Pain Management and Sedation
Rahim Valani MD, CCFP-EM, FRCPC, PG Dip Med Ed
ANATOMY OF PAIN1
Pain is a neuro-biochemical phenomenon.
Nociceptors from the periphery transduce stimuli into neural impulses that are propagated to cell bodies and up the spinal cord.
Neuron cell bodies are in the spinal cord’s dorsal root ganglion (DRG).
Each spinal cord level has its own DRG, while the face has the trigeminal ganglion.
Two main types of receptors, the slow C-fibers and the fast Aδ fibers (Table 18-1).
Impulse-inducing chemicals include leukotrienes, bradykinin, serotonin, histamine, potassium, protons, acetylcholine, substance P, and platelet-activating factor.
The spinothalamic pathway is the main tract for pain transmission.
Spinothalamic pathway is divided into:
Lateral fast signals.
Travel to the brainstem’s thalamus and reticular area.
Help discriminate location, intensity, and duration of pain.
Medial slow/chronic pain.
Terminates in the spinal cord’s lamina II and III.
A multisynaptic pathway with a large terminal distribution area.
The thalamus is the key area for initial pain interpretation.
Pain is divided into somatic pain or visceral pain.
Visceral pain can be activated by:
Ischemia.
Chemical stimulation.
Spasm of hollow viscus.
Overdistention of hollow viscus.
CLINICAL CONSIDERATIONS IN PAIN MANAGEMENT
Thorough assessment of medical condition is necessary for pain management.
Pain affects a child’s psychological, behavioral, physiologic, and emotional state.
Goal: To optimally and safely manage a patient’s pain.
Pediatric differences compared to adults include:
Cognitive abilities.
Developmental status.
Respiratory mechanics and airway anatomy.
Metabolism of drugs.
Pain assessment should be:9
Individualized.
Comprehensive.
Measured.
Continuous.
Monitored.
Documented.
Most reliable pain indicator is patient self-reporting.
There are many different pain scales in use (Fig. 18-1).
The American Academy of Pediatrics (AAP) and American Pain Society recommend observing behavior to complement self-reporting.
This is an acceptable alternative when valid self-reporting is unavailable.11
TABLE 18-1 Comparison of Different Neural Pain Fibers | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
MODES OF PAIN RELIEF
Nonpharmacologic
Cognitive: Music, imagery, positive reinforcement, hypnosis.
Behavioral: Relaxation, biofeedback, breathing.
Physical: Heat/cold application, massage, touch, TENS, acupuncture, immobilization.
Have naloxone available in case of respiratory depression with opioids.
Dose: 0.1 mg/kg (maximum dose is 2 mg).
Narcotic clearance is slower in neonates, and increases over the first 2 to 6 months.
Dose accordingly.
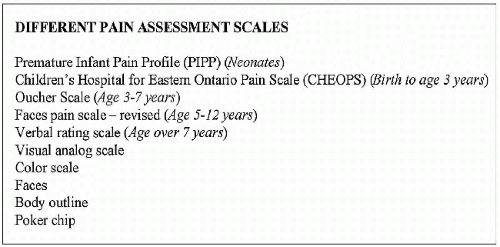
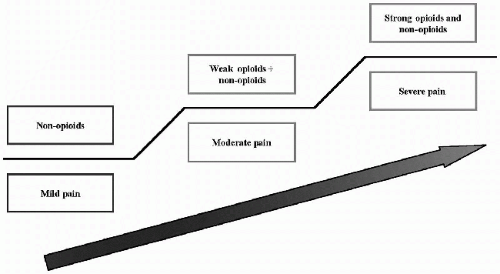 FIGURE 18-2 • Pain relief ladder. (From Kowalczyk A, ed. The 2004-2005 formulary of drugs. The Hospital for Sick Children, University of Toronto, 2004, with permission.) |
|
|









