65 Pleural Disease and Pneumothorax
 Radiologic Signs of Pleural Disease in the Intensive Care Unit
Radiologic Signs of Pleural Disease in the Intensive Care Unit
Pleural Fluid
Standard Chest Radiograph
In healthy humans in the supine position, the radiolucency of the lung base is equal to or greater than that in the lung apex.1 Furthermore, when in the supine position, breast and pectoral tissue tend to fall laterally away from the lung base, so an effusion should be suspected if there is increased homogeneous density over the lower lung fields compared to the upper lung fields. As the pleural effusion increases, the increased radiodensity involves the upper hemithorax as well. However, failure of chest wall tissue to move laterally, cardiomegaly, prominent epicardial fat pad, and lung collapse or consolidation may obscure a pleural effusion on a supine radiograph. Patient rotation or an off-center x-ray beam can mimic a unilateral homogeneous density. An absent pectoral muscle, prior mastectomy, unilateral hyperlucent lung, scoliosis, previous lobectomy, hypoplastic pulmonary artery, or pleural or chest wall mass may lead to unilateral homogeneous increased density and mimic an effusion.
Approximately 175 to 525 mL of pleural fluid results in blunting of the costophrenic angle on an erect radiograph.2 This quantity of effusion can be detected on a supine radiograph as an increased density over the lower lung zone. Failure to visualize the hemidiaphragm, absence of the costophrenic angle meniscus, and apical capping are less likely to be seen with effusions of less than 500 mL.1 The major radiographic finding of a pleural effusion in a supine position is increased homogeneous density over the lower lung field that does not obliterate normal bronchovascular markings, does not show air bronchograms, and does not show hilar or mediastinal displacement until the effusion is massive. If a pleural effusion is suspected in the supine patient, ultrasonography should be performed.
Other Radiographic Imaging
Sonography
Ultrasonography (US) provides good characterization for pleural diseases and is a useful diagnostic modality for critically ill patients who cannot be transported for computed tomography (CT). US takes less time and is less expensive than CT, can be done at the bedside, and can be repeated serially. Disadvantages include hindrance of the ultrasonic wave by air, either in the lung or pleural space, a restricted field of view, inferior evaluation of the lung parenchyma compared to CT, and operator dependence. US was helpful in diagnosis in 27 (66%) of 41 patients and treatment in 37 (90%) of 41 patients, and had an important influence on treatment planning in 17 (41%) of 41 critically ill patients.3
US has also been demonstrated to be a useful modality to guide bedside thoracentesis in the mechanically ventilated patient, resulting in high success rate and excellent safety of the procedure.4
Pneumothorax
When supine, pneumothorax gas migrates along the anterior surface of the lung, making detection on the anteroposterior radiograph problematic. The base, lateral chest wall, and juxtacardiac area should be carefully visualized for evidence of pneumothorax. Accumulation of air along the mediastinal parietal pleura may simulate pneumomediastinum.5 An erect or decubitus (suspected hemithorax up) radiograph should be obtained to assess for the presence of a pneumothorax. US is sensitive for the detection of pneumothorax by determining the presence or absence of “lung sliding.”6 In individuals without pneumothorax, the lung–chest wall interface, which represents a to-and-fro movement synchronized with respiration, can be identified. US visualization of lung sliding is correlated with the absence of pneumothorax, and from this sign alone, at least anterior pneumothorax can be excluded rapidly at the bedside of a mechanically ventilated patient. However, absence of lung sliding may be caused by the presence of large bullae or pleural symphysis caused by previous pleurodesis or pleural adhesions due to previous pleural disease. Hence, the absence of lung sliding is not specific for pneumothorax, but detection of lung sliding reliably excludes the presence of pleural air in the examined area.
The most common radiographic signs of tension pneumothorax are contralateral mediastinal shift, ipsilateral diaphragmatic depression, and ipsilateral chest wall expansion. Underlying lung disease may prevent total lung collapse even if tension is present; in patients on mechanical ventilation, little or no midline mediastinal shift may result from the tension.7 In the latter, a depressed ipsilateral diaphragm is a more reliable sign of tension than mediastinal shift.
