 Patient Position:
Patient Position: Supine, eyes closed in a central position.
 Indications:
Indications: Anterior eye segment surgery—cataract, trabeculectomy; posterior eye segment surgery—vitreoretinal surgery; conjunctival surgery, scleral buckle.
 Needle Size:
Needle Size: 22-gauge, 25-mm, normal bevel.
 Local Anesthetic Solution:
Local Anesthetic Solution: Half 0.5% or 0.75% bupivacaine, half 2% lidocaine, plus 100 to 150 IU/10 mL hyaluronidase.
 Volume:
Volume: 8 to 12 mL.
 Anatomic Landmarks:
Anatomic Landmarks: Inferotemporal orbit injection—third inferolateral border of the orbit; superonasal orbit injection—third superomedial border of the orbit.
 Approach and Technique:
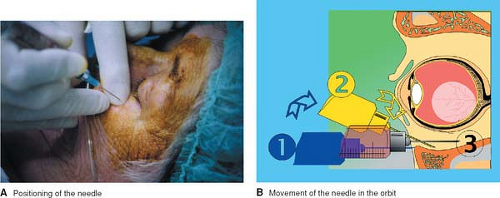
Approach and Technique: For an inferotemporal periconal injection, the needle is introduced perpendicular to the skin. After contact with the bony rim, the needle is moved slightly in the cranial direction to lose this bone contact, angled 30°, and introduced another 5 mm to a new periosteum contact. The needle is then moved back to the perpendicular position and progressively inserted to its full extent. After a negative blood aspiration, 6 to 8 mL of local anesthetic solution is injected. A good sign is a relative protrusion of the eye with a downward movement of the superior eyelid during the injection. Ocular tonicity must be checked continuously during the procedure
(Fig. 17-1).
For a superonasal periconal injection, the technique is similar to the one described for the inferotemporal injection. The needle is moved slightly in the caudal direction, and 2 to 4 mL of local anesthetic solution is injected
(Fig. 17-2).
After these injections, the globe is compressed for 5 to 10 minutes with a special device such as a Hoonan balloon. The low-pressure cuff allows for ocular compression of less than 30 mm Hg
(Fig. 17-3).


 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access




