CHAPTER 20
Periorbital Nerve Blocks (Supraorbital, Supratrochlear, and Infraorbital Nerves)
INDICATIONS
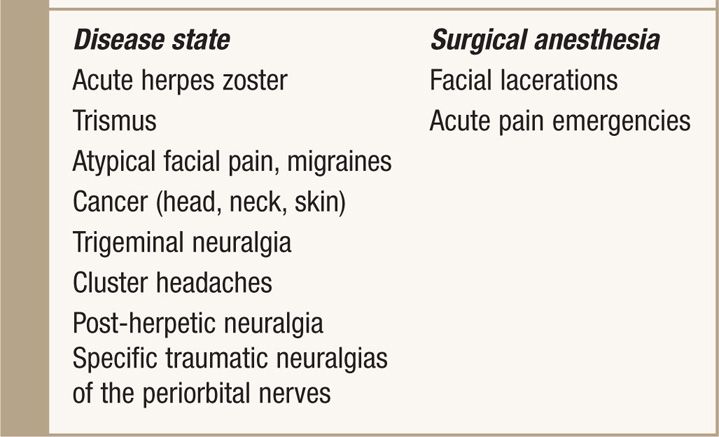
Blockade of the periorbital nerves (supraorbital, supratrochlear, and infraorbital) is useful for surgical anesthesia of the face, treatment of painful facial conditions, and can provide diagnostic information for the possibility of neurolytic blocks and neuromodulatory techniques. The indications are summarized in Table 20-1.
TABLE 20-1. Indications for Periorbital Nerve Blocks
ANATOMY
• The supraorbital and supratrochlear nerves are terminal branches of the ophthalmic division of the trigeminal nerve (V1).
• The infraorbital nerve is a terminal branch of the maxillary division of the trigeminal nerve (V2).
• V1 provides cutaneous innervation above the eye, forehead, and along the medial aspect of the nasal bridge.
• V2 provides cutaneous innervation below the eye and the areas medial to the zygomatic arch to the nostril and the lateral forehead (Figure 20-1).
• The supraorbital, supratrochlear, and infraorbital nerves lie along a vertical plane, which extends from the supraorbital notch to the corner of the mouth, bisecting the pupil.
• The supraorbital notch is located above the pupil in the orbital rim, the supratrochlear groove is just medial to the supraorbital notch, while the infraorbital foramen is located 1 cm below the orbital rim, within the vertical plane.
• The nerves emanate from these foramina respectively (Figure 20-2).
• The supraorbital and infraorbital notches are relatively easy to palpate.
• The supratrochlear nerve emanates from the supratrochlear notch, which lies at the intersection of the nasal bridge and the supraorbital ridge, medial to the supraorbital notch (Figure 20-3).
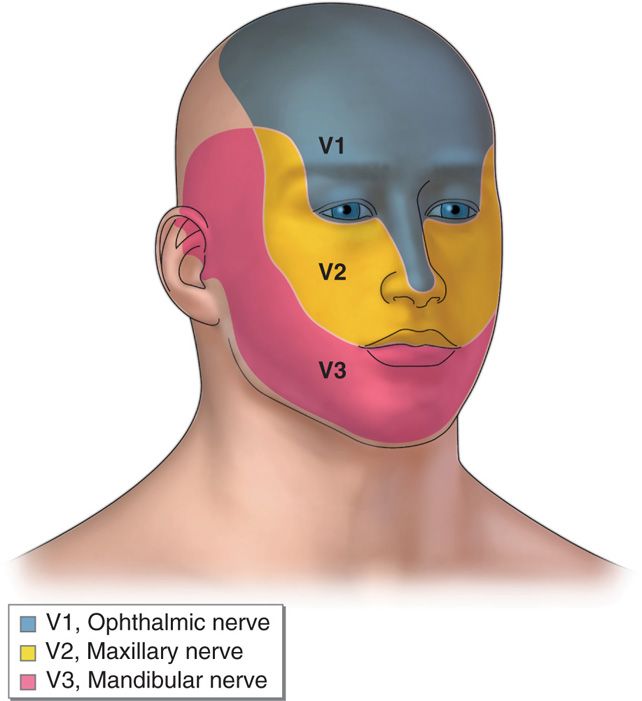
Figure 20-1. Trigeminal pattern.
