Chapter 28 Percutaneous Translaryngeal Jet Ventilation
I Introduction
Invasive airway management is relegated to the category of rescue techniques that one must know but hopes never to use. Students may be able to witness a surgical cricothyrotomy, and possibly to assist in the performance of an elective tracheostomy, but most anesthesiologists have successfully avoided incorporating these procedures into their practice. Although the modern airway armamentarium has made resorting to invasive procedures a rare event, the “cannot intubate, cannot ventilate” (CICV) scenario still occurs.1 By equipping the clinician with an alternative to routine upper airway management, the potential for rescuing a failed airway and preventing devastating adverse outcomes is substantially increased.
Multiple studies have indicated that the incidence of the CICV scenario is between 0.01 and 2.0 cases per 10,000 anesthesias.1–3 Although the root cause of this dire apneic or obstructive state may be fully or partially related to the patient’s disease, it often has an iatrogenic component, being recognized at the time of anesthetic induction or as a result of other interventions. The American Society of Anesthesiologists (ASA), The Difficult Airway Society, and The Advanced Trauma Life Support guidelines, as well as the opinions of other expert organizations, concur that, although invasive airway access is rarely practiced or prepared for, this capability must be at the fingertips of any operator who is charged with airway management.4–6 The conditions that commonly require the use of invasive airway access include facial fractures (32%), blood or vomit in the airway (32%), traumatic airway obstruction (7%), and failed intubation in the absence of other indications (11%).7 A completely obstructed airway state does not have to exist for a patient to be at jeopardy. Any time the clinician cannot ensure adequate, life-sustaining gas exchange by virtue of a problem within the conveyance portions of the respiratory tract, further actions (noninvasive or invasive) are mandatory.
Although surgical cricothyrotomy has long been a standard of emergency invasive airway rescue, its use has declined, in part because of advances in noninvasive airway devices such as supralaryngeal airways (SLAs) and video laryngoscopes, the adoption of pharmacologic agents for rapid-sequence intubation in the emergency department, and increased requirements for trainee supervision.8
There is widespread agreement in the literature that percutaneous translaryngeal jet ventilation (PTJV),5 using a small-bore catheter placed through the cricothyroid membrane (CTM), is a simple and effective treatment for the desperate CICV situation.8,9 Compared with surgical cricothyrotomy and tracheostomy, the establishment of PTJV is ordinarily quicker, simpler, and therefore more efficacious for most anesthesiologists, who may not be practiced in more formal surgical techniques.8,10 This may not hold true for the infant or small child, however. Although PTJV was faster to achieve than a surgical airway, it had an exceedingly high failure rate (83%) in a swine model of the juvenile population.11 This is likely due to the lack of circumferential support offered by the immature cricoid cartilage.
A A Note on Nomenclature
The literature is replete with descriptions of PTJV techniques and of a number of devices, both commercial and “operating room [OR] rigged.”12–16 As discussed here, many of these OR-rigged PTJV setups have not undergone objective testing; although they are easy to construct, they may not be practical, robust, or life-sustaining.
