KEY POINTS
1. Chronic pain due to intercostal nerve injury develops in approximately 50% of postthoracotomy patients, and in 5% this pain becomes severe and disabling.
2. Thoracic epidural analgesia for cardiac surgery is associated with reduced supraventricular arrhythmias and postoperative pulmonary complications relative to standard approaches.
3. Highly lipophilic drugs, such as fentanyl, are best used with catheters placed near the involved dermatomes. Hydrophilic drugs, such as morphine, are most useful for remote catheters such as those positioned in the lumbar region.
4. Epidural opioids should generally not be administered unless postoperative observation and monitoring for delayed respiratory depression are planned.
5. Patients with severe lung disease have the most to gain in terms of improved outcome from optimal postoperative analgesia such as continuous thoracic epidural.
6. The risk of nephrotoxicity appears to be low (1:1,000 to 1:10,000) with perioperative ketorolac administration.
7. Respiratory depression requiring naloxone administration is reported to occur in 0.2% to 1% of patients receiving epidural narcotics.
8. Pending additional contributions to our understanding of the risk of peridural bleeding, the trend in expert opinion has recently shifted to argue for caution, particularly regarding thoracic epidural catheter placement prior to “full” heparinization for cardiac surgery.

1
I. Introduction
A. Incidence and severity of pain after cardiothoracic procedures. Pain is an unpleasant sensation occurring in varying degrees of severity as a consequence of injury or disease. Chest surgery, via sternotomy and especially via thoracotomy, is among the most debilitating for patients due to pain and consequent respiratory dysfunction. Important sources of postoperative discomfort after cardiothoracic surgery, in addition to incisional pain, include indwelling thoracostomy tubes, rib or sternal fractures, and costovertebral joint pain due to sternal retraction. Chronic pain due to intercostal nerve injury develops in approximately 50% of postthoracotomy patients, and in 5% this pain becomes severe and disabling. Despite the early belief that minimally invasive thoracic and cardiac surgical procedures involving smaller incisions would reduce the incidence and severity of postoperative pain compared to traditional cardiac surgery, clinical experience has not borne out this assumption for most patients. No single thoracotomy technique has been shown to reduce the incidence of chronic postthoracotomy pain, and patients should be warned in advance of this potential postoperative complication.
B. Transmission pathways for nociception. An understanding of the anatomy and physiology of pain pathways underpins the logical choice of analgesic strategies during and after cardiothoracic surgery. Multimodal approaches take advantage of numerous therapeutic targets in the signaling chain to optimize pain control while minimizing side effects [1].
In the thoracic region, pain signals are relayed through myelinated Aδ and unmyelinated C fibers in peripheral intercostal nerves. The ventral, posterior, and visceral branches of each intercostal nerve innervate the anterior chest wall, posterior chest wall, and visceral aspects of the chest, respectively. These branches join together just before entering the paravertebral space and then pass through the intervertebral foramina in the spinal canal. Sensory intercostal nerve fibers form a dorsal root that fuses with the spinal cord dorsal horn to enter the central nervous system (CNS). Somatic pain is mediated predominantly through myelinated Aδ fibers in the ventral and posterior branches. Sympathetic (visceral) pain is mediated by unmyelinated C fibers in all three branches. Sympathetic afferent pain signals are directed from intercostal nerve branches through the sympathetic trunk (a paravertebral structure found just beneath the parietal pleura in the thorax) and then pass back into the peripheral nerves to enter the CNS from T-1 to L-2. In addition, the vagus nerve provides parasympathetic visceral innervation of the thorax. This cranial nerve enters the CNS through the medulla oblongata and, therefore, is not normally affected by epidural or intrathecal (IT) methods of pain control.
The spinal cord and spinal canal are considerably different in length, and consequently spinal cord dermatomal segments do not typically lie at the level of their respective vertebrae. Thus, knowledge of spinal anatomy is essential if regional analgesia techniques are to be successful. This is particularly true with the use of lipid-soluble epidural opioids because the targeted dorsal horn often is significantly cephalad relative to the associated intervertebral foramen and nerve.
Most spinal pain signals are transmitted to the brain after crossing from the dorsal horn to contralateral spinal cord structures (e.g., spinothalamic tract). Distribution of nociceptive messages occurs to numerous locations in the brain resulting in cognitive, affective, and autonomic responses to noxious stimuli.
Endogenous modification of pain signals begins at the site of tissue trauma and includes hyperalgesia related to inflammation and other CNS-mediated phenomena such as “windup.” The substantia gelatinosa of the dorsal horn is an important location for pain signal modulation, including effects that are mediated through opioid, adrenergic, and N-methyl-D-aspartate (NMDA) receptor systems.