In patients with acute respiratory distress syndrome (ARDS), barotrauma can result in a localized tension pneumothorax with a subtle contralateral mediastinal shift, flattening of the cardiac contour, and depression of the ipsilateral hemidiaphragm.8 Pleural adhesions and relative compressibility and mobility of surrounding structures, in addition to the supine position, probably account for these loculated tension pneumothoraces.
In a study of 88 critically ill patients with 112 pneumothoraces, the anteromedial and subpulmonic recesses were involved in 64% of patients in the supine and semierect position.9 Furthermore, in 30% of the pneumothoraces in this study that were not initially detected by the clinician or radiologist, half the patients progressed to tension pneumothorax. Therefore, a high index of suspicion is necessary to avoid catastrophic situations.
Factors that may contribute to an improved ability to diagnose this potentially lethal problem include familiarity with atypical locations of pneumothoraces in critically ill patients, usually due to the supine or semierect position; the consequence of underlying cardiopulmonary disease; and knowledge of other risk factors contributing to misdiagnosis (e.g., mechanical ventilation, altered mental status, prolonged ICU stay, and development of pneumothorax after peak physician staffing hours).10
 Evaluation of Pleural Effusion in the Intensive Care Unit
Evaluation of Pleural Effusion in the Intensive Care Unit
Diagnostic Thoracentesis
Indications
Although disease of any organ system can cause a pleural effusion in critically ill patients, the diagnoses listed in Table 65-1 represent the majority of the causes seen in ICUs. The types of pleural effusions seen in medical and surgical ICUs are similar, but some causes related to surgical (coronary artery bypass grafting, chylothorax, abdominal surgery) and nonsurgical trauma (hemothorax) represent a substantial percentage of surgical ICU effusions.
TABLE 65-1 Causes of Pleural Effusions
| In the Medical ICU | In the Surgical ICU |
|---|---|
| Atelectasis | Atelectasis |
| Congestive heart failure | Congestive heart failure |
| Pneumonia | Pneumonia |
| Hypoalbuminemia | Pancreatitis |
| Pancreatitis | Hypoalbuminemia |
| ARDS | Coronary artery bypass surgery |
| Pulmonary embolism | ARDS |
| Hepatic hydrothorax | Pulmonary embolism |
| Esophageal sclerotherapy | Esophageal rupture |
| Postmyocardial infarction | Hemothorax |
| Iatrogenic | Chylothorax |
| Abdominal surgery | |
| Iatrogenic |
ARDS, Acute respiratory distress syndrome; ICU, intensive care unit.
When a pleural effusion is suspected on physical examination and confirmed radiologically, a diagnostic thoracentesis under ultrasonographic guidance should be performed in an attempt to establish the cause. Exceptions are patients with a secure clinical diagnosis and a small amount of pleural fluid, as in atelectasis, or patients with uncomplicated congestive heart failure (CHF).13 Observation may be warranted in these situations, but thoracentesis should be performed if there are adverse changes.11
The indications for diagnostic thoracentesis do not change simply because the patient is in the ICU or on mechanical ventilation. In fact, establishing the diagnosis quickly in these critically ill patients may be more important and life saving than in non–critically ill patients. It has been well documented that even in patients on mechanical ventilation, diagnostic thoracentesis is safe if there is strict adherence to the general principles of the procedure and ultrasonography is used.4,12 Pneumothorax, the most clinically important complication of thoracentesis,13 is no more likely to occur in the patient on mechanical ventilation than in the patient who is not; however, if a pneumothorax does develop, the patient on mechanical ventilation is likely to develop a tension pneumothorax.
Complications
Complications of diagnostic thoracentesis include pain at the needle insertion site, bleeding (local, intrapleural, or intraabdominal), pneumothorax, empyema, and spleen or liver puncture. Pneumothorax has been reported in prospective studies to occur in 4% to 30% of patients.13,14–16 However, when ultrasound-guided thoracentesis is performed by experienced physician sonographers, pneumothorax or other injuries due to organ puncture appear to be rare events.4 Liver or spleen puncture tends to occur when the patient is not sitting absolutely upright because movement toward recumbency causes cephalad migration of the abdominal viscera. The upward displacement of abdominal organs is readily detected by ultrasonography. However, even if the liver or spleen is punctured with a small-bore needle, generally the outcome is favorable if the patient is not receiving anticoagulants and does not have a bleeding diathesis.
