Immediate Management of Life-Threatening Conditions
Establish and maintain an adequate airway and ventilation. Begin supplemental oxygen, 12 L/min, by nonrebreathing mask. If the patient has no gag reflex, intubate for airway protection, to facilitate oxygenation and to remove airway secretions. Continuously monitor oxygen saturation.
Obtain arterial blood for blood gas and pH measurements to determine adequacy of ventilation and perfusion.
Insert a large-bore (≥18-gauge) peripheral or central intravenous catheter, and draw blood for complete blood count, serum electrolyte and blood glucose measurements, and tests of renal and hepatic function.
Give glucose, 50 mL of a 50% solution (25 g of glucose) intravenously over 3–4 minutes, if a normal blood glucose cannot be determined immediately. If the patient’s response is weak or if narcotic overdose is suspected, as indicated by pinpoint pupils and shallow respirations, give repeated doses of naloxone 2 mg every 1–2 minutes up to a total dosage of 10–20 mg. Note: The duration of action of naloxone (2–3 hours) is shorter than that of many of the narcotics it reverses. Patients responding to naloxone must be observed for at least 3 hours after the last dose.
If alcoholism or malnutrition is suspected, give thiamine, 100 mg intramuscularly or in intravenous solution with or prior to glucose administration.
Maintain circulation, and treat shock by restoring intravascular volume with intravenous infusion of crystal-loid solutions. Caution: Fluid overload and pulmonary edema may occur with overly vigorous hydration. Some medications (salicylates) put patients at higher risk for pulmonary edema. If administration of more than 20–30 mL/kg of crystalloid solution and usual doses of dopamine (ie, 5–15 μg/kg/min intravenously) fail to restore blood pressure, insert a central venous catheter and arterial pressure catheter to obtain pressure readings and help guide further therapy with fluids or pressor agents.
If the patient is experiencing seizures, give diazepam, 0.1–0.2 mg/kg, or lorazepam, 0.05 mg/kg, intravenously. If this is not effective, within a few minutes, repeat the dose. If the seizures continue, administer phenobarbital, 20 mg/kg, intravenously over 20 minutes. Phenytoin is ineffective for stopping seizures caused by most poisonings.
Start cardiac monitoring. Obtain a 12-lead electrocardiogram (ECG) and note especially the rate; rhythm; presence of arrhythmias; and PR, QRS, and QT intervals. If overdose of tricyclic antidepressants is suspected, obtain serial ECGs.
Place a nasogastric or orogastric tube for the administration of activated charcoal. Activated charcoal may be premixed with a 70% solution of sorbitol. Activated charcoal, 1 g/kg, should be given to anyone who may have ingested a toxic substance within 1 hour prior to arrival (see section on decontamination below).
Look for other causes of coma or seizures. In particular, look for (1) head trauma (focal neurologic deficits or asymmetric seizures), (2) other trauma causing hemorrhage or shock, (3) infection (generalized or central nervous system), (4) metabolic disorders (hyponatremia, hypoglycemia, hyperglycemia), (5) hypothermia (use a rectal thermometer that can measure temperatures lower than 32°C [89.6°F]), or (6) hyperthermia.
Further Management of Victims of Poisoning
For assistance in identifying drugs and poisons and access to expert toxicologic consultation call your local poison center at 1-800-222-1222. Refer to http://www.aapcc.org for other local poison center listings. Experts at the poison center can (1) provide immediate assistance in selecting appropriate laboratory or toxicity tests and (2) in recommending preferred methods of gut decontamination, patient specific care recommendations, or the use of antidotes, and (3) advise on patient disposition.
Obtain as much information as possible from paramedics, bystanders, police, family, and friends. Ask about recent use of drugs or medications, and find out whether any empty pill bottles, medications, or drug paraphernalia were found at the scene. If several patients present with similar symptoms of poisoning, consider carbon monoxide poisoning, food poisoning, or other toxins that can affect multiple victims simultaneously including chemical and bioterrorism. Correlate the history with physical findings and results of laboratory tests, but do not be misled by the history. What the patient or friends say was ingested may differ from what was actually swallowed, especially in suicide attempts.
Remove the patient from the source of poison to fresh air and give oxygen by mask. Inhalation of a water aerosol may help to dilute inhaled irritants in the nasopharynx. Check for hoarseness and singed nasal hairs (eg, after smoke inhalation) and be alert for delayed development of upper airway obstruction or pulmonary edema.
Wash the eyes immediately with copious amounts of plain water or normal saline; do not use neutralizing solutions. Hang a bottle containing 500–1000 mL of normal saline above the patient, and dribble the solution slowly into the corner of the injured eye through the intravenous tubing.
If the contaminating material was acidic or basic, tears may be checked with pH paper after the eyes have been washed to make sure that all toxic material has been removed. A careful eye examination is indicated following irrigation.
Wash the skin immediately with plenty of water and dilute soap solution. Discard contaminated clothes in a marked plastic bag. Certain toxins, such as organophosphates, are well absorbed through the skin and are difficult to remove. Remove all particulate matter prior to irrigation. Health-care providers should take measures to avoid direct exposure with skin or clothes in an effort to prevent secondary contamination.