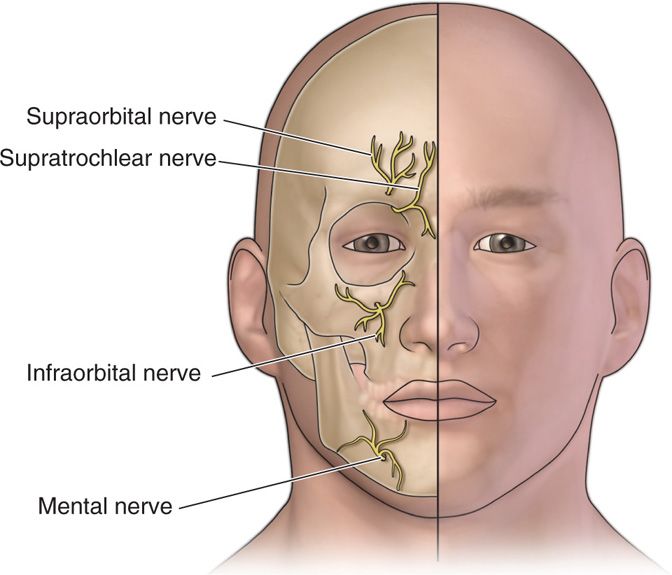
Figure 20-2. Trigeminal terminal branches.
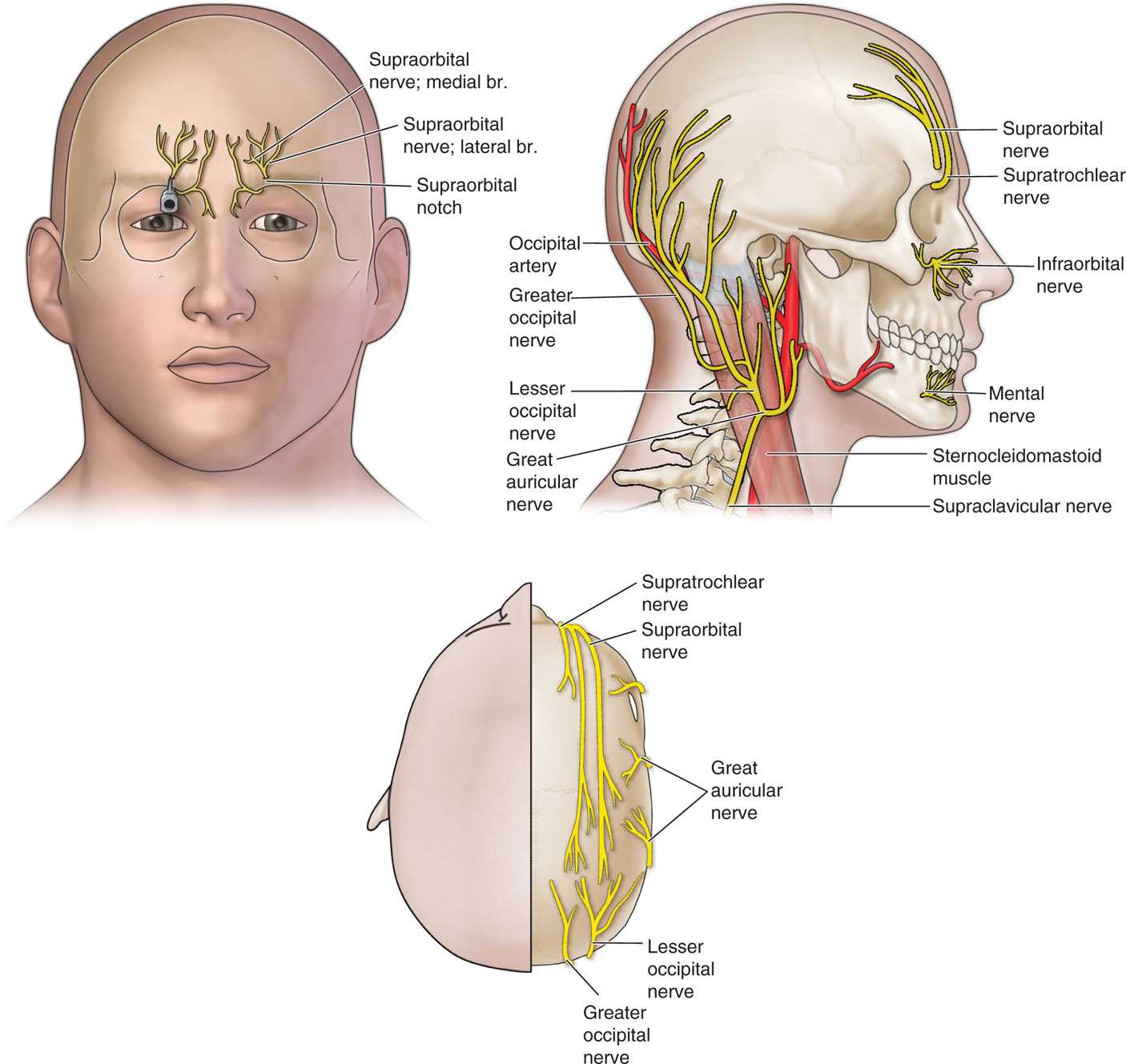
Figure 20-3. Supraorbital and infraorbital nerves.
