on the posterior aspect of the patient’s leg, in the popliteal fossa (Sonoanatomy Figs. 62.4 and 62.5). It is recommended that a systematic scan be performed starting at the level of the popliteal skin crease (where structures are most superficial) and moving proximally or cephalad (the traceback approach) [6]. On the lateral aspect of the image, the muscle bulk is made up of biceps femoris, and medially, the muscles of semitendinosus and semimembranosus (Sonoanatomy Fig. 62.6). The popliteal vessels are identified as dark hypoechoic circular structures and can be distinguished by the fact that the artery is pulsatile and the vein is compressible. Color Doppler can also be used for additional confirmation (Sonoanatomy Fig. 62.7). The hyperechoic tibial nerve is located superficial (posterior) to the popliteal vessels and is most commonly lateral to the vein. As the probe is moved proximally, the smaller common peroneal (fibular) nerve will be seen to move from the lateral aspect of the thigh toward the midline to join the tibial nerve to form the sciatic nerve within a common (paraneural) sheath (Sonoanatomy Fig. 62.8).


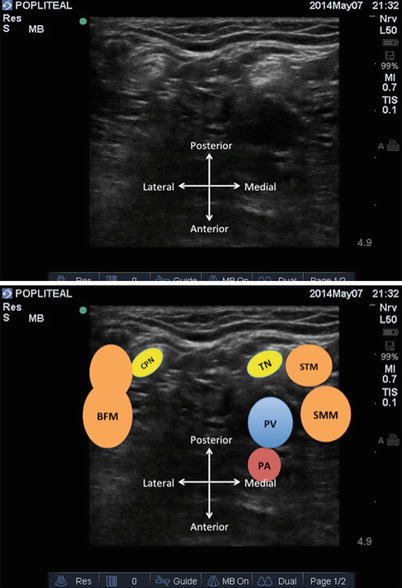
Fig. 62.4
Ultrasound probe position in the popliteal fossa with the patient in the supine position (With permission from Dr. Ki Jinn Chin)
Fig. 62.5
Ultrasound probe position in the popliteal fossa with the patient in the prone position (With permission from Dr. Ki Jinn Chin)
Fig. 62.6
Transverse view of the popliteal fossa and associated structures. The tibial nerve (TN) is located superficial to the popliteal artery (PA) and vein (PV). The common peroneal nerve (CPN) is visible lateral to the tibial nerve. BFM biceps femoris muscle, STM semimembranosus muscle, SMM semimembranosus muscle (With permission from Dr. Ki Jinn Chin)
Fig. 62.7
Color Doppler may be used to help identify the popliteal vein (upper image) and artery (lower image) (With permission from Dr. Ki Jinn Chin)
Fig. 62.8
Scanning the sciatic nerve in the popliteal fossa from distal to proximal using the traceback method. The positions of the ultrasound in Figs. a to d correspond to the positions indicated in the figure on the right side. The tibial nerve (nerve on the right side) and common peroneal nerve (nerve on the left side) of the sciatic nerve will be seen to approach each other and join within a common sheath (With permission from Dr. Ki Jinn Chin)
Clinical Pearls for Optimal Imaging of the Popliteal Sciatic Nerve
The neural structures are often more laterally positioned in the popliteal fossa than initially anticipated; bear this in mind with initial probe placement.
Use color Doppler to identify the popliteal vessels. Use minimal pressure initially to ensure that the popliteal vein is not occluded.
The traceback method allows you to identify the point at which the common peroneal (fibular) nerve unites with the tibial nerve to form the common sciatic nerve. Blockade at this point is ideal.
The tibial and common peroneal (fibular) nerves rarely lie in a parallel plane to the skin surface and are therefore usually poorly visible if the ultrasound probe is placed perpendicular to the skin surface. The probe will need to be tilted (often in a plantar direction) to a varying degree to increase the echogenicity and visibility of the nerves (a phenomenon known as anisotropy).
Technique: Landmark-Guided Approach (Single Shot)
Required Supplies and Equipment
Disinfectant solution and swabs for skin preparation
Sterile gloves and drapes
Short-beveled 22-G block needle with extension tubing
50–80 mm (posterior approach)
80–100-mm needle (lateral approach)
Local anesthetic of choice in 10- or 20-ml syringes
Lidocaine 1–2 % in 3-ml syringe with a 25–27-G hypodermic needle for skin infiltration (at operator’s discretion)
