Figure 10.1. Relationship between the spinous processes, transverse processes, and spinal nerves in the lumbar and thoracic spine. The lumbar spinal nerves course caudad to the transverse process of the vertebrae for which they are named.
III. Indications
A. Paravertebral block is indicated any time a dermatomal block distribution is desired. It is particularly useful when a strictly unilateral block is desired.
1. Caveat. Because innervation overlaps across the midline, areas near the mid-line may not be adequately blocked by unilateral paravertebral (or intercostal) block. Similarly, there is overlap between adjacent dermatomes on the same side so that it is almost always necessary to place blocks one dermatomal level above and below the desired level(s) to assure complete block of the targeted dermatome(s).
B. Outpatient surgery. Paravertebral block is well suited to outpatient surgery because it generally does not impair the sympathetic nervous system as extensively as does epidural/spinal anesthesia and can produce analgesia lasting 10 hours or more with long-acting local anesthetics. Also, unlike central neuraxial block, paravertebral block is unlikely to affect micturition or to significantly impair lower extremity motor function (above L2), which should speed discharge.
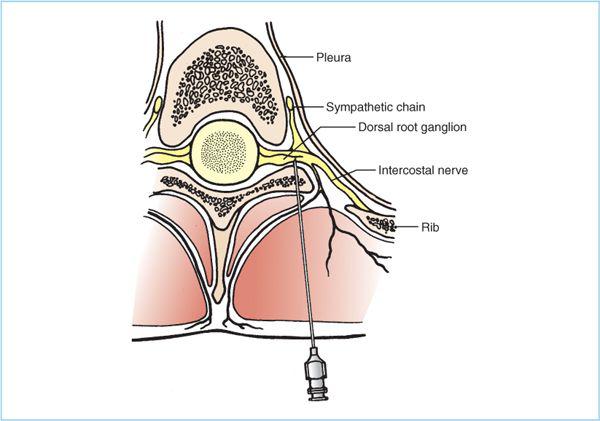
Figure 10.2. Thoracic paravertebral block. The thoracic spinal nerves exit the intervertebral foramen and enter a small triangular space formed by the vertebral body, the pleura, and the plane of the transverse process. The needle is advanced off the superior border of the transverse process and into this triangle. The depth from the transverse process to the nerve is approximately 2 cm. Some medial angulation is important to reduce the chance of entering the pleura and causing a pneumothorax.
C. Specific uses. There are numerous potential uses of paravertebral block, either as a “stand-alone” regional anesthesia technique or in combination with other blocks (e.g., intercostal). Given in the subsequent text are a few common examples.
1. Breast surgery. Thoracic paravertebral block has been shown to be superior to general anesthesia in terms of postoperative pain, nausea/vomiting incidence, and ambulatory discharge time (1).
2. Inguinal hernia. As with breast surgery, paravertebral block has been shown to be superior to general anesthesia (less postoperative pain, nausea/vomiting, and faster discharge) for inguinal hernia repair (2, 3).
3. Postsurgical analgesia: thoracotomy/thoracoscopy. Thoracic paravertebral block provides excellent analgesia for thoracic surgery and has been shown to be superior to thoracic epidural analgesia (lower pain scores, less hypotension, less nausea/vomiting, better pulmonary function). The ability to place a catheter for continuous local anesthetic infusion is an important advantage of paravertebral block over intercostal block (4, 5).
4. Other pain therapy. Both single-injection and continuous techniques can be useful with longer-term pain problems.
a. Rib fracture. Rib fractures are readily treated by paravertebral block (6). The ability to place a catheter for continuous infusion is a significant advantage of paravertebral block over intercostal block and a reduced effect on the sympathetic nervous system is an advantage over thoracic epidural analgesia. Continuous paravertebral block also has potential advantages over epidural block in the setting of concomitant spinal trauma.
b. Herpes zoster (acute outbreak and postherpetic neuralgia). Unlike intercostal block, a catheter can be placed for repetitive or continuous paravertebral block. This approach has been reported to be successful in treating refractory postherpetic neuralgia (7).
IV. Local anesthetics
A. Any local anesthetic and concentration used for peripheral nerve block is appropriate for paravertebral block. Specific examples are given in the subsequent text.
1. Intermediate-duration amide local anesthetics (e.g., lidocaine, mepivacaine) will produce blocks lasting 3 to 5 hours.
2. Long-duration amide local anesthetics (e.g., bupivacaine, levobupivacaine, ropivacaine) will produce blocks lasting 8 to 14 hours.
3. As with other blocks, more dilute solutions (lower doses) produce less motor block and shorter-duration sensory blocks.
B. The local anesthetic volume required per nerve blocked is significantly higher with paravertebral blocks than with intercostal blocks; therefore, fewer dermatomes can be safely blocked than would be the case with intercostal block.
V. Lumbar technique
A. Position. The block can be performed with the patient in any position, although prone (with an abdominal pillow to flex the spine) and sitting are probably easier (especially for bilateral blocks) than lateral.
B. Mark injection sites. Identify the spinous processes associated with the nerves to be blocked and mark them along their entire length. Draw transverse lines through the spinous processes of the vertebrae for the targeted nerves. Three to four centimeters lateral to the spinous processes, draw vertical lines connecting the transverse lines (Figure 10.3). The lines should intersect over the inferior edge of the vertebra’s transverse process.
1. In the lumbar region, the superior border of the spinous process is at the same level as the caudad edge of its own transverse process (Figure 10.1). Also, because the spinal nerve is named for the vertebra forming the cephalad half of the intervertebral foramen, the spinal nerve exits inferior to the transverse process of the vertebra for which it is named.
C. Aseptically prepare and drape the skin and raise local anesthetic skin wheals at each intersection of the transverse and vertical lines.
D. Needle placement
1. Fixed-depth technique. Insert a 6- to 8-cm (2.5–3.5 in.) 22-gauge or larger needle through the skin wheal at a 10- to 30-degree cephalad angle (Figure 10.4).
a. Depending on the girth of the patient, the transverse process should be contacted at a depth of 2.5 to 5 cm (1–2 in.). If the transverse process is not contacted at the expected depth, gently probe cephalad and caudad parallel to the neuraxis.
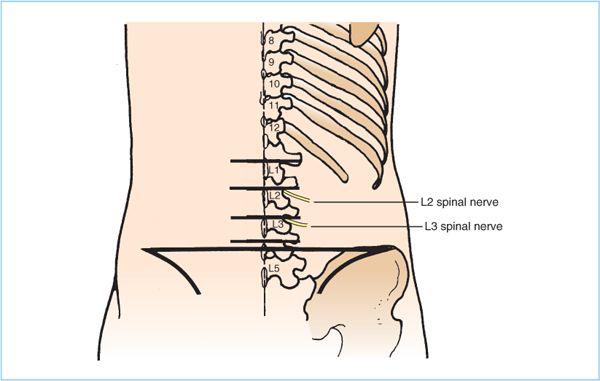
Figure 10.3. Cutaneous landmarks for lumbar paravertebral block. The entire spinous process is outlined, and the horizontal lines pass through the cephalad edge of the process. The intersection of the horizontal and vertical lines should lie above the caudad edge of the transverse process, and the needle should be inserted at this point with a slight (10- to 30-degree) cephalad angle to contact the transverse process.







Full access? Get Clinical Tree