Therapeutic Thoracentesis
Indications and Contraindications
The primary indication for therapeutic thoracentesis is relief of dyspnea. Contraindications to therapeutic thoracentesis are similar to those for diagnostic thoracentesis. However, there appears to be an increased risk of pneumothorax,13 making a therapeutic thoracentesis in patients on mechanical ventilation potentially hazardous.
The technique for therapeutic thoracentesis is essentially the same as for diagnostic thoracentesis, except that a blunt-tip needle or plastic catheter, rather than a sharp-tip needle, should be used. This reduces the risk of pneumothorax, which may occur as fluid is removed and the lung expands toward the chest wall. Again, the use of sonographic guidance is recommended.17
The amount of fluid that can be removed safely from the pleural space at one session is controversial. Ideally, monitoring pleural pressure should dictate the amount of fluid that can be removed. As long as intrapleural pressure does not fall to less than −20 cm H2O, fluid removal can continue.18 However, intrapleural pressure monitoring is not done routinely. In the patient with contralateral mediastinal shift on chest radiograph who tolerates thoracentesis without chest tightness, cough, or light-headedness, probably several liters of pleural fluid can be removed safely, but neither the patient nor the operator may be aware of a precipitous drop in pleural pressure. In patients without a contralateral mediastinal shift or with ipsilateral shift (suggesting an endobronchial obstruction), the likelihood of a precipitous drop in intrapleural pressure is increased, and pleural pressure should be monitored during thoracentesis. Alternatively, a small-bore catheter connected to a standard thoracostomy pleural drainage system may be temporarily inserted, thus avoiding excessively negative pleural pressure development during drainage. Simple gravity drainage or drainage using any system incorporating a non-return valve do not reliably guard against the development of excessively negative pressure.
Physiologic Effects and Complications
Improvement in lung volumes up to 24 hours after therapeutic thoracentesis does not correlate with the amount of fluid removed, despite relief of dyspnea in those patients.19–21 In some patients, however, maximum spirometric improvement may not occur for several days. Patients with initial negative pleural pressures and those with more precipitous falls in pleural pressure with thoracentesis tend to have the least improvement in pulmonary function after therapeutic thoracentesis because many have a trapped lung or endobronchial obstruction.18 The mechanism of dyspnea from a large pleural effusion probably is related to the increase in chest wall resting volume, resulting in shortening of the respiratory muscles’ resting length and consequent decrease in contractile efficiency.20 Drainage of moderately sized pleural effusions (1495 mL) does not appear to result in predictable changes in respiratory system compliance or resistances, although a systematic decrease in work performed by the ventilator as a consequence of thoracentesis has been reported.22
Complications of therapeutic thoracentesis are the same as those seen with diagnostic thoracentesis. Three complications unique to therapeutic thoracentesis are hypoxemia, unilateral pulmonary edema, and hypovolemia. After therapeutic thoracentesis, hypoxemia may occur despite relief of dyspnea23,24 from worsening ventilation/perfusion relationships in the ipsilateral lung or clinically occult unilateral pulmonary edema.
Some investigators have concluded that the change in partial pressure of arterial oxygen (PaO2) after therapeutic thoracentesis is unpredictable24; some have observed a characteristic increase in PaO2 within minutes to hours,19 and others suggest a systematic decrease in PaO2 that returns to prethoracentesis values by 24 hours.23 In the largest study including 33 patients with various causes of unilateral pleural effusions, a significant increase in PaO2 was found at 20 minutes, 2 hours, and 24 hours after therapeutic thoracentesis.25 This was in conjunction with a decrease in the alveolar-arterial oxygen gradient [P(A-a)O2] and was accompanied by a small but significant decrease in shunt, without a change in the ratio of dead space to tidal volume (VD/VT). Data suggest an improved ventilation/perfusion relationship after therapeutic thoracentesis, with an increase in ventilation of parts of the lung that were previously poorly ventilated but well perfused. The relief of dyspnea in these patients cannot be explained by improved arterial oxygen tension.
