(1)
Department of Anaesthesia, Pamela Youde Nethersole Eastern Hospital, Hong Kong, China
(2)
University of Alberta, Edmonton, AB, Canada
(3)
Department of Anesthesiology and Pain Medicine, University of Alberta, Edmonton, AB, Canada
(4)
Department of Anesthesiology and Pain Medicine, University of Alberta and University of Alberta Hospital and Stollery Children’s Hospital, Edmonton, AB, Canada
Femoral Nerve Block
Introduction, Indications, and Complications
The femoral nerve is a mixed sensory and motor nerve. The motor fibers supply the quadriceps femoris, sartorius, and pectineus muscles, while the sensory fibers innervate the anterior thigh and medial aspect of the knee and lower leg. The nerve is formed from the posterior divisions of the L2–L4 roots. After emerging at the lateral border of psoas, it descends between the psoas and iliacus muscles underneath the fascia iliaca and runs beneath the inguinal ligament into the thigh, lateral to the femoral sheath.
Femoral nerve block is a relatively safe and easy block that is performed commonly in children. It is indicated in the management of femoral fracture, providing pain relief and muscle relaxation to facilitate transport, examination, and manipulation of the fracture. It also offers postoperative analgesia for surgery on the knee and quadriceps tendon. Occasionally, it is used to provide surgical anesthesia for muscle biopsy and skin grafting of the anterior thigh. Complete anesthesia below the mid-thigh can be achieved if it is performed in combination with a sciatic nerve block.
Patient Positioning, Preparation, Equipment, and Dosage
The patient lies supine and the leg is slightly externally rotated. The skin is cleaned with antiseptic solution. If ultrasound is used, prepare the probe surface by applying a sterile adhesive dressing.
A 50-mm, 22-G short-beveled needle is used. An insulated needle should be chosen if nerve stimulation is used. The recommended local anesthetic dose is 0.2–0.5 mL/kg of 0.25 % bupivacaine or 0.2 % ropivacaine without exceeding the toxic dose limits (2 mg/kg for bupivacaine and 3–4 mg/kg for ropivacaine without epinephrine). The dose for the femoral block should be decreased if an additional sciatic nerve block is planned.
Nerve Stimulation Technique
The point of needle insertion is approximately 0.5–1 cm lateral to the femoral artery at the inguinal crease (which is about 0.5–1 cm below the inguinal ligament) (Fig. 72.1). This insertion point may vary according to the age and weight of the child. The needle is inserted at 30–45° to the skin, pointing cephalad. Advance the needle until “patellar twitch” (contraction of quadriceps femoris muscle) is obtained. The current is initially set at 0.8–1 mA (1 Hz, 0.1–0.2 ms) and then gradually reduced to a threshold current of 0.5 mA. Currents less than 0.3 mA indicate intraneural placement, and the needle should be withdrawn slightly. As the needle is advanced, two “pops” or “gives” can be felt as the needle passes through the fascia lata and fascia iliaca, respectively. Local anesthetic is injected after the second “pop” following negative aspiration. Depending on the age and size of the patient, the depth of insertion is usually around 0.5–1 cm.
Fig. 72.1
Surface anatomy and landmarks for femoral nerve block
Ultrasound-Guided Technique
A high-frequency (13-6 MHz) linear probe is suitable for this block. In small children, a small footprint (“hockey stick”) probe is desirable. The probe is placed in a transverse plane along the inguinal crease to obtain a transverse view of the femoral artery and the vein (Fig. 72.2). The nerve, which often appears oval or triangular shaped, is located lateral to the femoral artery and just underneath the hyperechoic fascia iliaca. Color Doppler may be used to identify the vessels. The femoral artery is anechoic, circular, and pulsatile, whereas the femoral vein is more irregular in shape, compressible, and located medial to the artery. If localization of the nerve is difficult, scan distally to look for the profunda femoris artery and trace it proximally to the point where it joins the femoral artery. The femoral nerve is usually found lateral to the artery.
