Platelets and Immunology of Migraines
Rajiv Joseph
Jacqueline deBelleroche
Giovanni D’Andrea
Andre Pradalier
Platelets are anuclear cellular components of blood that function primarily to secure hemostasis. They are metabolically adapted to expend large amounts of energy rapidly during aggregation, secretion, and clot formation. Platelets have been likened to a sponge because of their remarkable propensity to absorb various substances from plasma, including serotonin and amino acids (62). The sequence of platelet response to stimulation is called the basic platelet reaction (57). Vascular injury results first in the adhesion of platelets to the vessel wall. The platelets then change shape from their normal discoid appearance into spheres with pseudopodia and adhere to one another in the process of primary aggregation. Simultaneously, a constricting wave of microtubular contraction results in dense bodies and α granules being shifted to the center of the platelet, and the granular contents are secreted into the tubular system for release to the exterior. The dense bodies contain substances such as adenine nucleotides and serotonin, whereas the α granules contain fibrinogen, β-thromboglobulin (βTG), and platelet factor-4. Platelet secretory products, together with thromboxane A2 synthesized within platelets from arachidonic acid, cause irreversible secondary aggregation, leading to thrombus formation and hemostasis.
PLATELET STUDIES IN MIGRAINE
Tests of platelet activity have a degree of intrinsic variability, and more than three decades ago it was recommended that limits of variability be ascertained before comparing results in groups of patients (53). Platelet studies in migraine sufferers have not established the normal range of variability for the tests. Frequently, conclusions on the role of platelets in migraine have been drawn on the basis of trends seen in a solitary test of platelet activity. This is hazardous for the following reasons. First, normal platelet function combines several activities including adhesion, aggregation, and secretion, which are not all reflected by any one test. Second, the platelet is susceptible to a wide range of physiologic changes, such as age, gender, and stress. The possibility that one of these variables might account for the platelet changes would be higher if only a single test were performed. Finally, because the tests per se have a great deal of intrinsic variability, it is more reliable if consistent changes are seen in a complete range of platelet investigations. Such caveats must be applied when considering the studies described. Platelet aggregation and secretion has conventionally been studied using the optical principle in platelet-rich plasma, prepared to be free of other blood cells (13). Although this method does not fully reflect the in vivo state, increased spontaneous (52), serotonin- (61), adenosine diphosphate- (19), and epinephrine-induced (71) platelet aggregation have been observed in migraine sufferers between attacks. As a result, inhibition of platelet aggregation was postulated to be of therapeutic value in migraine (34). Indeed, drugs such as methysergide (47,75,106) and ergotamine (46), beneficial in treating migraine, also inhibit platelet aggregation (6,20). However, the inhibitory effect of ergotamine on platelet aggregation was found to be unrelated to clinical efficacy (55). The prophylactic efficacy of β-blockers (113) and naproxen sodium (118), a potent inhibitor of platelet aggregation, was also unrelated to inhibition of platelet aggregation. Furthermore, serial study of platelet aggregation during acute migraine has revealed no correlation with migraine-associated neurologic symptoms (19). Subsequent studies in whole blood using the impedance technique, a better reflection of the in vivo state, confirmed normal aggregability in migraine sufferers (66). Nevertheless, platelet levels of the aggregating prostaglandin D2 were reduced without change in thromboxane in female migraineurs, as well as reduced prostacyclin and an inducer of endothelial prostacyclin (91). It remains to be determined whether platelet eicosanoids are involved in migraine pathogenesis, although speculatively they have the potential to induce cellular, vascular, or neurologic effects during an attack. Platelet benzodiazepine receptors also are increased between attacks of migraine, invoking a link
with mitochondrial dysfunction because these receptors modulate mitochondrial respiratory chain function (85).
with mitochondrial dysfunction because these receptors modulate mitochondrial respiratory chain function (85).
PLATELET ACTIVITY IN ACUTE MIGRAINE
Platelet activity is altered in acute migraine. After the establishment of an index of variability for each test of platelet activity in migraine sufferers, estimations of changes in aggregation, secretion, plasma thromboxane, and circulating platelet microaggregates during acute migraine attacks were made (62). These measurements of platelet activity were tested in a prospective manner in eight migraineurs carefully selected for their cooperativity. All subjects had readily identifiable migraine attacks occurring two to four times per month. They were administered (single-blind) placebo capsules matched for Inderal (Wyeth-Ayerst) LA 160 mg (propranolol) once per day for up to 8 consecutive weeks. Four patients had no migraine attacks, and each of the other four subjects were studied serially during one of their migraine attacks that occurred during the study period. The duration of individual attacks varied from 24 to 36 hours. Platelet activity tests were performed weekly in these subjects, and three times during an acute migraine attack at the beginning, peak, and end. All platelet measurements were increased in acute migraine, and, except for plasma thromboxane, which was raised above the normal range, the other tests were within the normal range of variability seen in these subjects. A platelet activity index derived by integrating all the tests was maximal shortly after cessation of the attack and not at the start, as would be predicted if platelets had a causal role in migraine pathogenesis (Fig. 36-1).