Hydrofluoric acid burns are particularly penetrating and corrosive. Following irrigation prompt application of 10% calcium gluconate gel to exposed areas is warranted. A secondary option is immersion of the burn into quaternary ammonium salt solution. Subcutaneous injection of calcium gluconate deep to the burn (0.5 mL of 10% solution per square centimeter of burn area)or intra-arterial calcium may be helpful. Monitor calcium levels closely. Contact a poison control center for additional recommendations. A plastic surgeon (or hand surgeon) should be consulted for injuries involving the fingers.
The traditional approach has been to remove ingested toxins by emesis or gastric lavage, followed by activated charcoal and catharsis. However, recent evidence suggests that gastric emptying may have limited efficiency, especially if initiated more than 1 hour after the ingestion, and may delay the administration of charcoal. Activated charcoal is the preferred method of gastric decontamination, particularly in patients who have taken a rapid-acting medication.
Induced emesis is no longer recommended.
Use gastric lavage in patients with suspected serious poisonings, who have a decreased level of consciousness, and who present to the emergency department within 1 hour of ingestion. Unless a patient is intubated, gastric lavage is contraindicated if airway protective reflexes are absent.
Gastric lavage is performed with a large-bore (at least 36F for adults) orogastric or nasogastric tube. (Pill fragments cannot be removed through standard-sized nasogastric tubes.) Use tap water or saline at body temperature in 250-mL increments, and continue lavage until fluid returns clear or free of pill fragments.
Activated charcoal, 50–100 g as a slurry, can be given if a patient has ingested a potentially toxic amount of most poisons. The administration of activated charcoal is contraindicated in those patients unable to protect their airway. Activated charcoal may be administered by nasogastric or orogastric tube following intubation for patients who do not have an intact airway. For oral administration, charcoal can be made more palatable by adding a small amount of cherry, licorice, or chocolate flavoring just before administration. Mixing the charcoal with 1 mL/kg of 70% sorbitol improves taste and also provides cathartic action. A cathartic should be limited to a single dose of activated charcoal in order to minimize diarrhea and dehydration. The effectiveness of activated charcoal decreases with time, and it will be ineffective for most substances if given more than 1 or 2 hours after the ingestion. Charcoal has great adsorptive properties and can bind most poisons (exceptions include caustics, hydrocarbons, alcohols, iron, lithium, lead, and potassium). If the ingested dose of poison is known, give at least 10 times that weight of charcoal, in divided doses if necessary.
Indications for whole bowel irrigation include large ingestion of sustained release products, large ingestion of chemicals not absorbed by charcoal (such as lithium), and ingestion of foreign bodies or drug-filled packets. This technique utilizes a balanced electrolyte polyethylene glycol solution (Colyte, GoLYTELY) to flush out the entire intestinal tract. It is given by nasogastric tube, 1–2 L/h (400–500 mL/min in children), until the rectal effluent is clear (3–5 hours or more).
Look for characteristic physical signs of various kinds of poisoning while immediate treatment measures are being started. Physical signs associated with specific poisons are listed in Tables 47–1 and 47–2.
|
| Toxidrome | Representative Agent(s) | Most Common Findings | Additional Signs and Symptoms | Potential Interventions |
|---|---|---|---|---|
| Opioid |
| CNS depression, miosis, respiratory depression |
| Ventilation or naloxone |
| Sympathomimetic |
| Psychomotor agitation, mydriasis, diaphoresis, tachycardia, hypertension, hyperthermia |
| Cooling, sedation with benzodiazepines, hydration |
| Cholinergic |
| Salivation, lacrimation, diaphoresis, nausea, vomiting, urination, defecation, muscle fasciculations, weakness, bronchorrhea |
| Airway protection and ventilation, atropine, pralidoxime |
| Anticholinergic |
| Altered mental status, mydriasis, dry/flushed skin, urinary retention, decreased bowel sounds, hyperthermia, dry mucous membranes | Seizures, dysrhythmias, rhabdomyolysis. Death may result from hyperthermia and dysrhythmias | Physostigmine (if appropriate) sedation with benzodiazepines, cooling supportive management |
| Salicylates |
| Altered mental status, respiratory alkalosis, metabolic acidosis, tinnitus hyperpnea, tachycardia, diaphoresis, nausea, vomiting | Low-grade fever, ketonuria. Death may result from pulmonary edema, cardiorespiratory arrest | MDAC, alkalinization of the urine with potassium repletion, hemodialysis, hydration |
| Hypoglycemia |
| Altered mental status, diaphoresis, tachycardia, hypertension | Paralysis, slurring of speech, bizarre behavior, seizures. Death may result from seizures, altered behavior | Glucose, containing solution intravenously, and oral feedings if able, frequent capillary blood for glucose measurement |
| Serotonin syndrome | Meperidine/dextromethorphan + MAOI, SSRI + TCA, SSRI/TCA/MAOI + amphetamine, SSRI overdose | Altered mental status, increased muscle tone, hyperreflexia, hyperthermia | “Wet dog shakes” (intermittent whole body tremor). Death may result from hyperthermia. | Cooling, sedation with benzodiazepines, supportive management, theoretical benefit—cyproheptadine |
Appropriate laboratory evaluation of the patient is determined, in part, by the patient’s clinical condition.