Equipment and supplies for managing life-threatening acute complications, including intralipid for local anesthetic systemic toxicity
Drugs for intravenous sedation during the block (at operator’s discretion)
Preparation of Patient
Obtain informed consent for the block.
Explain expected clinical course including care of the insensate limb and managing the transition to systemic analgesia.
Establish intravenous access, supplemental oxygen delivery, and standard monitors (ECG, noninvasive blood pressure, pulse oximetry).
Perform a time-out to confirm patient identity and site and side of surgery.
Block Performance
There are two main landmark-guided approaches that may be used.
1.
The posterior popliteal block
2.
The lateral popliteal block
Landmark-Guided Popliteal Nerve Block: Posterior Approach
Patient Position
The patient is placed prone with little to no flexion at the knees and in a neutral position—internal or external rotation at the hips should be avoided. This is done by placing a small soft roll under the ankles or by allowing the feet to dangle off the foot of the bed.
A right-handed operator should always stand on the left side of the patient, to allow use of the dominant hand for needling, and vice versa.
Surface Landmarks
Different methods of determining the appropriate needle insertion point have been described [7], but all are based upon the principle of targeting the sciatic nerve in the mid-thigh, proximal to its bifurcation into tibial and peroneal nerves.
The modified intertendinous approach [7] (LMG Fig. 62.9):
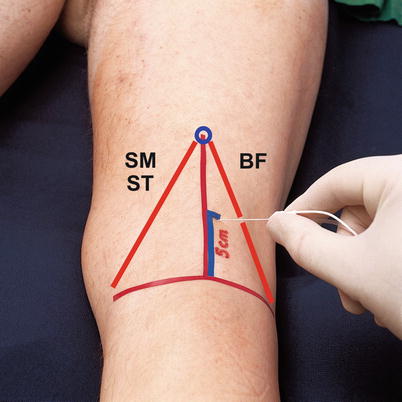
Fig. 62.9
Surface landmarks for the posterior approach to the popliteal nerve block. A transverse line between the lateral and medial epicondyles of the femur (corresponding approximately to the popliteal crease) is drawn and its midpoint marked. The upper borders of the popliteal fossa, formed by semimembranosus (SM), semitendinosus (ST), and biceps femoris (BF) muscles, are palpated and marked. There are two possible insertion points: (1) at the apex of the popliteal fossa (the modified intertendinous approach) or (2) at a point 5–7 cm cephalad and 1 cm lateral to the midpoint of the transverse line between femoral epicondyles (With permission from Danilo Jankovic)
Palpate the upper (cephalad) borders of the popliteal fossa, which are formed by the tendons and muscle bellies of the semimembranosus and semitendinosus (medial) and the biceps femoris (lateral). Identification of these landmarks can be facilitated by asking the patient to flex their knee against resistance.
Trace the borders to where they meet at the apex of the popliteal fossa—this is the site of needle insertion.
Alternative method (LMG Fig. 62.9):
Draw a transverse line between the lateral and medial epicondyles of the femur and mark its midpoint.
From a point 1 cm lateral to the midpoint of this first line, draw a second line perpendicular to the first one, extending 5–7 cm in a cephalad direction—this is the site of needle insertion.
Needle Insertion and Injection Technique
Disinfect the skin, drape the area appropriately, prime the block needle and tubing with local anesthetic solution, and attach a nerve stimulator at an initial current setting of 1–2 mA, pulse duration of 0.1–0.3 ms, and frequency of 1–2 Hz.
Fixing the skin over the skin insertion point with the second and third fingers of the nondominant hand, insert a 50–80-mm block needle at a 45–60° angle in a cephalad direction and parallel to the long axis of the leg (LMG Fig. 62.10).

Fig. 62.10
Needle insertion in the surface landmark-guided posterior approach to the popliteal nerve block. The needle is advanced at 45–60° angle in a cephalad direction until an appropriate motor response is obtained at 0.3–0.5 mARelated posts:

Full access? Get Clinical Tree