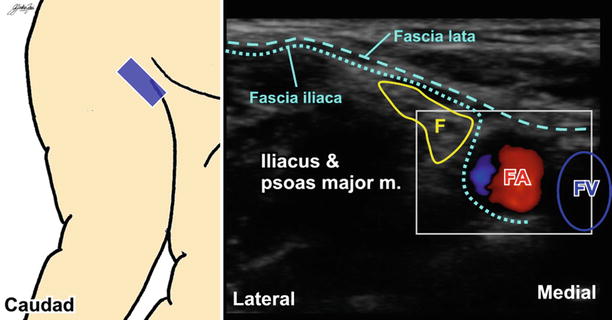
Fig. 72.2
Ultrasound image of major anatomical structures surrounding the femoral nerve. F femoral nerve, FA femoral artery, FV femoral vein
Both in-plane and out-of-plane techniques can be used. For the in-plane approach, the needle is inserted at the lateral edge of the probe and angled medially to reach the nerve. Two “pops” or “gives” are felt as the needle penetrates the fascia lata and fascia iliaca. When using the out-of-plane approach, the nerve is centered in the middle of the screen, and the needle is inserted at 0.5–1 cm away from the midpoint of the caudad edge of the probe at 45° to the skin. The needle then “walks down” to reach the nerve while maintaining the needle tip in view. A test dose of D5W can visualize spread and confirm nerve localization prior to injection of local anesthetic.
Lateral Cutaneous Nerve Block
Introduction, Indications, and Complications
The lateral cutaneous nerve of the thigh is a pure sensory nerve that innervates the lateral thigh up to the knee. It arises from the posterior branches of the L2 and L3 roots. After emerging from the lateral border of the psoas muscle, the nerve runs obliquely towards the anterior superior iliac spine (ASIS) beneath the fascia iliaca. It then passes underneath the inguinal ligament at a point approximately one fingerbreadth medial to the ASIS and then enters the thigh deep to the fascia lata, where it divides into anterior and posterior branches to supply the skin of the lateral thigh.
This block is indicated for procedures involving the lateral thigh, for example, muscle biopsy, skin grafting, and hip or femur operations with lateral incisions. Very often, it is performed in conjunction with femoral and sciatic nerve blocks for upper thigh surgery. Occasionally, it is used to diagnose meralgia paresthetica, a condition that presents with pain and numbness of the outer thigh as a result of the entrapment of the lateral cutaneous nerve of the thigh.
Patient Positioning, Preparation, Equipment, and Dosage
The child lies supine with the leg externally rotated. Clean the skin with antiseptic solution. If ultrasound is used, prepare the probe surface by applying a sterile adhesive dressing.
A 50-mm, 22-G short-beveled needle is used. Local anesthetics of choice are 0.25 % bupivacaine and 0.2 % ropivacaine. A volume of 1–3 mL (up to a maximum of 10 mL) is adequate.
Landmark Technique
Nerve stimulation is not used for this block since the nerve is purely sensory and monitoring paresthesia is often impossible for children. The point of needle insertion for the landmark technique is approximately 0.5–1 cm (depending on the age and size of the child) medial to the ASIS and below the inguinal ligament. Advance the needle until a “pop” is felt as the fascia lata is penetrated. Local anesthetic is deposited at this point.
Ultrasound-Guided Technique
A small footprint (“hockey stick”) high-frequency (13-6 MHz) probe is used. The probe is placed in a transverse plane along the inguinal crease with the lateral end over the ASIS. The nerve, which is often oval shaped, is usually seen 0.5–1 cm medial and inferior to the ASIS, between the fascia lata and fascia iliaca (Fig. 72.3). The nerve is superficial and can be difficult to identify. The hyperechoic nerve will be better visualized after injection of hypoechoic D5W or local anesthetic, which expands the fascial plane.
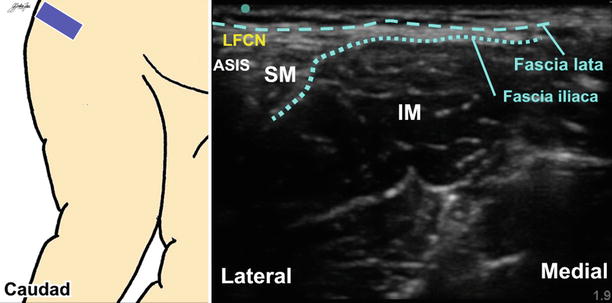
Fig. 72.3
Ultrasound image of the lateral femoral cutaneous nerve (LFCN) between the fascia lata and fascia iliaca. ASIS anterior superior iliac spine, SM sartorius muscle, IM iliacus muscle
Both in-plane and out-of-plane techniques can be used. For the in-plane approach, the needle is inserted in either a lateral-to-medial or medial-to-lateral direction. When using the out-of-plane approach, the nerve is centered in the middle of the screen, and the needle is inserted 1 cm away from the caudad edge of the probe at 45° to the skin. The needle then “walks down” to reach the nerve between the fascial planes while maintaining the needle tip in view. A test dose of D5W can visualize spread and confirm nerve localization prior to injection of local anesthetic.