Obtain arterial blood gas to determine adequacy of ventilation and circulation. Draw blood for measurement of serum electrolytes, blood urea nitrogen, blood glucose, and serum osmolality. Calculate anion and osmolar gaps (Tables 47–3 and 47–4).
|
The osmolar gap (Δ Osm) is determined by subtracting the calculated serum osmolality from the measured serum osmolality. Calculated osmolality:  |
| Osmolar gap: ΔOsm = measured Osm – Calculated Osm |
Obtain an ECG and look for widened QRS complexes or QT intervals, atrioventricular block, ventricular tachyarrhythmias, or evidence of ischemia (Table 47–5).
| Sign | Examples of Causes |
|---|---|
| Prolonged QT interval |
|
| Prolonged QRS interval |
|
| Atrioventricular block |
|
| Ventricular tachyarrhythmias |
|
| Ischemic pattern or current of injury |
|
Obtain a chest X-ray to examine for pulmonary edema (caused by opioids, barbiturates, salicylates, ethchlorvynol, or corrosive chemicals) or infiltrates (due to aspiration of gastric contents, inhalation of certain metal fumes, or hydrocarbon aspiration). Obtain an abdominal X-ray to look for radiopaque pills or toxins (Table 47–6).
Obtain urine for toxicologic screening and routine analysis. Calcium oxalate crystals may be present with ethylene glycol poisoning. Occult blood in the urine may be indicative of myoglobinuria or hemolysis. Phenylpyruvic acid (eg, Phenistix) may be positive for phenothiazine or salicylate overdose in an alkaline urine.
Qualitative determination of the presence of drugs in the urine rarely provides information that alters therapy and is seldom helpful in the emergency department. Results of toxicologic studies may be useful in later confirmation of the diagnosis. It is more cost effective to save serum and urine samples in the laboratory and analyze them later only if necessary. For a few types of medication poisoning (eg, lithium, acetaminophen, digoxin), the blood or serum drug concentration may be valuable in determining the need for specific therapy. These specific drugs and their antidotes are discussed later in this chapter.
The rational management of drug overdose requires an understanding of the absorption, distribution, and elimination of the toxin. Most published kinetic parameters have been determined at normal doses, whereas pharmacokinetics in victims of large doses is often more complex.
Dissolution and absorption of toxin or gastric-emptying time may be altered in poisoned patients, so that the peak effects may be delayed (as occurs with anticholinergics). The gastrointestinal tract may be injured, allowing increased absorption of certain materials (eg, iron). If the finite capacity of the liver to metabolize a drug is exceeded, an increased amount of the drug may be delivered to the systemic circulation. If the concentration of the toxin in the bloodstream increases dramatically, protein binding may be saturated (eg, in salicylate poisoning), so that the fraction of free toxin increases. Circulatory insufficiency, hypothermia, and electrolyte and acid–base imbalance influence the metabolism and excretion of ingested drugs. Any of these factors may drastically alter normal kinetics and confuse calculations. Despite these limitations, pharmacokinetic principles may be useful in the management of drug overdose. Some terms commonly used in toxicology are defined below.
The half-life of a toxin is the time required to eliminate one half of the toxin from the body. This parameter is most meaningful for the many drugs (eg, barbiturates, theophylline) that exhibit first-order kinetics, in which a fixed percentage of the toxin is removed per unit of time. Other drugs (eg, alcohol) have zero-order kinetics, in which a fixed amount of toxin is removed per unit of time. In an overdose, pathways of elimination are often saturated, and first-order kinetic elimination is replaced by zero-order (fixed amount) elimination.
The volume of distribution (Vd) is the volume into which the toxin is distributed after absorption. If a drug is sequestered outside the blood and is highly tissue bound, it will have a large volume of distribution. Table 47–7 gives the volumes of distribution for several common drugs.
| Drugs with Large Volumes of Distribution | Drugs with Small Volumes of Distribution | ||
|---|---|---|---|
| Chlorpromazine | 10–20 L/kg | Acetaminophen | 0.8 L/kg |
| Haloperidol | 20–30 L/kg | Digitoxin | 0.5 L/kg |
| Amitriptyline | >40 L/kg | Ethanol | 0.6 L/kg |
| Imipramine | 10–20L/kg | Isoniazid | 0.6 L/kg |
| Digoxin | 6–10 L/kg | Lithium | 1.1 L/kg |
| Meperidine | 4 L/kg | Phenytoin | 0.6 L/kg |
| Methadone | 5 L/kg | Salicylate | 0.2 L/kg |
| Theophylline | 0.5 L/kg | ||
Clearance is the volume of plasma that can be cleared of toxin per unit of time. Clearance includes both renal and metabolic components, and the proportion that each contributes to total clearance is important. For example, a toxin may be 95% metabolized and 5% renally excreted, in which case doubling the renal clearance of the toxin will not significantly enhance its total elimination from the body.