C. Analgesia considerations: The procedure, patient, and process. The degree and location of surgical trauma, particularly in relation to the site of skin incision and route of bony access to the chest, are particularly important in anticipating analgesic requirements after cardiothoracic surgery. Notably, minimally invasive procedures that reduce total surgical tissue disruption but relocate it to more pain-sensitive regions may not translate into reduced postoperative pain (e.g., minithoracotomy vs. sternotomy). Analgesic strategies are best individualized, particularly for high-risk patients in whom outcome benefits may be the greatest. This includes not only appropriate postoperative analgesia delivery but also preoperative education regarding pain reporting, procedures, and devices to provide analgesia, and expectations for postoperative transition to oral medications and home administration.
D. Adverse consequences of pain. In addition to unpleasant emotional aspects of pain, nociceptive signals have several other effects that can be harmful and delay patient recovery. These include activation of neuroendocrine reflexes constituting the surgical stress response (including inflammation and elevated circulating catecholamines), a catabolic state associated with high levels of several other humoral substances (e.g., cortisol, vasopressin, renin, angiotensin), decreased vagal tone, and increased oxygen consumption. Spinal reflex responses to pain include localized muscle spasm and activation of the sympathetic nervous system.
Pathophysiologic consequences of the neuroendocrine local and systemic responses to pain include respiratory complications related to diaphragmatic dysfunction, myocardial ischemia, ileus, urinary retention and oliguria, thromboembolism, and immune impairment [2].
2
E. Outcome benefits of good analgesia for cardiothoracic procedures. A primary benefit of effective pain control is patient satisfaction. Studies have documented additional advantages of optimizing analgesia, especially in recovery from thoracotomy. Belief that the pain of median sternotomy is less severe and inconsequential to outcome leads many institutions to employ conventional analgesia protocols involving fixed dosing of analgesics on a timed schedule. However, after coronary bypass grafting, attention to profound analgesia in the early postoperative period may decrease the incidence and severity of myocardial ischemia. A meta-analysis of 28 randomized studies suggests that thoracic epidural analgesia for cardiac surgery is associated with reduced supraventricular arrhythmias and postoperative pulmonary complications relative to standard approaches [3].
Evidence supporting reductions in perioperative complications related to pain relief are reported for many different analgesia techniques and may be related to their effectiveness in blocking the surgical stress response and nociceptive spinal reflexes. In this regard, neuraxial and regional analgesia are most often reported as being effective. Nonetheless, beyond reduced pain, any outcome benefits related to the incidence of major morbidities and mortality of specific analgesia techniques remain difficult to prove, possibly due to the insufficient numbers of patients studied and the low frequency of these events, as is well summarized in a review by Liu et al. [4]. In general, reported benefits of good analgesia rely on reporting of surrogate markers that correlate with major adverse outcomes (e.g., arterial oxygen saturation) that imply attenuation of the adverse consequences of pain outlined in Section I.D. For example, in the setting of thoracic surgery, thoracic epidural analgesia provides superior pain relief compared to systemic opioids and decreases the incidence of atelectasis, pulmonary infections, hypoxemia, and other pulmonary complications [5]. In addition, effective analgesia established before surgery in some circumstances may provide pre-emptive protection against the development of chronic pain syndromes. Aggressive pain control in the early postoperative period was associated with a greater than 50% reduction in the number of patients continuing to experience chronic pain 1 year after thoracotomy in one study [6]. Unfortunately, in cardiac surgery, reports of neuraxial techniques generally involve small numbers and fail to demonstrate clinical outcome benefit, although benefits in hospital length of stay and cost avoidance have been commonly shown [7]. Outcome benefit following cardiac surgery with central neuraxial analgesia was not demonstrated in a meta-analysis published in 2004 nor in a randomized trial published in 2011 [8,9].
