Immediate Management of Life-Threatening Injuries
Patients with orthopedic injuries and musculoskeletal disorders constitute a large portion of patients presenting to the Emergency Department. All trauma patients should be managed initially in the same manner, with similar guiding principles of trauma care regardless of their underlying injuries. Orthopedic injuries may be dramatic, but they should not draw attention away from more critical elements of initial patient assessment and treatment. The emergency physician must assess the patient and manage injuries and based on the immediate threat to survival, evaluating each trauma patient with the primary survey, which consists of assessing the airway, breathing, circulation, disability, and exposure (ABCDEs) (Table 28–1).
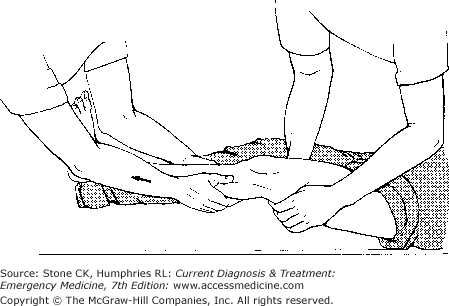
Once the primary survey has been addressed, proceed to the secondary survey, which should be a thorough, but rapid physical examination from head to toe to assess for all injuries. With cervical spine precautions in place, logroll the patient, assess the posterior scalp, and examine the entire spine for tenderness or step-off deformities. Perform a digital rectal examination to evaluate for sphincter tone, gross blood, or abnormal prostate position. When evaluating the pelvis for stability, apply gentle anteroposterior and lateral compression. Visualize and go through range of motion of all joints and document all lacerations, abrasions, and contusions. Physical examination of orthopedic injuries includes inspection for deformity, color change, palpation for tenderness, range of motion, and assessment of neurovascular status. At this time, consider reduction of certain orthopedic emergencies such as a dislocated hip, knee, or any fracture or dislocation in which vascular compromise is present (Figure 28–1). Delayed reduction may lead to avascular necrosis, or other complications; therefore, if possible, reduce fractures and dislocations with neurovascular compromise before transferring the patient.
- Sharp, guillotine injuries are best candidates for reimplantation
- Keep amputated part clean, moisten with saline, and put on ice
- Do not allow part to freeze
- Cooling will help increase viability of amputated part up to 12–24 hours
Patients incurring traumatic amputations should be considered for reimplantation surgery. Young healthy patients with sharp, guillotine injuries without crushing or avulsion damage are the best candidates for successful reimplantation. However, it is best to consider all patients as potential candidates, care for the amputated part, and make appropriate consultations or arrange for transfer.
The patient presents with an amputated digit or limb.
Although this diagnosis is made clinically, X-rays often help delineate exactly where the injury occurred, or if underlying fractures or dislocations exist.
The amputated part should be kept clean, wrapped in a sterile dressing, moistened with sterile saline, placed in a plastic bag, and put on ice. Do not use dry ice or allow the amputated part to freeze. Cooling the amputated part will increase the viability from 6–8 hours to approximately 12–24 hours. The injury should be treated as an open fracture, with appropriate use of antibiotics and tetanus prophylaxis.
Patients with limb amputations usually require consultation with an orthopedic, plastic, or trauma surgeon. These patients should be admitted for further surgical management, neurologic and vascular evaluation, and monitoring of blood loss. Patients with small digit amputations may be managed in the emergency department and discharged with appropriate close follow-up.
A potentially devastating and subtle complication of orthopedic injuries is the development of a compartment syndrome. Although predominantly occurring in the lower extremities, a compartment syndrome can potentially occur anywhere in the body with a restricting compartment. Compartment syndromes are caused by compromised blood flow due to increased hydrostatic pressure in a closed tissue space. The lower leg has four compartments: anterior, lateral, posterior, and deep posterior. Trauma below the knee can lead to progressive swelling with eventual decreased blood flow from vascular compression as well as neurologic compromise. The immediate threat is to the viability of the tissue and nerves, but late findings can include permanent posttraumatic muscle contracture, infection, rhabdomyolysis, and renal failure.
The classical findings associated with compartment syndrome are pallor, pulselessness, pain, paresthesias, and poikilothermia. Pain on passive stretching of the muscle groups and the subjective complaint of pain out of proportion to the physical findings are important findings. Decreased or absent pulses are a late and ominous sign, and the presence of a pulse does not exclude compartment syndrome. Delays in recognition of compartment syndrome are more likely to occur in sedated patients or in those with head injuries than in other patients due to altered mental status. The diagnosis can be confirmed by measuring intracompartmental pressures with a Stryker pressure monitor or with a needle connected to an arterial line pressure monitor, although noninvasive methods such as ultrasound are being studied. Levels above 30 mm Hg are abnormal and lead to necrosis of nerve and muscle.