II Incorporating Percutaneous Translaryngeal Jet Ventilation into the Difficult Airway Plan
The 2003 ASA difficult airway (DA) algorithm lists three techniques that should be employed when circumstances are encountered in which one cannot intubate (i.e., via direct laryngoscopy) and cannot ventilate, either by bag-mask or with the use of a laryngeal mask airway (LMA; LMA North America, Inc., San Diego, CA). These techniques are insertion of an esophageal-tracheal Combitube (ETC; Ambu, Copenhagen, Denmark), use of PTJV, and provision of an emergency surgical airway. Because the LMA and ETC are familiar to most anesthesiologists, both of these noninvasive airways should be considered first in cases of supraglottic obstruction, unfavorable anatomy, or other CICV situations. Both have been demonstrated to be highly effective in this setting and are generally considered atraumatic.4,17,18 Though other SLAs are likely to be as applicable, they are not mentioned in the 2003 practice guidelines. Whether or not future guideline revisions call for other devices or refer to generic SLAs, operator experience and comfort should guide choice. The preferred device should be immediately available whenever the possibility of a CICV situation might arise.17
If insertion of an SLA does not affect gas exchange quickly, the ASA DA algorithm recommends that the clinician move to an invasive airway access maneuver without hesitation or delay. Of the maneuvers suggested, PTJV may be the most familiar to the anesthesiologist. A distinct advantage of PTJV over surgical cricothyrotomy is that it can be practiced in nonemergency clinical care. The anesthesiologist who is practicing elective, awake intubation may choose to make the percutaneous transtracheal injection of lidocaine a routine technique, thereby practicing laryngeal catheter placement, and some have advocated the placement of prophylactic transtracheal catheters in high-risk airway situations or for elective laryngeal surgery.19 It should be noted that severe subcutaneous emphysema is a rare complication of translaryngeal lidocaine injection, even in otherwise uncomplicated cases.20
III Incidence and Complications
Barotrauma with resultant pneumothorax and hemodynamic changes has been reported with both emergent and elective use of PTJV.8,19,21–31 In a retrospective chart review, Patel and associates described a 53-month experience with patients in acute respiratory failure in the intensive care unit.21 Of the 352 patients requiring endotracheal intubation, 29 emergent PTJV attempts were made. The procedure was performed by house staff (n = 5) and attending physicians (n = 24). Successful cannulation of the airway was achieved in 79% of patients. Subcutaneous emphysema occurred in 2 of these patients. Orotracheal intubation was subsequently required in 22 patients, with 1 requiring a surgical tracheostomy. PTJV failed in 6 patients. These failures were attributed to recent thyroid surgery (n = 1), obesity (n = 2), kinking of the PTJV cannula (n = 2), and misplacement of the cannula (n = 1). Subcutaneous emphysema was seen in only 1 patient for whom PTJV failed. The other patient who suffered subcutaneous emphysema experienced severe pneumomediastinum treated with bilateral chest tubes. Of the 6 patients with failed PTJV, 2 were subsequently orally intubated with the aid of a bougie, and the remaining 4 died.
Smith and colleagues reported a 29% incidence of complications in 28 patients managed with PTJV to provide an emergency airway.22 These complications included subcutaneous emphysema (7.1%), mediastinal emphysema (3.6%), exhalation difficulty (14.3%), and arterial perforation (3.6%), none of which were fatal. Other complications, such as esophageal puncture, bleeding, hematoma, and hemoptysis, have been also reported after PTJV.23
In a review of 265 elective PTJV and other forms of jet oxygenation/ventilation for otolaryngologic surgery, Jaquet and colleagues wrote that PTJV was associated with hemodynamic instability (8 patients), subcutaneous emphysema of the neck (3 patients), posterior tracheal mucosa tear (1 patient), catheter kinking (3 patients), severe mediastinal/cervical subcutaneous emphysema (1 patient), unilateral pneumothorax (1 patient), and bilateral pneumothorax (1 patient).19 The last 3 events were considered major complications, and all were associated with cough or laryngospasm during PTJV. Damage to the tracheal wall, witnessed by this group, was also demonstrated in a large-animal model of PTJV in which full-thickness erosion and hemorrhage of posterior tracheal mucosa was seen in all specimens.29 Subcutaneous emphysema has been associated with cannula shaft lacerations in the absence of frank cannula misplacement.30
In another series of elective PTJV cases, there was an overall minor complication rate of 3%.22 These complications (minor bleeding, subcutaneous emphysema) were typically seen when multiple attempts had to be made during cannula placement. The authors recommended that no more than two attempts should be made.