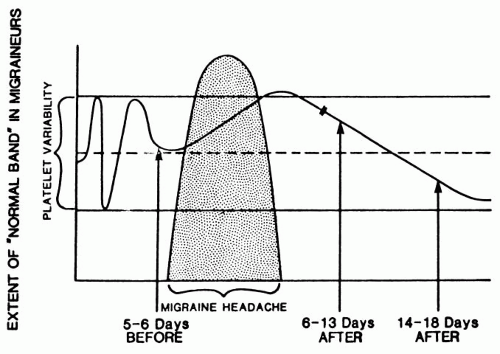 FIGURE 36-1. Model of platelet activity in migraine. Peak platelet activity soon after cessation of headache; normality restored within 2 weeks; migraine causes increased platelet activity. |
Nitroglycerin-induced migraine attacks were associated with calcitonin gene-related peptide (CGRP) release into plasma in concert with decreased platelet serotonin. Results suggested that the CGRP release is directly related to the headache whereas the serotonin changes may act to prevent or lower CGRP release (70).
SIGNIFICANCE OF PLATELET ACTIVATION IN MIGRAINE
Although not of causal importance, the reason for platelet activation in migraine is not known. One possibility is that platelet activation is a consequence of stress (64). There is a well-recognized relationship between stress and migraine (93). Stress precipitates migraine, and migraine worsens stress. The manifestations of migraine are easily related to those of excessive circulating catecholamines. Catecholamines and free fatty acids, known platelet-stimulating agents, increase during migraine (58) and after stress (11,17,81). Platelet activity is increased nonspecifically in several apparently unrelated conditions, such as cerebrovascular disease (63,68), multiple sclerosis (88), anorexia nervosa (80), psoriasis (9), alcohol withdrawal (59), and with smoking (79). Physiologic stress is also associated with increased platelet activity (53). Oxidative stress has been linked to increased platelet membrane rigidity, and reduced cytosolic calcium in the resting state and after thrombin stimulation. This suggests an increased vulnerability of platelets to oxidative stress in migraine sufferers (115). Whatever may be the cause for platelet activation in migraine, it is not without clinical significance. Increased platelet activity may contribute to a prothrombotic state, leading to stroke, a well-recognized complication of migraine (14,19,71). Further, proinflammatory platelet adhesion to leukocytes occurs during headache-free intervals, similar to that seen in cerebrovascular disease (120). Consequently, it appears safer to avoid the use of drugs that increase platelet activity in migraineurs (64).
PLATELET SEROTONERGIC FUNCTION
The wealth of information contained in studies of platelets in migraine sufferers provides support for a biochemical abnormality in migraine (65). Although the platelet is not directly involved in migraine causation, it is a biochemical storehouse and contains a number of substances such as serotonin and catecholamines, and is easily available for study. Therefore, platelets have been used as a model to study the function of certain of these substances in migraine (82). Serotonergic nerve endings and platelets share many morphologic, biochemical, and physiologic
characteristics. These similarities are believed to derive from their common ectodermal origin (16). Both tissues accumulate, store, and release serotonin. They possess α2-, β2-, 5-hydroxytryptamine 2 (5-HT2)-, and specific imipramine-binding sites and use Ca2+ and metabolites of the phosphoinositol and prostaglandin pathways as mediators of secretion (38,76,94,95,97). Therefore, the metabolism of serotonin in the platelet dense body may mirror that in the nervous system (82). This has justified studying the platelet, particularly its dense body, as a model of central serotonergic metabolism and function. Almost all of the serotonin present in blood is located in dense bodies and is released on platelet activation (51). The amount of free serotonin in plasma is extremely low and its estimation difficult (25). A transient increase in plasma serotonin may cause a sterile inflammatory response in vascular walls and increase their permeability (24). Serotonin is mainly converted to 5-hydroxyindole acetic acid (5-HIAA) for renal excretion (23,27). Increase of 5-HIAA in urine and cerebrospinal fluid has been reported in migraine sufferers (68,72). Controversy surrounds the relationship of these observations to platelet serotonin content. Some investigators have noticed an inverse correlation between increased urinary 5-HIAA and decreased platelet serotonin (2,21,99), but others have not (21,92,104). Hannington et al. showed that the release of platelet serotonin within 3 days of a migraine attack was reduced compared with migraine-free intervals (52). However, it has not been established whether changes in platelet serotonin are caused by a primary platelet abnormality or are secondary to a plasma factor (3,40,109,121).
characteristics. These similarities are believed to derive from their common ectodermal origin (16). Both tissues accumulate, store, and release serotonin. They possess α2-, β2-, 5-hydroxytryptamine 2 (5-HT2)-, and specific imipramine-binding sites and use Ca2+ and metabolites of the phosphoinositol and prostaglandin pathways as mediators of secretion (38,76,94,95,97). Therefore, the metabolism of serotonin in the platelet dense body may mirror that in the nervous system (82). This has justified studying the platelet, particularly its dense body, as a model of central serotonergic metabolism and function. Almost all of the serotonin present in blood is located in dense bodies and is released on platelet activation (51). The amount of free serotonin in plasma is extremely low and its estimation difficult (25). A transient increase in plasma serotonin may cause a sterile inflammatory response in vascular walls and increase their permeability (24). Serotonin is mainly converted to 5-hydroxyindole acetic acid (5-HIAA) for renal excretion (23,27). Increase of 5-HIAA in urine and cerebrospinal fluid has been reported in migraine sufferers (68,72). Controversy surrounds the relationship of these observations to platelet serotonin content. Some investigators have noticed an inverse correlation between increased urinary 5-HIAA and decreased platelet serotonin (2,21,99), but others have not (21,92,104). Hannington et al. showed that the release of platelet serotonin within 3 days of a migraine attack was reduced compared with migraine-free intervals (52). However, it has not been established whether changes in platelet serotonin are caused by a primary platelet abnormality or are secondary to a plasma factor (3,40,109,121).
Related posts:







Full access? Get Clinical Tree