Improvement in lung volumes is a constant finding after therapeutic thoracentesis but may take days or even weeks to maximize; immediate changes are usually modest and highly variable. Therefore, the relief of dyspnea cannot be adequately explained by changes in lung volume or in the mechanics of breathing but may be the result of decreased stimulation of lung or chest wall receptors, or both.20
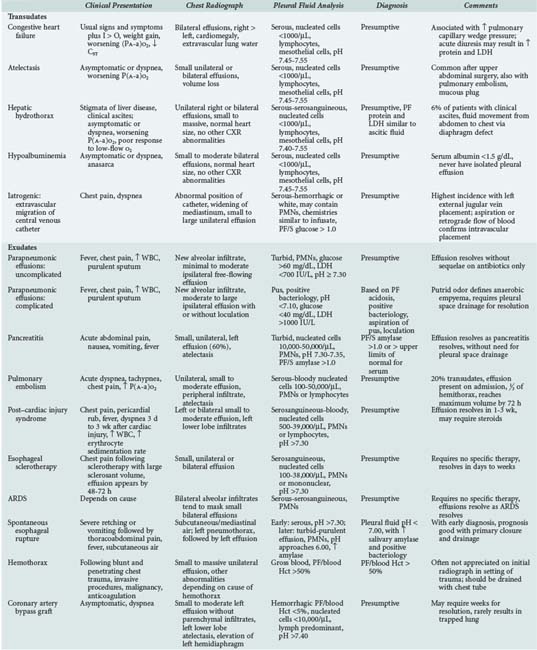
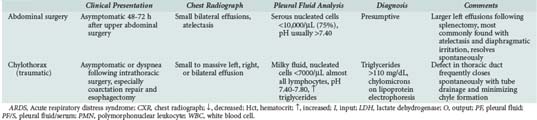
The differential diagnosis of pleural effusions in critically ill patients is outlined in Table 65-2. Brief discussions of the more common etiologies follow.
Atelectasis
Atelectasis is a common cause of small pleural effusions in comatose, immobile, pain-ridden patients in ICUs26 and after upper abdominal surgery.27,28 Other causes include major bronchial obstruction from lung cancer or a mucous plug. Atelectasis causes pleural fluid because of decreased pleural pressure. With alveolar collapse, the lung and chest wall separate further, creating local areas of increased negative pressure. This decrease in pleural pressure favors the movement of fluid into the pleural space, presumably from the parietal pleural surface. The fluid accumulates until the pleural or parietal-pleural interstitial pressure gradient reaches a steady state.
Congestive Heart Failure
CHF is the most common cause of transudative pleural effusions and a common cause of pleural effusions in ICUs. Pleural effusions due to CHF are associated with increases in pulmonary venous pressure.29 Most patients with subacute or chronic elevation in pulmonary venous pressure (pulmonary capillary wedge pressure of at least 24 mm Hg) have evidence of pleural effusion on US or lateral decubitus radiograph. Isolated increases in systemic venous pressure tend not to produce pleural effusions. Thus, patients with chronic obstructive pulmonary disease (COPD) and cor pulmonale rarely have pleural effusions, and the presence of pleural fluid implies another cause.
Most patients with pleural effusions secondary to CHF have the classic signs and symptoms. The chest radiograph shows cardiomegaly and bilateral small to moderate pleural effusions of similar size (right slightly greater than left). There is usually radiographic evidence of pulmonary congestion, with the severity of pulmonary edema correlating with the presence of pleural effusion.29
The effusion associated with CHF is a transudate, with mesothelial cells and lymphocytes accounting for the majority of the less than 1,000 cells per µL.12 Acute diuresis can raise the pleural fluid protein and lactate dehydrogenase into the range of an exudate.30,31 In the patient with secure clinical diagnosis of CHF, observation is appropriate. Thoracentesis should be performed if the patient is febrile, has pleural effusions of disparate size, has a unilateral pleural effusion, does not have cardiomegaly, has pleuritic chest pain, or has a PaO2 inappropriate for the degree of pulmonary edema.
