Fig. 59.1
Pre- and postoperative hip replacement
TJA of the knee requires replacing the injured bone and cartilage with a plastic or metal implant to optimize alignment and restore function. Common complications include infection, knee stiffness and loss of range of motion, blood clots, nerve injury, and implant wear. See Fig. 59.2.
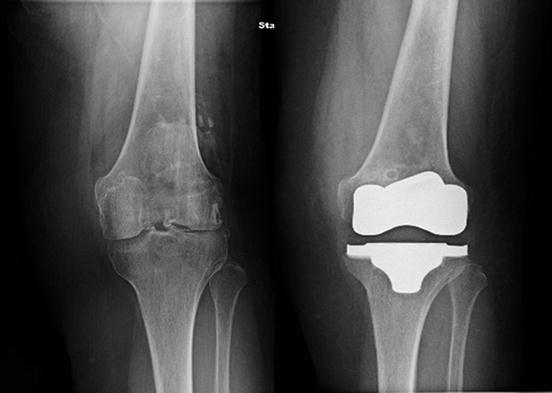
Fig. 59.2
Pre- and postoperative knee replacement
Improvements in technology and clinical management have allowed for effective and safe joint arthroplasty in the aging population. As such, there are no strict age restrictions for TJA . Patients should be evaluated individually, with emphasis on the natural history of experienced pain, its associated limitations on everyday activities, the patient’s responsiveness to medical treatment, and existing comorbidities.
Foot and Ankle Surgery
Foot and ankle pain commonly occurs in patients with osteoarthritis , rheumatoid arthritis , or poorly healed fractures. Selective fusion and TJA of the ankle, foot, and toes provides pain relief for the majority of patients [8–10].
Fusion involves the removal of articular cartilage between adjacent bones and implantation of metal instrumentation to hold bones in the most functional position while the bones heal together (arthrodesis). Bone grafts may also be used to aid in fusion. Fusion of the ankle, foot, or toe joints is indicated depending on the location of pain and joint degeneration. Complications include delayed or poor bone fusion, wound healing issues, infection, hardware irritation, and stiffness in adjacent joints.
In TJA of the ankle, an artificial ankle consisting of metal and plastic components is implanted to replace the diseased joint . Unlike ankle fusion, joint mobility is maintained and often improved by TJA. Complications include infection, neurovascular damage, blood clots, misalignment, and implant wear.
Fusion and TJA of the ankle should be avoided in patients with bone or vascular illness that may interfere with bone healing, severe deformity of the extremity, markedly impaired leg function, or prior/current bone infection.
Hand Surgery
Carpal tunnel syndrome , osteoarthritis , and rheumatoid arthritis are the main causes of debilitating pain in the hand and wrist. Carpal tunnel release surgery, TJA , and fusion of bones in the hand and wrist are commonly used and effective procedures [11–13].
Carpal tunnel release involves incising the transverse carpal ligament, which is located on the ventral surface to the wrist. This creates a larger carpal tunnel and decreases pressure on the median nerve thus decreasing pain and optimizing nerve function. Complications include bleeding, median nerve damage, and infection.
Fusion of wrist and hand bones requires the removal of articular cartilage on surfaces of adjacent bones followed by the insertion of metal pins/plate and screws into the bones , which stabilizes the joint as the bones fuse. Selecting which bones to fuse is dependent on the location of pain and joint pathology. Complications include skin necrosis, irritation related to retained instrumentation, incomplete fusion, and loss of mobility and dexterity.
TJA of the wrist involves replacing damaged bone and cartilage with a wrist prosthesis, consisting of radial and carpal components. The radial component of the prosthesis is implanted in the distal radius , while the carpal component is inserted into viable carpal bones. These two components are linked by a plastic spacer , which approximates the wrist’s natural motion. Prosthetic wear and loosening are common complications, especially in patients with severe wrist deformity or poor bone stock. Infection and wound healing problems are also possible complications, which are more common in patients with rheumatoid arthritis .
Surgical treatments for hand and wrist pain are generally less invasive compared to major joint or spine operations. As such, most can be performed in under local anesthesia and in the outpatient setting.
Shoulder and Elbow Surgery
Shoulder and elbow pain are commonly associated with arthritis , fractures, and tendon inflammation or tears [14–16]. TJA of the shoulder is considered for shoulder fractures and arthritis . Rotator cuff repair is reserved for tendon injuries
TJA of the shoulder includes substituting the damaged humeral head and glenoid fossa with a polished metal ball and a plastic socket, respectively. This procedure may not be suitable for individuals with torn rotator cuff tendons. Hemiarthroplasty and reverse total shoulder arthroplasty are also viable joint replacement options. Complications include infection, nerve injury, and implant dislocation or wear. See Fig. 59.3.
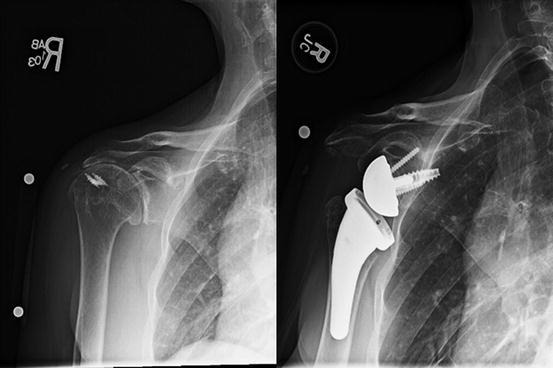
Fig. 59.3
Pre- and postoperative shoulder replacement
Rotator cuff repair most commonly involves reconnecting a tendon to the humeral head. A complete tear within the tendon requires suturing of two ends back together. Partial tears may only involve trimming loose, aggravating tendon pieces. Complications include infection, nerve damage, stiffness, failed deltoid reattachment, and tendon retear.
Open, mini-open, or arthroscopic surgical approaches are suitable for rotator cuff repair and produce comparable outcomes. Arthroscopic procedures have grown tremendously in popularity over the last decade and now account for the vast majority of rotator cuff repair procedures. Patient noncompliance with rehabilitation and postoperative restrictions, old age, and large tendon tears are all linked with suboptimal surgical outcomes.
Spine Surge+ry
Back and radicular arm and leg pain may occur due to disc pathology (degeneration, herniation), spondylolisthesis (vertebral displacement), spinal stenosis (canal narrowing), or deformity (scoliosis, kyphosis). See Fig. 59.4. Discectomy, laminectomy, fusion, and spinal deformity correction are commonly performed procedures for back and radicular pain [17–19].
Discectomy normally involves surgical removal of the protruding portion of the herniated vertebral disc that is impinging on nerve roots and eliciting pain in the patient. In the cervical spine, the disc is often completely removed from an anterior approach, thus necessitating reconstruction with either fusion or arthroplasty . In the lumbar spine, the offending fragment of disc is most commonly removed from a posterior approach. Open or minimally invasive approaches may be taken and fusion is not generally required. Complications include infection, neurovascular injury, continued pain, and leakage of cerebrospinal fluid (CSF) .Related posts:
 Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
Pain in the Stroke Rehabilitation Patient
Pain in the Neuromuscular Disease Rehabilitation Patient
Basic Psychopharmacology for the Treatment of Pain in the Rehabilitation Patient
Intrathecal Therapy for the Treatment of Pain in the Rehabilitation Patient
 Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
Intra-articular Joint and Bursa Injections for the Treatment of Pain in the Rehabilitation Patient
 Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient
Chiropractic Medicine for the Treatment of Pain in the Rehabilitation Patient

Full access? Get Clinical Tree