CONTRAINDICATIONS
There are absolute and relative contraindications to performing periorbital nerve blocks, summarized below (Table 20-2):
TABLE 20-2. Absolute and Relative Contraindications to Periorbital Nerve Blocks
Preoperative Considerations
• Pt should be thoroughly evaluated prior to any interventional pain procedure and the risks/benefits explained.
• Although a relative contraindication, coagulopathy does not preclude the safe performance of a periorbital nerve block.
• Many patients who are anticoagulated suffer from painful conditions of the face and can benefit greatly from a periorbital nerve block.
• The risk/benefit ratio of stopping such medications (Plavix, Coumadin, etc) prior to the procedure may not be acceptable in certain situations (history of stroke, MI, stent, etc).
• Use small gauge needles (25, 27, or 30 gauges) and apply appropriate pressure to the injection site post block.
• A cold compress can be used to mitigate the effects of hematoma and ecchymosis, which can be seen with these procedures.
• Since this area is highly vascular, systemic uptake of local anesthetic can occur and the dose of such should be considered.
• Although usually not seen in the low doses commonly used for these blocks, local anesthetic toxicity may occur and consists of signs such as metallic taste, altered mental status, seizures, and ultimately hemodynamic compromise.
Positioning
The patient is placed in the supine or semi-recumbent position and monitored appropriately. The supraorbital notch and infraorbital foramen are palpated to identify the structure and confirm the diagnosis (Figures 20-4 to 20-5).

Figure 20-4. Supraorbital exam. (Used with permission from Andrea Trescot, MD.)

Figure 20-5. Infraorbital exam. (Used with permission from Andrea Trescot, MD.)
Typically local anesthetics such as lidocaine or bupivicaine may be utilized in small volumes, not usually exceeding 2 cc. Small syringes (3 cc) should be used.
Technique
Supraorbital nerve (Figure 20-6):
• The supraorbital notch is identified in the vertical plane described above and sterilely prepped with antiseptic solution with care to avoid any excess from entering the eye.
• The patient is asked to look directly in front (usually told to pick a spot on the ceiling) to ensure midline position of the pupil. This aligns the supraorbital notch and infraorbital foramen in the same plane.
• The skin at the notch is entered with a small gauge needle (25, 27, or 30 gauges) and directed slightly medially to avoid entering the foramen until periosteum is contacted.
• A paresthesia may be elicited and the patient should be counseled prior to the procedure regarding this.
• If the needle enters the foramen, it should be drawn back to prevent intracranial and/or intraneural injection.
• After careful aspiration, 1 to 2 cc of local anesthetic is injected. Large volumes may actually entrap the nerve.
• Soft gauze should be used after the injection to apply gentle pressure to the orbital soft tissue to prevent subcutaneous dissection of local anesthetic.

Figure 20-6. Supraorbital injection. (Used with permission from Andrea Trescot, MD.)
Supratrochlear nerve:
• The junction of the nasal bridge and the supraorbital rim is palpated and sterilely prepped with antiseptic solution, with care to avoid any excess entering the eye.
• A needle is inserted through the skin just lateral to this point and directed medially into the subcutaneous tissues.
• A paresthesia may be elicited and the patient should be counseled prior regarding this.
• After careful aspiration, 0.5 to 1 cc of local anesthetic is injected.
• Soft gauze should be used during injection to apply gentle pressure to the orbital soft tissue to prevent subcutaneous dissection of local anesthetic.
Infraorbital nerve; extraoral approach (Figure 20-7):
• The infraorbital nerve is approached 1 cm below the orbital rim in the vertical plane passing through the supraorbital notch and the pupil.
• The patient is asked to look directly in front (usually told to pick a spot on the ceiling) to ensure midline position of the pupil.
• The skin is sterilely prepped with antiseptic solution, with care to avoid any excess entering the eye.
• The needle is inserted into the skin and directed 15 degrees medially to avoid entry into the foramen until periosteum is contacted.
• A paresthesia may be elicited and the patient should be counseled prior regarding this.

Figure 20-7. Infraorbital percutaneous injection. (Used with permission from Andrea Trescot, MD.)
• After careful aspiration, 1 to 2 cc of local anesthetic is injected.
• Soft gauze should be used during injection to apply gentle pressure to the orbital soft tissue to prevent subcutaneous dissection of local anesthetic.
Infraorbital nerve; intraoral approach (Figure 20-8):

Figure 20-8. Infraorbital intraoral injection. (Used with permission from Andrea Trescot, MD.)
• This approach to the infraorbital nerve may be desired when
– Surgical anesthesia is required for removal of lesions.
– Laceration repair is needed.
– Cosmetic considerations, such as avoiding needle puncture sites externally, are needed.
– There is inability to access the nerve using the extraoral approach.
• The infraorbital foramen is palpated and the upper lip is pulled backward.