Hepatic Hydrothorax
Pleural effusions occur in approximately 6% of patients with cirrhosis of the liver and clinical ascites. The effusions result from movement of ascitic fluid through congenital or acquired diaphragmatic defects.32–34
The patient usually has the classic stigmata of cirrhosis and clinically apparent ascites. The usual chest radiograph shows a normal cardiac silhouette and a right-sided pleural effusion, which can vary from small to massive; effusions are less likely isolated to the left pleural space or are bilateral.32–35 Rarely, a massive pleural effusion may be found without clinical ascites (demonstrated only by US), implying the presence of a large diaphragmatic defect. The pleural fluid is a serous transudate with a low nucleated cell count and a predominance of mononuclear cells, pH greater than 7.40, and a glucose level similar to that of serum.12 The fluid can be hemorrhagic due to an underlying coagulopathy or rupture of a diaphragmatic bleb. Demonstrating that pleural and ascitic fluids have similar protein and lactate dehydrogenase concentrations substantiates the diagnosis.32 If the diagnosis is problematic, injection of a radionuclide into the ascitic fluid, with detection on chest imaging within 1 to 2 hours, supports a pleuroperitoneal communication through a diaphragmatic defect36; delayed demonstration of the tracer suggests that the pathogenesis of the effusion is via convection through the mesothelium.
Hepatic hydrothorax may be complicated by spontaneous bacterial empyema (SBE), which is analogous to spontaneous bacterial peritonitis. The criteria for diagnosis of SBE are similar to those for the diagnosis of spontaneous bacterial peritonitis. SBE must be considered in the differential diagnosis of the infected cirrhotic patient, even in the absence of clinical ascites.37,38 The pleural fluid culture and analysis may reveal positive culture, a total neutrophil count of more than 500 cells per µL, and a serum to pleural fluid albumin gradient greater than 1.1. The chest radiograph should not show a pneumonic process. Treatment of SBE is conservative with antibiotics unless purulence is present, in which case tube thoracostomy must be considered.
Treatment of hepatic hydrothorax is directed at resolution of the ascites, using sodium restriction and diuresis. The effusion frequently persists unchanged until all ascites is mobilized. If the patient is acutely dyspneic or in respiratory failure, therapeutic thoracentesis should be done as a temporizing measure. Care should be exercised with paracentesis or thoracentesis, because hypovolemia can occur with rapid evacuation of fluid. Chest tube insertion should be avoided, as it can cause infection of the fluid, and prolonged drainage can lead to protein and lymphocyte depletion and renal failure. Chemical pleurodesis via a chest tube is often unsuccessful owing to rapid movement of ascitic fluid into the pleural space. Treatment options in hepatic hydrothorax refractory to medical management include transjugular intrahepatic portal systemic shunt and video-assisted thoracoscopy to patch the diaphragmatic defect, followed by pleural abrasion or talc poudrage in the properly selected patient.39,40
Hypoalbuminemia
Many patients admitted to a medical ICU have a chronic illness and associated hypoalbuminemia. When the serum albumin level falls below 1.8 g/dL, pleural effusions may be observed.41 Because the normal pleural space has an effective lymphatic drainage system, pleural fluid tends to be the last collection of extravascular fluid that occurs in patients with low oncotic pressure. Therefore, it is unusual to find a pleural effusion solely due to hypoalbuminemia in the absence of anasarca. Patients with hypoalbuminemic pleural effusions tend not to have pulmonary symptoms unless there is underlying lung disease, since the effusions are rarely large. Chest radiograph shows small to moderate bilateral effusions and a normal heart size. The pleural fluid is a serous transudate with less than 1000 nucleated cells per µL, predominantly lymphocytes and mesothelial cells. The pleural fluid glucose level is similar to that of serum, and the pH is in the range of 7.45 to 7.55. Diagnosis is presumptive if other causes of transudative effusions can be excluded. The effusions resolve when hypoalbuminemia is corrected.
Iatrogenic Causes
Extravascular migration of a central venous catheter can cause pneumothorax, hemothorax, chylothorax, or a transudative pleural effusion.42–44 Its incidence is estimated at less than 1% but may be considerably higher. Malposition of the catheter on placement should be suspected if there is absence of blood return or questionable central venous pressure measurements. The immediate postprocedure chest radiograph should be assessed for proper catheter placement; a catheter placed from the right side should not cross the midline. If the catheter is not in the appropriate vessel, phlebitis, perforation of a vein or the heart, or instillation of fluid into the mediastinum or pleural space can occur. In the alert patient, acute infusion of intravenous fluid into the mediastinum usually results in new-onset chest discomfort and dyspnea. Depending on the volume and the rate at which it is introduced into the mediastinum, tachypnea, worsening respiratory status, and cardiac tamponade may ensue. The chest radiograph shows the catheter tip in an abnormal position,45,46 a widened mediastinum, and evidence of unilateral or bilateral pleural effusions. The effusion can have characteristics similar to those of the infusate (milky if lipid is being given) and may be hemorrhagic and neutrophil-predominant due to trauma and inflammation. The pleural fluid to serum glucose ratio is greater than 1.0 if glucose is being infused.43 The pleural fluid glucose concentration can fall rapidly after glucose infusion into the pleural space, probably explaining the relatively low glucose concentrations in pleural fluid compared to the infusate.47 Extravascular migration of a central venous catheter appears to be more common with placement in the external jugular vein, particularly on the left side. Left-sided catheters appear to put the patient at increased risk of perforation because of the horizontal orientation of the left compared to the right brachiocephalic vein. When catheters are introduced from the left side, they should be of adequate length for the tip to rest in the superior vena cava.