Obturator Nerve Block
Introduction, Indications, and Complications
The obturator nerve is a mixed sensory and motor nerve. The motor fibers supply the adductor muscles (adductor longus, adductor brevis, adductor magnus, and gracilis). The sensory fibers innervate the medial thigh and the hip and knee joints. The nerve is derived from anterior divisions of the L2–L4 roots. After emerging from the inner border of the psoas, the nerve descends medially and posteriorly in the pelvis, close to the lateral wall of the bladder. The nerve exits the pelvis via the obturator foramen, splitting into anterior and posterior branches which enter the thigh. The anterior branch runs between the adductor longus and adductor brevis, supplying the adductor muscles, the hip joint, and the skin of the medial thigh. The posterior branch travels between the adductor brevis and adductor magnus, supplying the adductors and the knee joint.
Indications for obturator nerve block include relieving adductor spasm and treatment of pain in the hip and knee when combined with femoral block. Several approaches have been described to block the obturator nerve, for example, the psoas compartment block, iliaca compartment block, and the 3-in-1 block. The success rates of these approaches vary, and some approaches can be difficult to perform. Also, accidental puncture of the obturator arteries is a potentially life-threatening complication. The use of ultrasound allows isolated blockade of the nerve with increased success and safety and is highly recommended.
Patient Positioning, Preparation, Equipment, and Dosage
The leg is externally rotated and the knee slightly flexed to expose the medial thigh. The skin is cleaned with antiseptic solution. Prepare the probe surface by applying a sterile adhesive dressing if ultrasound is used.
A 50-mm, 22-G insulated needle is used. Choices of local anesthetic include 0.25 % bupivacaine and 0.2 % ropivacaine. Usually, a volume of 0.25 mL/kg (maximum 10 mL) is required for each interfascial plane. The depth is approximately 4–6 cm.
Nerve Stimulation Technique
The point of needle insertion is 0.5–1 cm (depending on the age and size of the child) lateral and caudal to the pubic tubercle (Fig. 72.4), where the nerve just passes underneath the inguinal ligament before bifurcation. Advance the needle until it contacts the superior pubic ramus and then walk the needle off the inferior border of the superior pubic ramus to enter the obturator foramen. Redirect the needle laterally and cephalad and advance slowly until twitches of the adductor muscles are observed. The initial current is set at 0.8–1 mA (1 Hz, 0.1–0.2 ms) and decreased slowly to a threshold current of 0.5 mA. Local anesthetic is deposited after careful aspiration.
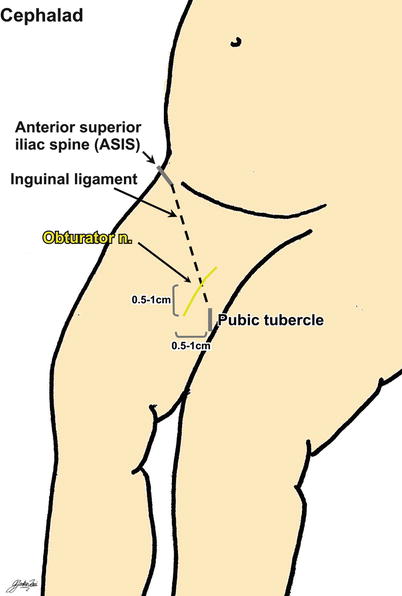
Fig. 72.4
Surface anatomy for obturator nerve block
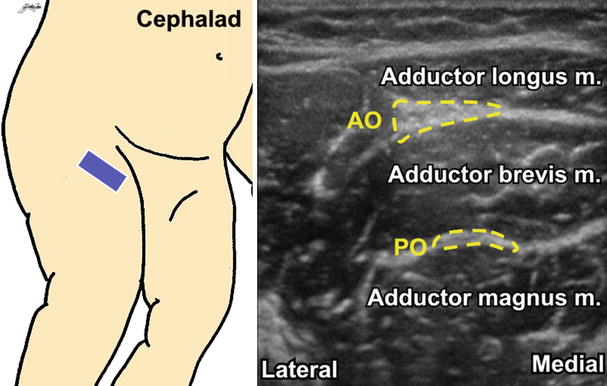
Ultrasound-Guided Technique
A 13-6 MHz linear probe is suitable for this block. The probe is placed in a transverse plane below the inguinal crease (around 2–3 cm inferior to the inguinal ligament) (Fig. 72.5). After locating the femoral vessels, scan medially to identify the pectineus muscle which is medial to the femoral vein. The three adductor muscles (adductor longus, adductor brevis, and adductor magnus, from superficial to deep) can be found medial to the pectineus. As the branches of the obturator nerve are usually too small to be seen, the aim for this technique is to perform two fascial blocks (injection between the fascial planes through which the branches pass).