Knowledge of these parameters is helpful when measures to increase drug elimination (eg, forced alkaline diuresis, hemodialysis, or hemoperfusion) are under consideration. For example, toxins with large volumes of distribution are present in only minute quantities in plasma and are not effectively removed by dialysis or diuresis. Measures to enhance elimination of drugs with rapid intrinsic clearance rates will not contribute significantly to the overall elimination rate.
The decision to use a specific therapy to improve drug elimination should be based on a rational understanding of the drug’s properties and the patient’s clinical condition. Most patients respond satisfactorily to appropriate supportive care. The risks, time, and expense involved in hemodialysis or hemoperfusion must be weighed against the possible benefits. In some patients, the severe potential toxicity of the poison warrants immediate hemodialysis (Table 47–8). With other poisons, dialysis is of no theoretic or proved benefit. Poison control center staff may be helpful in identifying those patients who may benefit from enhanced drug elimination.
|
Because many toxins are weak acids or bases, they can be ionized in solutions of varying pH. In the ionized state, they are less likely to cross cell membranes, and their reabsorption to the renal tubular epithelium is decreased. The clinical significance of these measures depends on the contribution of renal elimination to total body clearance. It is also important to consider the possible adverse effects of overhydration, alkalemia, or acidemia. Most studies have failed to show a significant improvement in the outcome of poisoning by either forced diuresis or by the production of acidemia or alkalemia.
However, weak acids such as salicylate and phenobarbital are more fully ionized in basic solutions, so that alkalizing the urine may serve to trap them in the tubular lumen, thus increasing excretion of the drug in the urine. Urine acidification is no longer recommended for any poisoning because it may promote myoglobinuric renal failure in patients with rhabdomyolysis.
During hemodialysis, toxin is removed from the blood into a dialysate solution across a semipermeable membrane. The toxin must be relatively water soluble and not highly protein bound. It should have a small volume of distribution and slow rate of intrinsic elimination (ie, a long half-life). Hemodialysis is effective in removing methanol, ethylene glycol, salicylates, and lithium, among other drugs (see Table 47–8). It is also of value in correcting pH and electrolyte imbalances, especially in anuric patients.
This method is much less efficient than hemodialysis in removing most drugs.
In hemoperfusion, blood is pumped through a column of adsorbent material (charcoal or resin) and returned to the patient’s circulation. Vascular access similar to that for hemodialysis is required. The kinetic conditions required are the same as in hemodialysis; that is, the drug should have a small volume of distribution and a slow rate of intrinsic clearance. Hemoperfusion has the advantage that the drug or toxin is in direct contact with the adsorbent material; therefore, high molecular weight, poor water solubility, and even plasma protein binding are not limiting factors as they are in hemodialysis. Hemoperfusion is commonly associated with thrombocytopenia. Hemoperfusion will not correct pH or electrolyte imbalances.
Repeated doses of charcoal given orally or via gastric tube (20–30 g every 3–4 hours without a cathartic) may enhance elimination of some drugs and toxins from the bloodstream by interrupting enterohepatic or enteroenteric recirculation of the toxic. Drugs for which this may be useful are quinine, aminophylline, phenobarbital, nadolol, carbamazepine, and dapsone.
Recently, successful case reports have been documented in humans with the use of lipid infusion in significant local anesthetic toxicity. A 20% lipid infusion has been used to resuscitate a patients from cardiac arrest following the use of anesthetics. Some have postulated that this treatment could be used for many other fat soluble medication poisonings such as calcium channel blockers.
Table 47–9 sets forth several common useful antidotes. Their indications and dosages are discussed below in the sections on specific toxins. The half-life of the antidote relative to that of the toxin must be considered. Most important, antidotes should not be used indiscriminately and without regard for the patient’s clinical condition. They may have serious adverse effects and in some cases may be more toxic than the poison. Note: Always treat the specific symptoms manifested by the patient, not those known to be associated with a certain poison or by history alone.
| Poison | Specific Antidote |
|---|---|
| Acetaminophen | Acetylcysteine |
| Anticholinergics | Physostigmine |
| Anticholinesterases (organophosphates, carbamates, physostigmine) |
|
| Benzodiazepines | Flumazenil |
| β-Blockers | Glucagon |
| Calcium channel blockers | Calcium |
| Carbon monoxide | 100% Oxygen |
| Cyanide | Sodium nitrite |
| |
| Digoxin | Digoxin-specific antibodies |
| Heavy metals | Chelating agents |
| Isoniazid | Pyridoxine (vitamin B6) |
| Methanol, ethylene glycol | Ethanol, folate, 4-methyl pyrazole (not approved for use in the United States) |
| Narcotics | Naloxone |
| Tricyclic antidepressants | Sodium bicarbonate |
Management of Conditions Associated with Poisoning
It is essential to protect the lungs from aspiration and maintain adequate ventilation and oxygenation.
