CHAPTER 56
Perlèche
(Angular Cheilitis)
Presentation
The patient complains of inflammation and soreness of the skin and contiguous labial mucous membranes at the angles of the mouth (Figure 56-1). On examination, there is erythema, fissuring, and maceration of the oral commissures. In severe cases, the splits can bleed when the mouth is opened, and shallow ulcers or a crust may form.
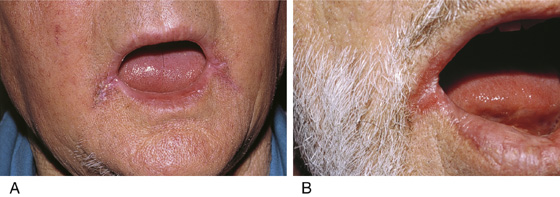
Figure 56-1 A and B, Perlèche. (From White G, Cox N: Diseases of the skin. St Louis, 2006, Mosby.)
What To Do:
 Attempt to identify a precipitating cause, and advise corrective action when possible.
Attempt to identify a precipitating cause, and advise corrective action when possible.
 Prescribe topical antifungal cream, such as ketoconazole 2% (Nizoral), econazole 1% (Spectazole), or ciclopirox olamine 0.77% (Loprox) applied bid, followed in a few hours by a corticosteroid in a nongreasy base, such as triamcinolone 0.1% (Kenalog) cream 15 g. Discontinue the steroids when the inflammation subsides in favor of a protective lip balm, such as ChapStick.
Prescribe topical antifungal cream, such as ketoconazole 2% (Nizoral), econazole 1% (Spectazole), or ciclopirox olamine 0.77% (Loprox) applied bid, followed in a few hours by a corticosteroid in a nongreasy base, such as triamcinolone 0.1% (Kenalog) cream 15 g. Discontinue the steroids when the inflammation subsides in favor of a protective lip balm, such as ChapStick.
 It is critical that the oral commissure be kept dry to decrease the chances of reinfection. Continue the antifungal cream for a few weeks for greatest effectiveness.
It is critical that the oral commissure be kept dry to decrease the chances of reinfection. Continue the antifungal cream for a few weeks for greatest effectiveness.
 Treat any associated oral candidiasis with an appropriate oral antimycotic (see Chapter 53).
Treat any associated oral candidiasis with an appropriate oral antimycotic (see Chapter 53).
What Not To Do:
 Do not use ointments or creams containing neomycin (Neosporin). They are unlikely to be effective and may cause an unnecessary contact dermatitis.
Do not use ointments or creams containing neomycin (Neosporin). They are unlikely to be effective and may cause an unnecessary contact dermatitis.
Perlèche is associated with the collection of moisture at the corners of the mouth, which encourages invasion by Candida albicans, staphylococci, streptococci, and other organisms. In children, this collection of moisture is often caused by lip-licking, drooling, thumb-sucking, and mouth-breathing. Adults may be troubled by age-related changes in oral architecture commonly seen in edentulous patients and in patients with poorly fitting dentures. The differential diagnosis includes impetigo (see Chapter 172) and herpes simplex (see Chapter 54) infections. Vitamin B2 or zinc deficiency or iron deficiency anemia can cause perlèche, but this is rare and should not be treated presumptively. The patient should be evaluated for evidence of poor diet or malnutrition (celiac disease). Angular cheilitis can also be a sign of anorexia or bulimia secondary to the associated malnutrition and frequent vomiting. KOH preparation (potassium hydroxide) will confirm a yeast infection. Cheilosis may also be part of a group of symptoms (dysphagia resulting from upper esophageal webs, iron deficiency anemia, burning mouth syndrome with a shiny red tongue resulting from glossitis, along with cheilosis) defining the condition called Plummer-Vinson syndrome.


Full access? Get Clinical Tree