The site of PTJV access may also influence complications. In a swine tracheal model, Salah and coworkers studied trans-CTM versus transtracheal cannulation. With some percutaneous techniques, traumatic injury (including posterior wall tears or frank penetration and cartilaginous fractures) were more common when the PTJV cannula was inserted into the trachea.31
Complete or near-complete airway obstruction during PTJV may also contribute to hemodynamic instability.24 In a controlled trial employing graded airway obstruction in dogs undergoing PTJV with 45 psi inflation pressures through a 13-G catheter, intratracheal pressures of 24 cm H2O were associated with decreasing blood pressure and increased central venous pressure, even in the absence of pneumothorax. In complete upper airway obstruction simulated in dogs, intratracheal airway pressure rose precipitously as soon as the total lung capacity was exceeded. This was accompanied by a fall in systolic blood pressure and eventual rupture of the pulmonary system (pneumothoraces, pneumomediastinum, subcutaneous emphysema, cardiac fibrillation) when an intratracheal pressure of 250 cm H2O was achieved.25
In one canine study, methylene blue instilled into the oral cavity was less readily aspirated into the trachea during PTJV, compared with controls.26,27 The authors reasoned that the retrograde egress of gas from the larynx reduced oral content aspiration. A similar phenomenon has been noted in humans during O2 insufflation through an endotracheal tube (ETT) exchange catheter.28
A Mechanism of Barotrauma and Other Forms of Airway Trauma
Striving to verify the intraluminal position of a percutaneously placed cannula is mandatory during PTJV. Though cannula misadventures are responsible for many of the complications related to PTJV, complete upper airway obstruction during O2 insufflation is likely responsible for most episodes of barotrauma. During involuntary obstruction of the upper airway (e.g., due to laryngospasm) intraluminal pressures, generally remaining in the safe range of 18 to 25 cm H2O during PTJV, rise precipitously. In an artificial lung model, upper airway obstruction (airway resistance 200 cm H2O/L/sec) resulted in an intratracheal pressure of 60 cm H2O. Intraluminal pressures between insufflations did not rise above minimal levels (3 cm H2O) until maximal airway resistance was produced, at which time there was an equilibration to maximal pressure.32 In an adult sheep model, complete airway obstruction during constant tracheal insufflation of O2 at 15 L/min resulted in a pressure of 96 cm H2O in 12 seconds. When intermittent jet ventilation (JV) was used (inspiratory-to-expiratory [I : E] phase ratio, 3 : 5), a pressure of 108 cm H2O was reached in 33 seconds.25
IV Cannula Size and Oxygenation
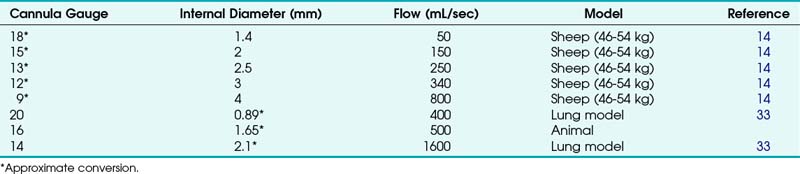
A wide variety of cannula-over-needle devices have been described in the PTJV literature in both in vivo and mechanical model trials and in case reports. Trials of cannulas smaller than 3 mm in diameter (equivalent to 8 G) have typically demonstrated the need for a high-flow regulator/conveyance apparatus. Although flow through cannulas of various diameters and lengths has been measured during simulated PTJV, actual flow varies with the clinical situation and is affected by factors such as airway resistance and pulmonary compliance. Table 28-1 lists experimental data on flow rates through cannulas of various sizes with the use of a 50 psi gas supply.14,33,36
Neff and colleagues insufflated gas through cannulas of various diameters in a sheep model.25 Marginal oxygenation was achieved with a 1.4-mm-diameter (15-G) cannula using 15 L/min constant and 50-psi “pulsed” O2 flow. Use of low-pressure systems, such as resuscitator bags and anesthesia machine circuits, which provide 1 to 2 psi, was futile for catheters smaller than 3 mm in diameter. However, Zornow and colleagues were able to produce “delayed” reoxygenation in a hypoxic swine model with a 14-G cannula and “vigorous” ventilation with an anesthesia machine circuit.25,29 O2 resuscitation was significantly faster when 50-psi supplies were used (15 versus 120 seconds).25