II. Pain management pharmacology
A. Opioid analgesics
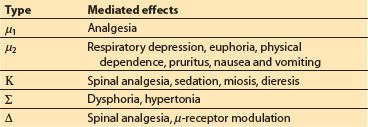
1. Mechanisms. Opioid analgesics are a broad group of compounds that include naturally occurring extracts of opium (e.g., morphine, codeine), synthetic substances (e.g., fentanyl, hydromorphone), and endogenous peptides (e.g., endorphins, enkephalins). The analgesic effects of these drugs are all linked to their interaction with opioid receptors; however, individual agents may function as agonists, antagonists, or partial agonists at different receptor subtype populations. Opioid receptors are widely distributed throughout the body, but they are particularly concentrated within the substantia gelatinosa of the dorsal horn of the spinal cord, as well as regions of the brain including the rostral ventral medulla, locus ceruleus, and midbrain periaqueductal gray area. Stimulation of opioid receptors inhibits the enzyme adenyl cyclase, closes voltage-dependent calcium channels, and opens calcium-dependent inwardly rectifying potassium channels, resulting in inhibitory effects characterized by neuronal hyperpolarization and decreased excitability. Opioid receptor subtypes have been sequenced and cloned, and they belong to the growing list of G-protein-coupled receptors. The effects of agonist binding at different opioid receptor subtypes are summarized in Table 27.1.
Table 27.1 Opioid receptors
3
2. Perioperative use. Opioids are commonly administered throughout the perioperative period for cardiothoracic procedures. Preoperatively, they can be given orally, intramuscularly (IM), or intravenously (IV) alone or as part of a sedative cocktail to provide anxiolysis and analgesia for transport and placement of intravascular catheters. Intraoperatively, they are given IV most commonly as part of a balanced anesthetic technique that includes potent inhaled anesthetics, benzodiazepines, and other agents. Finally, they can be injected directly into the thecal sac or included as a component of epidural infusions to provide intraoperative and postoperative analgesia. Opioids administered epidurally have varying spread and analgesic potency based in part on their water solubility and are best matched with analgesic requirements with knowledge of the position of the epidural catheter relative to the dermatomes affected by pain and the relative lipophilicity of the drug. Highly lipophilic drugs, such as fentanyl, are best used with catheters placed near the involved dermatomes. Hydrophilic drugs, such as morphine, are most useful for remote catheters such as those positioned in the lumbar region. Drugs with intermediate lipophilicity, such as hydromorphone, are considered ideal by most and can be used for more balanced spread.
3. Side effects and cautions
a. Respiratory depression (increased risk with higher dosing, coadministration of other sedatives, opioid-naive patients, advanced age, central neuraxial administration of hydrophilic opioid agents)
b. Sedation
c. Pruritus
d. Nausea
e. Urinary retention, especially common in the elderly and in males receiving spinal opioids
f. Inhibition of intestinal peristalsis/constipation
g. CNS excitation/hypertonia, much more notable with rapid IV administration of lipophilic agents
h. Miosis
i. Biliary spasm
All of the above effects can be reversed with administration of opioid antagonist drugs (e.g., naloxone). Opioid rotation, or changing the narcotic drug that a patient is receiving, may also be useful in reducing the incidence or severity of complicating side effects or also in enhancing the patient’s experience of analgesia [10].
B. Nonsteroidal anti-inflammatory drugs
1. Mechanisms. Nonsteroidal anti-inflammatory drugs (NSAIDs) act principally through both central and peripheral inhibition of cyclo-oxygenase, resulting in decreased synthesis of prostaglandins from arachadonic acid, including prostacyclin and thromboxane. Prostaglandins are involved in the physiology of numerous signaling pathways, including those influencing renal perfusion, bronchial smooth muscle tone, hemostasis, the gastric mucosal secretions, and the inflammatory response. Prostaglandin E2 is the eicosanoid produced in greatest quantity at sites of trauma and inflammation and is an important mediator of pain. The full therapeutic effects of NSAIDs are complex and likely involve mechanisms that are independent of prostaglandin effects. For example, prostaglandin synthesis is effectively inhibited with low doses of most NSAIDs; however, much higher doses are required to produce anti-inflammatory effects.
2. Perioperative use. NSAIDs are useful for postoperative analgesia. They are most commonly administered in cardiothoracic surgical patients as a complement to neuraxial techniques. Their principal advantage is the absence of respiratory depression and other opioid side effects. Many NSAIDs are available for oral or rectal administration. Ketorolac is a non-selective NSAID intended for short-term use (5 days or less) with preparations available for intravenous or intramuscular injection, in addition to tablets for ingestion.