In the patient with a depressed gag reflex, gastric lavage and administration of activated charcoal may result in significant aspiration. Endotracheal intubation should always be performed in these patients, especially before gastric lavage. Charcoal should be administered through an orogastric or nasogastric tube.
Activated charcoal may be administered and gastric lavage may be performed without special precautions.
The lethargic patient with fluctuating mental status and a variable gag reflex poses a more difficult problem in management. If the gag reflex is intact, cautious gastric lavage may be performed with the patient in the left lateral decubitus position and with the head of the bed or stretcher tilted down at an angle of 10–20°. Note: If there is any doubt about the patient’s ability to protect the airway with a gag or cough reflex, charcoal administration and gastric lavage must be preceded by intubation with a cuffed endotracheal tube.
If intubation is not immediately performed, it is critical to monitor the status of the airway closely and to position the patient so as to preserve aspiration. An initially responsive patient may rapidly become more obtunded. Significant swelling and upper airway obstruction may be late developments after thermal, chemical, or caustic burns.
Management of drug-induced seizures is generally the same as that for seizures due to other causes, that is, protection of the airway; use of anticonvulsants; and correction of acidosis, hypoxemia, electrolyte abnormalities, and hyperthermia. Seizures unrelated to poisoning may also occur as a result of intracranial bleeding from trauma, hypoglycemia, or hyponatremia. Seizures caused by poisoning are rarely focal, nor are they associated with asymmetric neurologic findings. Meningitis may mimic metabolic or toxic encephalopathy and must be ruled out by lumbar puncture.
In certain types of poisoning, refractory seizures may require specific therapy:
Seizures occurring as a result of theophylline, lithium, or salicylate overdose usually require hemodialysis or hemoperfusion to accelerate removal of the drug.
In isoniazid poisoning with seizures refractory to diazepam, administer pyridoxine, 5 g (or 1 g per gram of isoniazid ingested) intravenously.
Seizures due to organophosphate poisoning may respond to atropine and pralidoxime. (See Organophosphates & Other Cholinesterase Inhibitors section, below.)
Seizures due to anticholinergics that are refractory to conventional therapy may respond to physostig-mine, 0.5–2 mg slow IV push.
Hypotension is a common associated condition in victims of poisoning. The mechanism of hypotension may be direct cardiac depression, peripheral vasodilation, or fluid defects or shifts that result in hypovolemia. Concurrent hypothermia may aggravate hypotension. Be alert for possible concurrent trauma with occult internal bleeding or concurrent infection with septic shock.
In the absence of associated pulmonary edema, a fluid challenge should be given with intravenous boluses of 1 L of normal saline. A central venous or pulmonary artery catheter may need to be inserted to monitor fluid needs and response to therapy in cases of refractory hypotension. Monitoring of urine output with an in-dwelling catheter is recommended. If hypotension and hypoperfusion are severe and unresponsive to administration of fluids and temperature correction, vasopressors may be of benefit.
Many drugs cause hyperthermia, either by direct toxic effects on temperature-regulating mechanisms or through associated hyperactivity or seizures.
Salicylate intoxication causes hyperthermia by uncoupling of oxidative phosphorylation, resulting in inefficient (and therefore heat generating) production of ATP.
Phenothiazines inhibit the autoregulatory ability of the central nervous system, leading to environmentally induced hypothermia or hyperthermia.
Hyperthermia may result from seizures or extreme hyperactivity (particularly if the patient has to be forcibly restrained) following poisoning by phencyclidine (PCP), cocaine, or amphetamines.
The anticholinergic properties of many drugs (eg, antihistamines, tricyclic antidepressants) can aggravate hyperthermia by inhibiting sweating.
For dangerous core temperatures above 41°C (105.8°F), cool the patient rapidly by sponge bathing with evaporation accelerated by fanning and ice packs; treat seizures. Muscular hyperactivity is most effectively treated with benzodiazepines or neuromuscular paralysis and assisted ventilation.
Hypothermia may be caused by certain drugs, exposure to cold, hypoglycemia, sepsis, or hypothyroidism. The diagnosis may be missed if a rectal thermometer capable of reading temperatures in the range of 24–32°C (75.2–89.6°F) is not used.
For severe hypothermia, rapidly restore normal body temperature with warm intravenous fluids, warm gastric or peritoneal lavage, or ventilation with warmed, humidified air. Slow passive rewarming by external means is usually sufficient in milder cases.
Initial evaluation may fail to reveal the seriousness of poisoning with some drugs. Severe, potentially preventable hepatic damage may occur after acetaminophen overdose unless the physician determines acetaminophen levels and administers the antidote N–acetylcysteine, when appropriate, early in treatment. Other poisons with characteristically delayed severe toxicity are listed in Table 47–10.
| Poison | Delayed Effect |
|---|---|
| Acetaminophen | Hepatic necrosis |
| Amanita mushrooms | Hepatic necrosis |
| Carbon tetrachloride | Hepatic and renal damage |
| Methanol | Blindness |
| Paraquat | Pulmonary fibrosis |
| Super-warfarins | Bleeding |
| Thallium | Peripheral neuropathy, hair loss |
| Ethylene glycol | Renal failure |
The development of sustained-release preparations has increased the chances of nearly normal results on initial evaluation. The possibility that a sustained-release preparation has been used must be considered in theophylline or salicylate poisoning, because with these drugs, serum or blood concentrations are used to evaluate the severity of intoxication. Under these circumstances, it is prudent to observe the patient longer and obtain a second blood-level reading before deciding on further treatment and disposition.
