Fig. 29.1
Initial view of a right adnexa demonstrating torsion
In preparation for surgical exploration patients should receive broad spectrum systemic antibiotics. Patients should be positioned in the dorsal lithotomy position. A foley catheter should be inserted prior to incision. It is important to have a uterine manipulator available.
Operative Strategy
One should visualize and explore the pelvis and adnexal structures bilaterally. Additionally, other potential causes of abdominal pain should be evaluated including appendicitis, diverticulitis, and Meckel’s diverticulum. Once the diagnosis is confirmed, use atraumatic graspers to detorse the ovary in question to assess for viability with an emphasis on adnexal preservation, especially nulliparous females. Both oophoropexy and shortening of the infundibular ligament have been proposed as strategies to prevent recurrence.
Operative Technique
The authors advocate a laparoscopic approach, though open laparotomy may be performed based on the skill of the operator. Patient is positioned in dorsal lithotomy and uterine manipulator is placed.
Incisions
A vertically oriented infra-umbilical 11 mm incision is created and the abdomen is entered using an open technique. In the case of a pregnant patient, a supraumbilical incision may be preferable based on the size and position of the gravid uterus. The vertical orientation allows for extension to accommodate removal of a large adnexa if necessary due to edema and necrosis or underlying mass. Pneumoperitoneum to 14 mmHg is obtained, and additional 5 mm trocars are placed in the right and left lower quadrants under direct visualization.
Exposure
The patient is positioned in trendelenburg and the uterus is elevated out of the pelvis using the manipulator. Any remaining bowel in the pelvis is maneuvered out of the pelvis taking care not to induce serosal injury. The appendix, sigmoid colon, and terminal ileum are all examined. Both adnexa are inspected and the torsion is untwisted by manipulating the adnexa with atraumatic graspers in a hand over hand technique (Fig. 29.2). Showering of clot located within the ovarian vein was once felt to pose such risk as the preclude ovarian salvage, however, as experience with ovarian salvage has gained momentum, the risk of this posing clinical significance is much lower than originally thought. Once the torsion has been released, allowing blood flow to restore, monitor the ovary for viability. If the ovary is salvageable, preparation should be made for oophoropexy. If it is obviously necrotic, make preparations for oophorectomy.
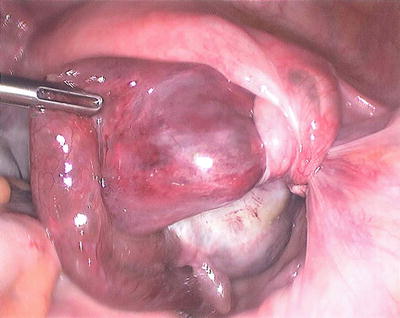
Fig. 29.2
Atraumatic graspers are used to detorse the ovary
Evaluation for Underlying Ovarian Pathology
Once the viability of the ovary has been determined as salvageable, the ovary should be carefully inspected for an underlying etiology predisposing to the torsion. Possible contributing factors include dermoid cysts, simple cysts, corpus luteum cysts in the case of pregnancy, and ovarian neoplasm. Management of these associated conditions should be based on clinical suspicion for malignancy as avoidance of spillage of malignant cells into the pelvis is of utmost importance. For benign conditions, preservation of as much functional ovarian tissue as possible should be employed. Cysts or teratomas can often be excised utilizing either ultrasonic or bipolar energy device. If a corpus luteum cannot be preserved prior to 10 weeks gestation, initiation of progesterone replacement should be performed. Any removed structures should be placed into an endoscopic retrieval bag to prevent spillage of contents during removal.
Related posts:





Full access? Get Clinical Tree