3. Side effects and cautions
a. Decreased renal blood flow/parenchymal ischemia
b. Gastrointestinal mucosal irritation
c. Impaired primary hemostasis
4. COX-2 inhibitors
The effects of cyclo-oxygenase are mediated by two distinct isoenzymes termed COX-1 and COX-2. COX-1 is the constitutive form responsible for production of prostaglandins involved in homeostatic processes of the kidney, gut, endothelium, and platelets. COX-2 is predominantly an inducible isoform responsible for production of prostaglandins during inflammation. Highly selective COX-2 inhibitors have potent analgesic properties and, until recently, were used frequently to treat perioperative pain. Unfortunately, combined data from several large randomized double-blind trials [11] revealed an increased incidence of cardiovascular complications including myocardial infarction with agents in this drug class. Celecoxib is the only remaining COX-2 inhibitor widely available for prescription in the US. The difference between celecoxib and the other agents may be due to its relatively modest COX-2 versus COX-1 subtype selectivity compared to the other agents (30 : 1 vs. >300 : 1). However, celecoxib use remains largely limited to treatment of severe arthritis, rheumatoid arthritis, and ankylosis spondylitis in circumstances where treatment of these conditions with several other NSAIDs has failed. Prothrombotic effects from COX-2 inhibition are likely due to reduced prostacyclin generation. In addition, COX-2 inhibitors lack the antiplatelet effects of aspirin and even favor vasoconstrictive effects. Thus, use of these agents for perioperative pain relief is not recommended.
C. Acetaminophen (paracetamol)
1. Mechanism
Acetaminophen is a synthetic, non-opiate, analgesic drug that is distinct from most other NSAIDs in that it is a weak inhibitor of the synthesis of prostaglandins and of COX-1 and COX-2. Its mechanisms appear to be primarily central, resulting in analgesia and antipyresis, with only minimal anti-inflammation. COX-3, a splice variant of COX-1, has been suggested to be the site of action. Other proposed actions include activation of descending serotonergic pathways and/or inhibition of the nitric oxide pathway mediated by a variety of neurotransmitter receptors including NMDA and substance P. Although the exact site and mechanism of analgesic action is not clearly defined, acetaminophen appears to produce analgesia by elevation of the pain threshold.
2. Perioperative use and cautions
Until recently, acetaminophen was only available for oral and rectal administration and thus infrequently used in the immediate perioperative period. In 2010, the FDA approved an intravenous form of the drug for relieving pain or fever in surgical patients, approved for use in adults and children aged 2 and older. It has been shown useful in the treatment of moderate to severe post-surgical pain, demonstrating an opioid-sparing effect with good patient acceptance and few adverse effects, especially in orthopedic surgical populations [12]. A modest opioid-sparing effect, with no reduction in the incidence of nausea and vomiting, was shown when intravenous acetaminophen was compared to oral acetaminophen in a postoperative population of coronary artery bypass surgical patients [13].
The primary risk of acetominaphen is hepatotoxicity secondary to overdose. Acetaminophen toxicity is the leading cause of acute liver failure in the United States. A typical intravenous adult dosing schedule involves administration of 650 to 1,000 mg every 6 hrs, with infusion of the drug timed to occur over at least 15 min.
D. Local anesthetics
1. Mechanisms. Local anesthetics interrupt neural conduction thus disrupting transmission of pain and other nerve impulses through blockade of neuronal voltage-gated sodium channels. This blockade does not change the resting potential of the nerve. However, altered sodium ion channel permeability slows depolarization such that, in the presence of a sufficient concentration of local anesthetic, threshold for propagation of an action potential cannot be reached.
2. Perioperative use. Local anesthetics are used throughout the perioperative period for topical, infiltration, peripheral nerve, or central neuraxial anesthesia. Their advantage lies in the capacity to provide profound analgesia without the undesired side effects seen with opioids or NSAIDs. Effective regional anesthesia is the best technique to most completely attenuate the neurohumoral stress response to pain. Thoracic epidural analgesia is particularly useful in treating pain, both somatic and visceral, for patients with occlusive coronary artery disease.
3. Side effects and cautions
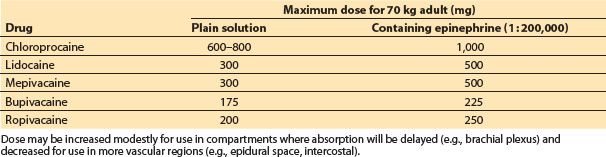
a. Not surprisingly, side effects from sodium channel blockade due to local anesthetic toxicity resemble those observed with severe hyponatremia. Excessive local anesthetic blood concentrations, reached through absorption or inadvertent intravascular injection, predictably result in toxic effects on the CNS (seizures, coma) and the heart (negative inotropy, conduction disturbances, arrhythmias). Table 27.2 lists commonly accepted maximum local anesthetic dosing for infiltration anesthesia.
Table 27.2 Maximum recommended dosing of local anesthetic agents for local infiltration







Full access? Get Clinical Tree