Initial interventions include immobilization and removal of any constricting bandages or splints, as well as being conscious of possible rhabdomyolysis and renal failure. Intracompartmental pressures greater than 30 mm Hg generally require immediate intervention with fasciotomy, preferably by a surgeon.
Patients with compartment syndrome require hospitalization for definitive surgical management.
General Orthopedic Principles
Precise language exists to describe fractures, allowing relevant information to be communicated. The terms closed or open designate whether the skin and soft tissue overlying the fracture site are intact. The exact anatomic location should be included in the description including the name of the bone, side of the body, and standard reference points. Degrees of displacement and angulation should be described in terms of the distal structure’s relationship to the more proximal part of the body. Additional modifiers include descriptions such as comminuted (fracture in more than two fragments), impacted (collapse of one fragment of bone onto another), transverse (fracture line at right angle to long axis of the bone), oblique (fracture line with angle other than right angle), and spiral (fracture line encircles the shaft of a long bone secondary to rotational forces). The term valgus refers to a deformity in which the described part is angled away from the body, whereas varus denotes angling toward the midline. An avulsion fracture occurs when a ligament or tendon pulls a fragment of bone away. Pathologic fractures occur in weakened areas of bone as seen with osteomalacia, cysts, carcinomas, and Paget disease. The possibility of a pathologic fracture should be considered when fractures occur with minimal trauma. Stress fractures occur most commonly in the lower extremity and are seen with repetitive trauma (eg, from prolonged marching or running). Stress fractures may be subtle, may be missed on initial radiographs, and may require a bone scan or other imaging modality to make the diagnosis.
Dislocations are complete disruptions in the normal relationship of the articular surfaces of the bones making up a joint. They may be associated with fractures. Dislocations should be described by the relationship of the distal bone to the more proximal bone. A subluxation is an incomplete dislocation.
Pediatric fractures are distinguished from adult fractures due to difference in the bones of children, which are generally less dense and have increased compliance. A Greenstick fracture refers to an angulated fracture in which the cortex and periosteum are only disrupted on one side of the bone. Torus fractures (also called cortical or buckle fractures) involve a buckling of the cortex. Physeal, or growth plate injuries in children are described by the Salter–Harris classification (Figure 28–2).
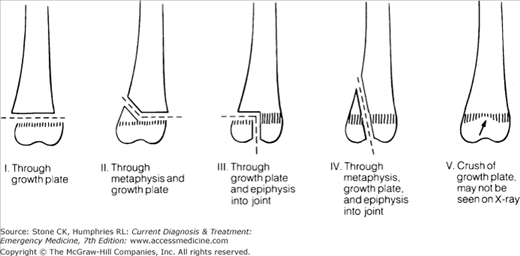
The epiphysis is separated from the metaphysis without radiographic evidence of metaphyseal or epiphyseal fracture. If significant displacement is not present, type I injuries may be difficult to diagnose on initial radiographs and should be suspected if there is point tenderness over an epiphysis. Thickening of the growth plate and soft tissue swelling may be the only signs evident on X-rays. If an injury is suspected but cannot be identified on the initial films, immobilization and orthopedic follow-up are recommended.
Type II injuries are the most common physeal injuries and most often seen in older children over 10 years. The fracture line travels through the physis and is associated with an oblique fracture of the metaphysis on the opposite side from where the force was applied. The metaphyseal fragment is referred to as the Thurston–Holland sign. Growth disturbances usually do not occur with types I and II injuries.
Type III injuries comprise a vertical fracture of the epiphysis perpendicular to the physis, extending into the growth plate. This type of injury is uncommon and most frequently occurs at the distal tibial epiphysis. To avoid the potential of growth plate arrest, the fracture must be appropriately reduced to maintain proper blood supply. Reduction is accomplished most commonly with operative fixation. If surgery is not performed, frequent rechecks and follow-up radiographs are recommended to ensure that the fracture does not become displaced after immobilization.
Unlike types I–III, type IV injuries are the result of compressive rather than rotational or shearing forces. Vertical splitting of the epiphysis occurs, extending through the physis and metaphysis and most commonly involves the distal humerus. Type IV injuries require surgical repair, and growth plate arrest may occur even with operative fixation.