Parapneumonic Effusions
Community-acquired or nosocomial pneumonia is common in critically ill patients. The classic presentation is fever, chest pain, leukocytosis, purulent sputum, and a new alveolar infiltrate on chest radiograph. In the elderly debilitated patient, however, many of these findings may not be present. The chest radiograph commonly shows a small to large ipsilateral pleural effusion.4,8,48–50 When the effusion is free flowing and anechoic on ultrasound, and thoracentesis shows a nonpurulent, polymorphonuclear (PMN) predominant exudate with a pH of 7.30 or greater, it is highly likely that the effusion will resolve during 7 to 14 days without sequelae with antibiotics alone (uncomplicated effusion). If the chest radiograph or CT demonstrates loculation and pus is aspirated, the diagnosis of empyema is established and immediate drainage is needed. In the free-flowing nonpurulent fluid, if Gram stain or culture is positive or pH is less than 7.30, the likelihood of a poor outcome increases, and the pleural space should be drained.
Although a meta-analysis found that low-risk patients with fluid pH between 7.20 and 7.30 may be managed without tube drainage, the patient admitted to the ICU typically cannot be considered low risk, and pH values of less than 7.30 should prompt drainage in most cases.51–53 Drainage can be accomplished by standard chest tube or small-bore catheter. When loculations occur, pleural space drainage should be accomplished by placement of image-guided tubes or catheters with fibrinolytics or empyectomy and decortication.54,55 Most thoracic surgeons routinely begin with thoracoscopy and, if not successful, proceed directly to a standard thoracotomy for empyectomy and decortication.56–59
Pancreatitis
Pleuropulmonary abnormalities are commonly associated with pancreatitis, largely owing to the close proximity of the pancreas to the diaphragm. Approximately half of patients with pancreatitis have an abnormal chest radiograph, with pleural effusions in 3% to 17%.60,61 Mechanisms that may be involved in the pathogenesis of pancreatic pleural effusion include direct contact of pancreatic enzymes with the diaphragm (sympathetic effusion), transfer of ascitic fluid via diaphragmatic defects, communication of a fistulous tract between a pseudocyst and the pleural space, and retroperitoneal movement of fluid into the mediastinum with mediastinitis or rupture into the pleural space.60,62 Ascitic amylase moves into the pleural space via the previously mentioned mechanisms. The pleural fluid/serum amylase ratio is greater than one in pancreatitis because of slower lymphatic clearance from the pleural space compared with more rapid renal clearance.
The effusion associated with acute pancreatitis is usually small and left-sided (60%) but may be isolated to the right side (30%) or be bilateral (10%).60 The patient usually presents with abdominal symptoms of acute pancreatitis. Diagnosis is confirmed by an elevated pleural fluid amylase concentration greater than that in serum. A normal pleural fluid amylase may be found early in acute pancreatitis but increases on serial measurements. The fluid is a polymorphonuclear (PMN)-predominant exudate with glucose values approximating those of serum. Leukocyte counts may reach 50,000 cells per µL. The pleural fluid pH is usually 7.30 to 7.35.