Emergency Treatment of Specific Poisonings
- Patient may be asymptomatic early after acute ingestion or present with anorexia, nausea, and right upper quadrant pain
- Draw 4-hour postingestion levels, and use the nomogram (Figure 47–1) to predict severity following acute ingestion
- – Chronic toxicity should be assessed through clinical examination, an acetaminophen level, and liver function tests
- – N-Acetylcysteine (NAC) therapy is antidote if indicated
- – Chronic toxicity should be assessed through clinical examination, an acetaminophen level, and liver function tests
Figure 47–1.
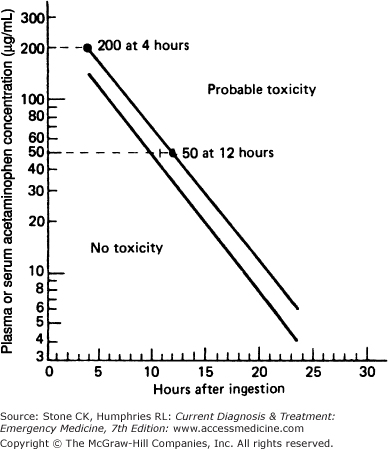
Nomogram for prediction of acetaminophen hepatotoxicity following acute overdosage. The upper line defines serum acetaminophen concentrations known to be associated with hepatotoxicity. The lower line defines serum levels 25% below those expected to cause hepatotoxicity. To give a margin for error, the lower line should be used as a guide to treatment. (Modified and reproduced, with permission, from Rumack BM, Matthew M: Acetaminophen poisoning and toxicity. Pediatrics 1975;55:871.)
Acetaminophen is a widely used ingredient in numerous over-the-counter and prescription preparations. One of the products of the normal metabolism of acetaminophen is hepatotoxic; at toxic levels, it saturates the glutathione detoxification system in the liver and accumulates, causing delayed hepatic injury (24–72 hours after ingestion). The toxic dose of acetaminophen is considered to be over 150 mg/kg in children and seven gin adults.
Caution: Shortly after ingestion of acetaminophen, there may be no symptoms or only anorexia, vomiting, or nausea; hepatic necrosis may not become clinically apparent until 24–48 hours later, when nausea, vomiting, abdominal pain, jaundice, and markedly elevated results on liver function tests may appear. Hepatic failure may follow.
Provide intensive supportive care and gastrointestinal decontamination as described previously. Administer activated charcoal regardless of the possibility that N–acetylcysteine may be administered.
Obtain a 4-hour postingestion acetaminophen serum concentration measurement, and use the Rumack-Matthew nomogram (see Figure 47–1) to predict the range of severity. If the 4-hour level is over 150 μg/mL, begin treatment with N–acetylcysteine. Because acetaminophen and salicylate are often ingested simultaneously, a measurement of serum salicylate concentration should also be obtained immediately. The nomogram is not helpful in determining the need for N-acetylcysteine for sustained-release product or chronic ingestions. If a sustained-released product has been ingested, two serum acetaminophen levels should be obtained 4–6 hours apart and treatment given if either level is above the possible toxicity line. For chronic toxicity or for those patients who present after 24 hours postingestion, treatment is based on clinical effects, liver function tests, and the acetaminophen level.
N–acetylcysteine substitutes for glutathione and binds the toxic metabolite of acetaminophen, thus inactivating and detoxifying it. It is available in both oral and intravenous dosage forms. Both the oral and intravenous routes have been demonstrated in multiple studies to be effective. Give 140 mg/kg orally of a 10 or 20% solution diluted to 5% with citrus juice or soda. Follow with 70 mg/kg orally every 4 hours for 72 hours. If the patient vomits a dose within 1 hour, it should be repeated; slow drip by nasogastric tube and administration of an antiemetic (eg, metoclopramide, 10–20 mg intravenously) may be helpful. Intravenous N-acetylcysteine dosing is 150 mg/kg in 200 mL of 5% dextrose for over 15 minutes. Maintenance dosing is 50 mg/kg in 500 mL of 5% dextrose over 4 hours followed by 100 mg/kg in 1-L 5% dextrose infused over 16 hours. Anaphylactoid reactions have been reported with the use of intravenous N-acetylcysteine.
To be effective, N–acetylcysteine must be given within 12–16 hours of ingestion of acetaminophen and preferably within 8 hours. Do not delay treatment if a serum acetaminophen level is not readily available and a toxic dose may have been taken. Treat with N-acetylcysteine empirically and reevaluate treatment after the acetaminophen level has returned. N-Acetylcysteine can also be safely given in pregnancy.