Some authors have speculated that entrainment of room air via a Venturi effect produced by the high velocity of the gas injected into the larynx during PTJV might add as much as 40% or 50% to the volume of inspired gas.33–35 This hypothesis has been contradicted by the findings of arterial blood gas studies in both animals and healthy patients undergoing jet ventilation, which demonstrated O2 tensions consistent with the insufflation of 100% O2 (no entrainment of room air).36–38
Whereas complete upper airway obstruction has been associated with ineffective ventilation and barotrauma, partial obstruction may enhance both oxygenation and ventilation by driving gas flow toward the lower bronchial tree, facilitating tidal volume (VT) and improving alveolar oxygen tension (PaO2).24
V Ventilation
Effective ventilation during PTJV requires a pathway for gas egress. Fortunately, most patients who present with life-threatening airway failure (e.g., laryngeal edema, epiglottitis, laryngeal tumor) have isolated inspiratory obstruction with no or partial expiratory obstruction.39 This is true during spontaneous breathing as well as controlled ventilation through a face mask or SLA, and it is related both to the extrathoracic position of the upper airway and to the architecture of laryngeal and supralaryngeal structures. Complete obstruction to gas escape is a contraindication for PTJV and may be dependent on the devices used.
Because removal of CO2 is dependent on sufficient volumes of gas entering and exiting the lung, low-pressure systems (e.g., resuscitation bags) are generally inadequate for ventilation, as they are for oxygenation. Zornow and colleagues, using a 14-G transtracheal cannula in a swine model, was able to effectively ventilate with a 50 psi O2 source but could not reduce arterial CO2 despite “vigorous” ventilation with an anesthesia machine circuit.29 Whereas gas escaping from an in vivo ETT could be measured when PTJV was performed with the high-pressure source, no gas movement was appreciated with use of the low-pressure system.
Ward and coworkers examined no, partial, and complete upper airway obstruction during PTJV in dogs, using 13-G catheters and a high-flow regulator delivering 45 psi of pressure.40 With no or partial upper airway obstruction, CO2 levels decreased during PTJV. Partial airway obstruction improved CO2 removal, possibly by promoting improved alveolar expansion during the O2 injection phase of PTJV.
A Airway Rescue in Complete Upper Airway Obstruction
Although controversial and based on animal models, low-flow insufflation of O2 into the pulmonary circuit has been proposed as a mechanism for maintaining oxygenation, although not effective ventilation, in the patient with a completely obstructed airway.24,41,42 Several alternative techniques have been studied in the model of complete upper airway obstruction.
Frame and associates, using a canine model (20 to 29 kg), found that with complete airway obstruction, O2 flows of 5 to 7 L/min through 10-G and 12-G catheters could maintain oxygenation with I:E phases of 1 : 4 seconds and provided reasonable ventilation (PaCO2 <75 mm Hg).41 When lower flow rates (3 L/min) were used, CO2 tension increased rapidly after 5 to 20 minutes. Although this study demonstrated the successful use of low-pressure O2 flow in complete airway obstruction (in an effort to avoid barotrauma), it must be cautioned that small animals and large insufflation catheters were used.
Low-flow translaryngeal rescue insufflation of oxygen (LF-TRIO) of as little as 2 L/min has been shown to maintain oxygenation in a large animal model (34-kg swine) for upwards of 60 minutes.5 LF-TRIO recovered the animals from O2 saturation nadirs of 50% in an average of 23 seconds. Cardiovascular parameters were stable in all animals for a minimum of 15 minutes. Although the animals experienced hypercapnia, the authors argued that this may be well tolerated if there are no specific comorbidities that may be aggravated by increasing CO2 (e.g., head trauma). Although imaging in this study was limited to a small number of animals, there was no evidence of microatelectasis after 1 hour of LF-TRIO. LF-TRIO was considered by these authors to be a short-term rescue option when definitive surgical airway control is anticipated.
