Fig. 34.1.
Right adductor tear with secondary cleft sign (fluid in pubic symphysis).
Fig. 34.2.
Right rectus avulsion injury with secondary cleft (sagittal view).
Fig. 34.3.
Right rectus avulsion with secondary cleft (axial view).
Fig. 34.4.
Left adductor tear with adductor edema and secondary cleft.
Diagnosis
Bilateral athletic pubalgia with MRI demonstrating bilateral rectus abdominis and adductor avulsions from their insertions on the pubis.
Nonoperative Management Options
Conservative treatment is the first-line therapy for musculoskeletal strains of the groin. Nonsurgical strategies include anti-inflammatory medications, deep massage, heat or ice, and prolonged rest followed by gradual return to activity. Physical therapy may be effective and should focus on core strengthening to allow for resolution of hip and pelvic muscular imbalance. In patients with radiographic and clinical evidence of osteitis pubis and/or adductor tendinopathy, fluoroscopically guided injection of the symphysis pubis and adductor origin with local anesthetic and/or steroids may be effective.
Operative intervention is generally indicated for chronic pain of greater than 2–3 months duration that is refractory to conservative management, including prolonged rest, physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDS), nerve blocks, and/or steroid injections.
For this patient, nonoperative treatment strategies had been employed for 6 months without significant improvement in symptoms. Further attempts at rehabilitation were felt unlikely to provide relief. Surgical intervention was offered.
Operative Treatment
Laparoscopic Bilateral Transabdominal Pre-peritoneal (TAPP) Repair
The technique utilized for sports hernia repair is identical to the standard repair of inguinal hernias and is well described in the literature. Briefly, a three-port technique is used, with a Hasson cannula at the umbilicus and one 5-mm port lateral to the rectus on either side of the umbilicus. The peritoneum is sharply opened at the medial umbilical ligament in a curvilinear fashion extending laterally. The pre-peritoneal space of Retzius is entered medially and the bladder bluntly dissected away from the pubis and Cooper’s ligaments. The inferior peritoneal flap is retracted and the cord structures are dissected away from the peritoneum. Any direct or indirect inguinal hernia defects are reduced. The posterior aspect of the rectus insertion is inspected to confirm evidence of attenuation or avulsion injuries of the rectus insertion onto the pubis.
After development of a wide pre-peritoneal pocket bilaterally, a large polypropylene mesh (minimum 12 × 15 cm) is used to reinforce the entire myopectineal orifice on each side. Bilateral mesh prosthetics are confirmed to overlap in the midline in order to provide for complete reinforcement of the entire myopectineal orifice, Cooper’s ligaments, and the pubic tubercle (Figs. 34.5 and 34.6). The mesh is secured with several tacks or staples to Cooper’s ligament and then further secured circumferentially with fibrin glue. No tacks or staples are placed into the abdominal wall musculature and no mechanical fixation is utilized below the iliopubic tract. The peritoneum is re-approximated. The same procedure is performed for the contralateral groin in order to allow for wide coverage of all potential inguinal defects on both sides.
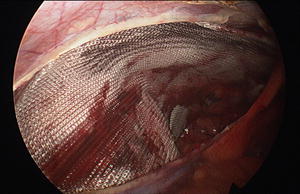

Fig. 34.5.
After development of a wide pre-peritoneal pocket, a large polypropylene mesh (minimum 12 × 15 cm) is used to reinforce the entire myopectineal orifice (left side).
Fig. 34.6.
Polypropylene mesh reinforcement of the myopectineal orifice (right side). Note mesh overlap of pubic tubercle in the midline.
Postoperative Course
The patient was discharged to home following surgery and seen in follow-up at 2 weeks and at 6 weeks postoperatively. His postoperative course was uncomplicated and he returned to activity following our sports hernia physical therapy protocol (Table 34.1). He began aerobic activity 2 weeks following surgery and gradually progressed to range of motion exercises and resumption of dynamic core training over the following month. He returned to light sporting activity at 6 weeks and was allowed to resume full activity including football 2 months postoperatively. He was able to compete at the collegiate level during the fall football season several months later. He had a successful senior season as a tight end and on special teams as a long snapper.
Table 34.1.
Sports hernia repair postoperative protocol.
Phase I: Immediate postoperative phase (weeks 0–2) |
Pain and edema control, gentle stretching, walking |
Phase II: Intermediate postoperative phase (weeks 2–3) |
Gentle strengthening/pelvic stabilization, light exercise (pool, bike) |
Phase III: (Weeks 3–4) |
Range of Motion, strengthening, dynamic core training, straight plane jogging |
Phase IV: (Weeks 4–5) |
Light sport specific activity, plyometrics, interval bike training |
Phase V: (Weeks 5–6) |
Return to full sport activity |
General recommendations |
Avoid trunk hyperextension for first 2 weeks |
Avoid hip extension past 0° for first 2 weeks |
Avoid crunch and lifting activities for first 6 weeks |
Pain and edema control, ice 3–4 times per day as needed for first week, as needed thereafter |
Return to work and sport to be determined on an individual basis by the physician and physical therapist |
Outcomes and Discussion
Chronic groin pain in the athlete can be disabling and in some cases career-ending. The exact cause is debated but is theorized to be due to repetitive loading of the pubic symphysis, leading to symphyseal degeneration and loss of mechanical stability. Shearing forces across the pubic symphysis are more prominent in athletes with an imbalance between the strong adductor muscles of the thigh and the relatively weaker lower abdominal wall musculature. These factors are believed to cause weakness and attenuation of the transversalis fascia portion of the posterior wall of the inguinal canal. Weakness in the inguinal floor can lead to localized bulging and compression of the genital branch of the genitofemoral nerve, which is believed to be a source of pain in these patients. Other proposed pathophysiologic mechanisms of injury remain an area of debate and include disruption of the conjoined tendon as well as tears of the rectus abdominis and adductor longus aponeurosis at the point of insertion on the pubis [1].
Related posts:
 Introduction to Primary and Secondary Groin Pain: What Is Inguinodynia?
Prevention of Pain: Optimizing the Laparoscopic TEP and TAPP Techniques
Prophylactic Neurectomy Versus Pragmatic Neurectomy
Patient with Referred Hip Pain
Introduction to Primary and Secondary Groin Pain: What Is Inguinodynia?
Prevention of Pain: Optimizing the Laparoscopic TEP and TAPP Techniques
Prophylactic Neurectomy Versus Pragmatic Neurectomy
Patient with Referred Hip Pain
 Chronic Pelvic Pain in Women
Chronic Pelvic Pain in Women
 Groin Pain Etiology: Hip-Referred Groin Pain
Groin Pain Etiology: Hip-Referred Groin Pain

Full access? Get Clinical Tree