Use serum concentration of acetaminophen as a guide to the severity of poisoning, and hospitalize all patients requiring acetylcysteine therapy and those with evidence of hepatotoxicity.
- All drugs in this class are central nervous system stimulants
- Predominant symptom is sympathetic hyperactivity
- Treatment is supportive; no specific antidote is available
Amphetamines and other stimulants are easily abused because of their wide availability, primarily through street sales. Illicitly obtained stimulants frequently contain methamphetamine and may also contain PCP.
All of these drugs are central nervous system stimulants and cause sympathetic hyperactivity. Some may produce significant vasoconstriction causing hypertension. Most of these drugs have short half-lives and their peak effect and toxicity occur within 30 minutes after intravenous or intramuscular administration and 2–3 hours after oral ingestion. As a result, serum drug level measurements are of little value, and measures to enhance elimination generally do not alter the outcome.
Significant amphetamine poisoning is always accompanied by symptoms. Euphoria, mydriasis, and restlessness progress in severe cases to toxic psychosis and seizures. Hypertension can be severe and associated with palpitations or arrhythmias. Seizures and hyperthermia may produce rhabdomyolysis and myoglobinuria.
Provide intensive supportive care and gastrointestinal decontamination as described previously. For severe agitation or psychotic behavior, diazepam (5–10 mg in adults and 0.1–0.2 mg/kg in children) or lorazepam (2–4 mg in adults and 0.05–0.1 mg/kg in children) intravenously may be helpful; repeat every 5–10 minutes until sedation has been achieved.
Treat seizures with diazepam (5–10 mg in adults and 0.1–0.2 mg/kg in children) or lorazepam (2–4 mg in adults and 0.05–0.1 mg/kg in children) intravenously. May repeat every 5–10 minutes until seizures have ended. If seizures continue, administer phenobarbital (20 mg/kg intravenously over 20 minutes).
Hypertension is generally transient and, unless severe, does not require treatment. Often the hypertension responds to benzodiazepine administration, but in severe cases (eg, diastolic blood pressure > 120 mm Hg, encephalopathy), intravenous nitroprusside, 0.5–1.0 μg/kg/min, is effective and easily titratable. Phentolamine, 0.1 mg/kg slowly intravenously, is an alternative drug.
Tachycardia and ventricular tachyarrhythmias rarely require treatment but may respond to administration of propranolol, 0.05–0.1 mg/kg intravenously.
Monitor temperature and start cooling measures if hyperthermia occurs. Check the urine for myoglobin. Acidification of the urine is not recommended.
If chest pain is present, perform an ECG and check for cardiac enzymes, and consider hospitalization to rule out myocardial ischemia or infarction. Patients with seizures may require computed tomography (CT) scanning to rule out intracranial hemorrhage.
Hospitalize patients with complications (psychotic behavior, hypertension, hyperthermia, chest pain, and arrhythmias) or those with prolonged symptoms.
- Ingestion produces many symptoms prompting the phrase “blind as a bat, hot as Hades, red as a beet, dry as a bone, and mad as a hatter”
- Treatment is primarily supportive, although physostigmine can be used in life-threatening situations
Atropine, scopolamine, belladonna, many antihistamines, tricyclic antidepressants, and many plants (eg, jimsonweed [Datura stramonium], nightshade, Amanita muscaria mushrooms) have anticholinergic effects.
These drugs block cholinergic receptors both centrally and peripherally. Ingestion of a significant amount of an anticholinergic drug can produce many clinical effects. The popular phrase “blind as a bat, hot as Hades, red as a beet, dry as a bone, mad as a hatter” describes many of the manifestations of anticholinergic toxicity. Other signs and symptoms include tachycardia, gastrointestinal ileus, urinary retention, seizures, delirium, and hallucinations.
Provide intensive supportive care and gastrointestinal decontamination as described previously. Most patients can be managed with supportive measures alone, including sedation with benzodiazepines, cooling, and bladder emptying. If a patient develops life-threatening complications of anticholinergic toxicity (hemodynamically significant tachycardia, hyperthermia, or seizures resistant to benzodiazepines) that is refractory to conventional therapy, physostigmine, 1–2 mg intravenously over 2 minutes, can be given. Physostigmine works within minutes and the duration of effect is 30–60 minutes. It has been associated with severe complications, including bradycardia, heart block, and seizures. Atropine should be readily available if the antidote is used, and ECG monitoring is necessary. Physostigmine is contraindicated in patients with an overdose of tricyclic antidepressants.
Hospitalize patients who have incapacitating signs or symptoms of anticholinergic poisoning.
- Average toxic dose is 5 mg/kg
- Anticholinergic symptoms range from mydriasis, agitation, and tachycardia to seizures and coma
- Cardiovascular manifestations are often lifethreatening and include QRS widening, profound hypotension, atrioventricular blocks, and ventricular arrhythmias
Major tricyclic antidepressants include amitriptyline (Elavil, many others), imipramine (Tofranil, many others), and doxepin (Adapin, Sinequan). Maprotiline (Ludiomil) is a tetracyclic antidepressant with similar properties.