More recently, the concept of an active expiratory phase has been applied to PTJV (Fig. 28-1). In a series of large-animal studies, Enk and Hamaekers described using the O2 flow from a standard flowmeter to create a negative-pressure, transcatheter expiratory phase.32 Bernoulli’s principle, application of which is familiar to anesthesiologists in the functioning of the Venturi valve, states that when a fluid in a vessel passes through a constriction, dynamic energy (speed of flow) is increased, whereas static pressure (potential energy) exerted on the vessel side-wall is diminished. This setup can be manipulated to produce a subatmospheric pressure during an expiratory phase of PTJV. In an initial bench model, a prototype expiratory ventilation assistance (EVA) device reduced by half the time required for a 1000-mL injected VT to be expired via a 2-mm ID cannula and also increased the effective minute ventilation by 33%.32 In another large-animal study by the same group that included a complete obstruction of the upper airway, EVA restored oxygenation within 10 seconds and limited hypercarbia over 15 minutes.42 However, EVA was less effective when the upper airway was unobstructed, possibly due to preferential entrainment of ambient air into the PTJV catheter via the lower-resistance upper airway path and, consequently, reduced removal of alveolar gases.43

B Percutaneous Translaryngeal Jet Ventilation in Relief of Upper Airway Obstruction
The introduction of PTJV may encourage partial relief of upper airway obstruction. In a controlled study, Okazaki and colleagues demonstrated that induced airway obstruction (by simple neck flexion) was partially relieved by the insufflation of 10 L/min O2, although not as well as by the chin lift–jaw thrust maneuver.44 This finding implies a potential utility of transtracheal insufflation in patients who are at high risk for airway obstruction during postanesthesia recovery.44,45
VI Elective Indications
A To Facilitate Operations of the Upper Airway
There have been several reports and various recommendations for the elective use of PTJV in surgical procedures to avoid tracheostomy, provide an unobstructed surgical field, or facilitate safe ETT. Singh and coworkers reported on 1500 cases of PTJV for diagnostic and surgical procedures of the upper airways, including bronchoscopy and esophagoscopy (n = 1257) and endolaryngeal surgery (n = 135).46 PTJV support was continued for 24 to 48 hours into the postoperative period in 108 cases. Spoerel and Greenway, describing ventilation techniques during endolaryngeal surgery, similarly found adequate pulmonary ventilation with excellent conditions for microscopic surgery.47 Smith and colleagues reported on elective transtracheal ventilation in children undergoing surgical procedures involving the head and neck.48 They described the use of this technique in two children, one undergoing an operation for laryngeal stenosis and one who became obstructed and cyanotic in the recovery room. PaCO2 measurement at the end of the procedures indicated that the patients were moderately hyperventilated. Similarly, because PTJV leaves the entire airway from the vocal cords to the face accessible for surgical manipulation, it is not surprising that its elective use has been described for a large variety of procedures on these structures in adults.49 In addition, Wagner and coauthors described a case in which high-frequency JV was used with success (thus avoiding tracheostomy) in a patient with a partial upper airway obstruction caused by a hypopharyngeal foreign body with sharp appendages.50
Dhara and colleagues reported on two cases in which a triple-lumen central venous catheter was placed through the CTM before induction of anesthesia.51 Making use of all three lumens, this unique approach allowed the clinicians to measure tracheal CO2 and intra-airway pressure, as well as providing jet oxygenation. In both cases, an upper airway egress for insufflated O2 was maximized by use of a nasopharyngeal airway (NPA) or tongue retraction.
Depierraz and associates investigated the elective use of PTJV in pediatric patients (aged from less than 1 to 12 years) with significant upper airway obstruction.52 They recited the major advantages of this technique: improved surgical exposure of the upper airway obstructive lesion, reduced manipulation of the lesion, reduced operative field movement during laser surgery, reduced danger of airway fire, and reduced risk of blowing particles into the distal airway.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Ultrasonography in Airway Management
Ultrasonography in Airway Management
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


