CHAPTER 37
Perforated Tympanic Membrane
(Ruptured Eardrum)
Presentation
The patient experiences ear pain after barotrauma, such as a blow or slap on the ear, an exploding firecracker, a fall while water skiing or during a deep water dive, or after direct trauma inflicted with a stick or other sharp object, such as a paper clip or cerumen curette. Hemorrhage is often noticed within the external canal, and the patient will experience the acute onset of pain (which tends to subside quickly) and some partial hearing loss. Tinnitus or transient vertigo may also be present. Otoscopic examination reveals a defect in the tympanic membrane (TM) that may or may not be accompanied by disruption of the ossicles (Figure 37-1). The presence of blood may make assessment difficult.
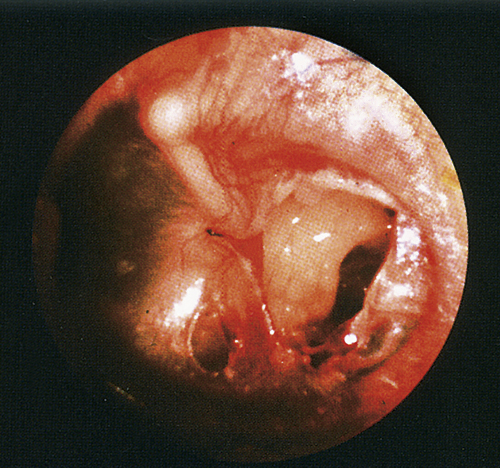
Figure 37-1 Small traumatic perforation of the tympanic membrane.
What To Do:
 When necessary, clear any debris from the canal, using gentle suction.
When necessary, clear any debris from the canal, using gentle suction.
 Determine if this is just an abrasion of the wall of the ear canal or if an actual TM perforation is present. If so, note its size and location.
Determine if this is just an abrasion of the wall of the ear canal or if an actual TM perforation is present. If so, note its size and location.
 Test for nystagmus and gross hearing loss.
Test for nystagmus and gross hearing loss.
 With a true TM perforation, place a protective cotton plug inside the ear canal, and instruct the patient to keep the canal dry by using soft wax earplugs while showering. He should also avoid submerging his head under water until the perforation is completely healed.
With a true TM perforation, place a protective cotton plug inside the ear canal, and instruct the patient to keep the canal dry by using soft wax earplugs while showering. He should also avoid submerging his head under water until the perforation is completely healed.
 Prescribe an appropriate analgesic, such as ibuprofen (Motrin), naproxen (Anaprox), or acetaminophen with hydrocodone (Lorcet) or with oxycodone (Percocet).
Prescribe an appropriate analgesic, such as ibuprofen (Motrin), naproxen (Anaprox), or acetaminophen with hydrocodone (Lorcet) or with oxycodone (Percocet).
 Prescribe the ototopical antibiotic ofloxacin (Floxin Otic) 5 mL, 3 to 5 drops in ear bid × 3 to 5 days, only if the lacerated TM and middle ear were contaminated with lake water, seawater, or a dirty object, such as a tree branch. Systemic antibiotics may be added in cases in which contamination is severe.
Prescribe the ototopical antibiotic ofloxacin (Floxin Otic) 5 mL, 3 to 5 drops in ear bid × 3 to 5 days, only if the lacerated TM and middle ear were contaminated with lake water, seawater, or a dirty object, such as a tree branch. Systemic antibiotics may be added in cases in which contamination is severe.
 Ensure that the patient gets early follow-up with an otolaryngologist. This is especially important with sharp, penetrating trauma in the posterior superior quadrant of the TM, where disruption of the ossicles is most likely to occur. The patient should be seen regularly until the TM is well healed.
Ensure that the patient gets early follow-up with an otolaryngologist. This is especially important with sharp, penetrating trauma in the posterior superior quadrant of the TM, where disruption of the ossicles is most likely to occur. The patient should be seen regularly until the TM is well healed.
What Not To Do:
 Do not suction or attempt to clear blood or debris close to the TM, if the canal is filled with clotted blood or if damage to the ossicles has occurred; vigorous suctioning may further traumatize these structures.
Do not suction or attempt to clear blood or debris close to the TM, if the canal is filled with clotted blood or if damage to the ossicles has occurred; vigorous suctioning may further traumatize these structures.
 Do not attempt to remove a foreign body you feel may have penetrated the middle-ear space. Consult an ear-nose-throat (ENT) specialist in these cases.
Do not attempt to remove a foreign body you feel may have penetrated the middle-ear space. Consult an ear-nose-throat (ENT) specialist in these cases.
 Do not instill any fluid other than Floxin Otic into the external canal or allow the patient to get water into his ear. Water in the middle ear is painful and irritating and may introduce bacteria. Wax earplugs or a cotton plug covered with petroleum jelly will allow the patient to shower more safely.
Do not instill any fluid other than Floxin Otic into the external canal or allow the patient to get water into his ear. Water in the middle ear is painful and irritating and may introduce bacteria. Wax earplugs or a cotton plug covered with petroleum jelly will allow the patient to shower more safely.
Discussion
Small uncomplicated perforations usually heal without sequelae over a period of days to weeks. Small defects (less than 2 mm) will heal spontaneously almost 100% of the time, but larger defects or marginal defects may not heal and would then require either myringoplasty or tympanoplastic procedures. When there is nystagmus, vertigo, profound hearing loss, or disruption of the ossicles, early otolaryngologic consultation is advisable.
If healing has not taken place after 8 weeks or if there is persistent hearing loss after healing, then surgical repair may be indicated.

Full access? Get Clinical Tree