Pulmonary Embolism
The presence of a unilateral pleural effusion may suggest pulmonary embolism or obscure the diagnosis by directing attention to a primary lung or cardiac process. Pleural effusions occur in approximately 40% of patients with pulmonary embolism.63 These effusions result from several different mechanisms including increased pleural capillary permeability, imbalance in microvascular and pleural space hydrostatic pressures, and pleuropulmonary hemorrhage.63,64 Ischemia from pulmonary vascular obstruction, in addition to release of inflammatory mediators from platelet-rich thrombi, can cause capillary leak into the lung and, subsequently, the pleural space, explaining the usual finding of an exudative effusion. Transudates, described in approximately 20% of patients with pulmonary embolism, result from atelectasis.64
With pulmonary infarction, necrosis and hemorrhage into the lung and pleural space may result. More than 80% of patients with infarction have bloody pleural effusions, but more than 35% of patients with pulmonary embolism without radiographic infarction also have hemorrhagic fluid.63 The presence of a pleural effusion does not alter the signs or symptoms in patients with pulmonary embolism. Chest pain, usually pleuritic, occurs in most patients with pleural effusions complicating pulmonary embolism and is invariably ipsilateral.63 The chest radiograph virtually always shows a unilateral effusion that occupies less than one-third of the hemithorax.63 An associated pulmonary infiltrate (infarction) is seen in approximately half of patients with pulmonary embolism and effusion.
Pleural fluid analysis is variable and nondiagnostic.64 The pleural fluid is hemorrhagic in two-thirds of patients, but the number of red blood cells exceeds 100,000 per µL in less than 20%.64 The nucleated cell count ranges from less than 100 (atelectatic transudates) to greater than 50,000 per µL (pulmonary infarction).64 There is a predominance of PMNs when a thoracentesis is performed near the time of the acute injury and of lymphocytes with later thoracentesis. The effusion due to pulmonary embolism is usually (92%) apparent on the initial chest radiograph and reaches a maximum volume during the first 72 hours.63 Patients with pleural effusions that progress with therapy should be evaluated for recurrent embolism, hemothorax secondary to anticoagulation, an infected infarction, or an alternate diagnosis. When consolidation is absent on chest radiograph, effusions usually resolve in 7 to 10 days; with consolidation, the resolution time is 2 to 3 weeks.64
The association of pleural effusion with pulmonary embolism does not alter therapy. Furthermore, the presence of a bloody effusion is not a contraindication to full-dose anticoagulation because hemothorax is a rare complication of heparin therapy.65 An enlarging pleural effusion on therapy necessitates thoracentesis to exclude hemothorax, empyema, or another cause. Active pleural space hemorrhage necessitates discontinuation of anticoagulation, tube thoracostomy, and placement of a vena cava filter.
Post–Cardiac Injury Syndrome
Post–cardiac injury syndrome (PCIS) is characterized by fever, pleuropericarditis, and parenchymal infiltrates 3 weeks (2 to 86 days) after injury to the myocardium or pericardium.66–68 PCIS has been described after myocardial infarction, cardiac surgery, blunt chest trauma, percutaneous left ventricular puncture, and pacemaker implantation. The incidence after myocardial infarction has been estimated at up to 4% of cases,66 but with more extensive myocardial and pericardial involvement, it may be higher. It occurs with greater frequency (up to 30%) after cardiac surgery.69 The pathogenesis of PCIS remains obscure; an autoimmune response in patients with myocardial or pericardial injury and possibly concomitant viral illness has been speculated.70
Pleuropulmonary manifestations are the hallmark of PCIS. The most common presenting symptoms are pleuritic chest pain, found in virtually all patients, and fever, pericardial rub, dyspnea, and rales, which occur in half of patients.68 Rarely, hemoptysis occurs, an important differential point when pulmonary embolism with infarction is in the differential diagnosis. Fifty percent of patients have leukocytosis, and almost all have an elevated erythrocyte sedimentation rate (average, 62 mm per hour).68
The chest radiograph is abnormal in virtually all patients, with the most common abnormality being left-sided and bilateral pleural effusions; a unilateral right effusion is unusual.68 Pulmonary infiltrates are present in 75% of patients and are most commonly seen in the left lower lobe.66 The pleural fluid is a serosanguineous or bloody exudate with a glucose level above 60 mg per dL and pleural fluid pH above 7.30. Nucleated cell counts range from 500 to 39,000 per µL, with a predominance of PMNs early in the course.68 Pericardial fluid on echocardiogram is an important finding suggesting PCIS. The pleural fluid characteristics should help differentiate PCIS from a parapneumonic effusion and CHF, but do not exclude pulmonary embolism.


Full access? Get Clinical Tree