The tricyclic antidepressants are analogs of phenothiazines, with complex effects, including anticholinergic, α-adrenergic-receptor blocking, and quinidine-like activity on the heart. They are well absorbed and highly tissue bound, with volumes of distribution of 10–40 L/kg. These drugs are eliminated primarily by metabolism in the liver, and the half-lives are 10–30 hours. The average toxic dose is more than 5 mg/kg, with severe poisoning occurring at doses of 10–20 mg/kg.
Other antidepressants include the selective serotonin reuptake inhibitors (SSRI): fluoxetine, paroxetine, sertraline, citralopram and escitralapam. Other antidresssants include serotonin/norepinephrine reuptake inhibitors (SNRI) (venlafaxine and duloxetine), buproprion (norepinephrine and dopamine reuptake inhibitor) and the antidepressant sedative trazodone.
The hallmark of tricyclic antidepressant toxicity is the rapid onset of life-threatening clinical effects. Many symptoms are the result of the anticholinergic activity of these drugs, for example, mydriasis, dry mouth, tachycardia, agitation, and hallucinations. The onset of coma may be rapid, even precipitous. Twitching and myoclonic jerking have been noted, and seizures occur frequently and may be difficult to treat.
Cardiovascular manifestations are the most dramatic and life-threatening (Figure 47–2). Quinidine-like slowing of conduction is reflected by widening of the QRS complex (>100 ms) and prolonged QT and PR intervals. Varying degrees of atrioventricular block and ventricular tachycardia are common. Atypical (torsades de pointes) ventricular tachycardia may occur. Profound hypotension resulting from decreased contractility and vasodilatation may occur and is a frequent cause of death. Hypoxemia and acidosis aggravate the cardiovascular toxicity of tricyclic antidepressants.
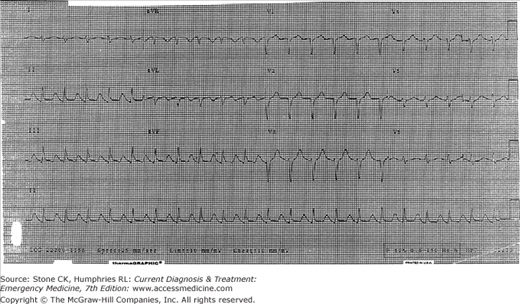
Diagnosis is generally based on history, relevant physical findings, widened QRS complexes, and prolonged QT intervals (3 Cs: c ardiac abnormalities, c onvulsions, and c oma). The diagnosis may be confirmed by qualitative or quantitative tests for these drugs in the blood or urine. Plasma concentrations are rarely available and often lack sensitivity in detecting active metabolites. Prolongation of the QRS complex or the terminal axis in lead aVR is a better predictor of severity of poisoning than is the drug concentration.
Some cyclic antidepressants (amoxapine) and antipsychotics (loxapine) can cause seizures and coma without associated cardiovascular toxicity or electrocardiographic changes.
The SSRIs in combination with other serotonergic drugs, or when taken alone, may lead to the development of some degree of serotonin syndrome. Ingestion of the SNRI antidepressants as well as buproprion, may cause seizures.
Provide intensive supportive care and gastrointestinal decontamination as described previously. Do not induce emesis because of the well-established risk of seizures and coma. Administer activated charcoal if the patient has ingested a toxic amount and is seen within 1 hour. Consider multidose charcoal for symptomatic patients.
Constant monitoring of the ECG for at least 6 hours is mandatory. Progressive widening of the QRS complex indicates worsening toxicity.
Treat seizures with diazepam or phenobarbital. Do not use physostigmine to treat seizures, because it may cause seizures and other complications.
Sinus tachycardia is benign and usually does not require treatment. Physostigmine and propranolol may aggravate conduction abnormalities and should not be used.
Ventricular arrhythmias and conduction defects may respond to sodium bicarbonate, 50–100 mEq (1–2 mEq/kg) as an intravenous bolus. It is not clear whether the improvement is merely a result of correction of acidosis, a result of transient hypernatremia, or a result of a shift in the protein binding of the drug with alkalosis. Lidocaine, 1–2 mg/kg as an intravenous bolus, is frequently effective. Quinidine-like drugs (eg, quinidine, procainamide, and disopyramide) are contraindicated, because they worsen cardiotoxicity.
Treat hypotension initially with intravenous infusion of sodium bicarbonate, 50–100 mEq (1–2 mEq/kg), and crystalloid solutions. If the patient fails to respond after 1–2 L have been infused, further therapy should be guided by measurement of pulmonary artery wedge pressures and cardiac output. Norepinephrine and epinephrine have been found to be more effective than dopamine in refractory hypotension.
Hemodialysis and hemoperfusion have no role in tricyclic antidepressant poisoning.
Hospitalize all symptomatic patients with overdose of tricyclic antidepressants. Use serial ECGs along with the patient’s clinical appearance to predict impending toxicity. Observe asymptomatic patients for a minimum of 6–8 hours, taking repeated measurements of the vital signs and QRS interval.
Related posts:






Full access? Get Clinical Tree