• The alveolar sulcus is then anesthetized with a cotton ball soaked with either 10% cocaine or 2% viscous lidocaine.
• A 25-gauge 1.5-in needle is inserted through the mucosa toward the infraorbital foramen.
• A paresthesia may be elicited and the patient should be counseled prior regarding this.
• After careful aspiration, 1 to 2 cc of local anesthetic is injected.
• Soft gauze should be used during injection to apply gentle pressure to the orbital soft tissue to prevent subcutaneous dissection of local anesthetic.
Complications
• Intravascular injection may occur with the possible concomitant signs and symptoms listed previously.
• More common are post-block ecchymosis or hematoma formation, secondary to vascular injury.
This can be mitigated by applying a cold compress with pressure immediately after injection.
• Infection can occur with any interventional procedure and should be aggressively diagnosed and treated.
• Infections in this area can be highly aggressive and spread into the CNS quickly.
Fluoroscopic Guidance
The supraorbital notch can be imaged under direct fluoroscopic view, which may aid in performing periorbital nerve blocks (Figures 20-9 and 20-10).
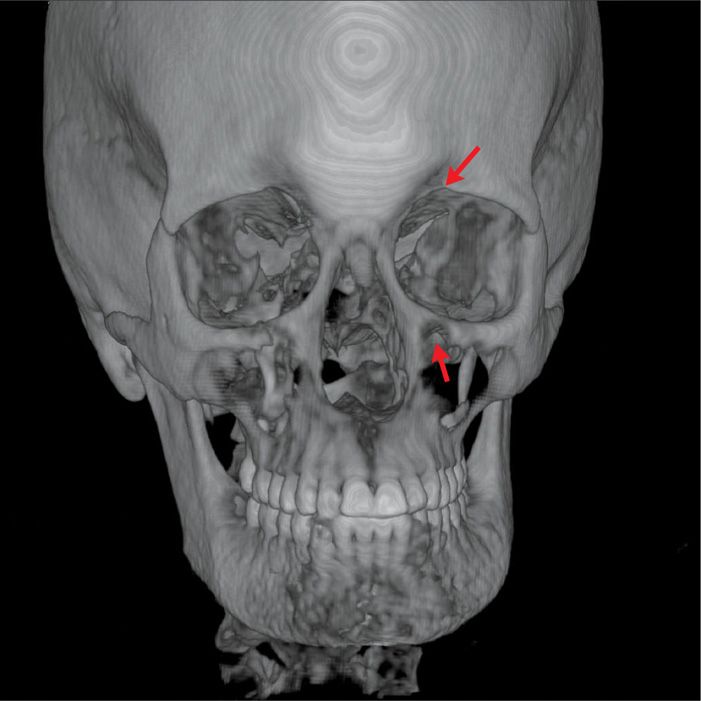
Figure 20-9. Fluoroscopic imaging of supraorbital notch. (Used with permission from Andrea Trescot, MD.)
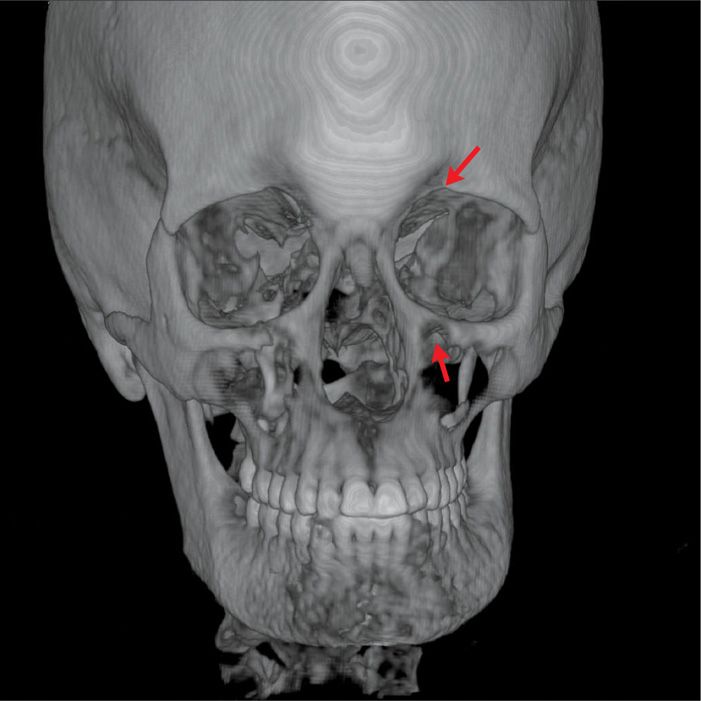
Figure 20-10. 3D reconstruction; supraorbital and infraorbital foramen. (Used with permission from Andrea Trescot, MD.)






Full access? Get Clinical Tree