Type V injuries, which are rare, are the result of crushing forces applied to the epiphysis at the area of the physis. When seen, they occur most often at the distal tibia and the knee. Because no fracture is visible, these injuries are frequently missed on initial radiographs and are often diagnosed on follow-up visits after the shortening, and angular deformity secondary to growth plate arrest is evident. Nontraumatic causes include osteomyelitis and epiphyseal aseptic necrosis. Treatment consists of immobilization and close orthopedic follow-up.
Even though emergency physicians are likely to be comfortable using the many eponyms that exist to describe fractures, such as Colles, Monteggia, Galeazzi, it is probably more efficient to provide orthopedic consultants with an anatomic description using the above terminology.
Sprains are injuries to ligaments and may be associated with a fracture. The following grading system is used to describe the severity of the injury:
- Grade I—Incomplete tear. Swelling and ecchymosis may be present. Immobilization and conservative care are indicated.
- Grade II—Significant incomplete tear. Swelling and ecchymosis are usually present as is some laxity in the joint. Immobilization and orthopedic follow-up are indicated.
- Grade III—Complete disruption. The joint is unstable. Orthopedic consultation is indicated for possible surgical repair.
When assessing joint instability, remember that joint effusions, guarding, and muscle contractions may complicate the initial clinical examination. If there is any question, a period of immobilization and follow-up examination are indicated. A strain is an injury to the muscle-musculotendinous unit. Strains are also graded according to severity. Most only require immobilization and conservative management; however, surgical repair may be necessary, and orthopedic consultation or referral should be obtained if indicated.
Splints are a basic part of orthopedic care and should be applied to suspected or confirmed fractures to attempt to avoid and further damage to muscle, nerves, vessels, and skin. They are used to stabilize the injury, provide some amount of pain relief, and help prevent further injury. Some splints are designed to be temporary, such as those applied in the field by emergency medical services personnel. These splints should ideally stabilize the joint above and below the suspected injury. Attempting to correct deformities before obtaining radiographs is not recommended, unless vascular compromise is suspected.
Splints are often applied in the emergency department before the patient is discharged or admitted and are left in place until more definitive orthopedic care is instituted. All physicians should be experienced in splinting. Even if the splint is to be applied by a technician, the physician should ensure that the splint is adequately padded and the limb is stabilized in an appropriate position before the patient is discharged. In addition, the physician should reevaluate and document the limb’s neurovascular status after any reduction or splinting procedure. Use of circumferential plaster (ie, casts) is strongly discouraged in the emergency department. In almost all orthopedic injuries, soft tissue swelling worsens after discharge, potentially leading to significant neurovascular compromise if a cast has been applied in the emergency department.
Before a fracture or dislocation is reduced, adequate analgesia and muscle relaxation must be provided. The best way to accomplish fracture or dislocation reduction is with sedation using either intravenous or intramuscular agents. Emergency departments should have specific policies in place for the administration and monitoring of patients undergoing sedation. The goal is to provide sufficient sedation for the procedure without having to administer general anesthesia.
Although controversial, most authorities recommend that before sedating a patient, ensure that the patient has fasted for 4–6 hours prior to the procedure. Necessary equipment includes at least one functioning venous catheter, continuous pulse oximetry, cardiac monitor, suction, airway intubation equipment, and a bag-valve mask. Mallampati oropharynx assessment and consideration of the patient’s American Society of Anesthesiologists (ASA) categorization should be determined before beginning the procedure to ensure that the emergency physician can manage any potential airway complications resulting from sedation. In general, only ASA class I or II patients (those without serious systemic comorbid diseases) should undergo procedural sedation in the emergency department. ASA class III or IV patients should optimally receive treatment in the operating room.
Most authors recommend that patients being sedated in the emergency department receive supplemental oxygen regardless of initial oxygen saturation. The goal is to maintain an oxygen saturation above 90% at all times. It is important to remember, however, that pulse oximetry only measures oxygen saturation and does not provide any information regarding the patient’s ventilation. Many clinicians now routinely utilize end-tidal CO2 monitoring as a measure of ventilation in order to prevent hypoxemia. Many agents are available for procedural sedation. Ideally, medications should be short acting. Etomidate, 0.15mg/kg has a profound and short-lived action, which should be sufficient for most procedures. It has been reported to cause adrenal suppression, the clinical significance of which is unknown and is currently not approved for use in children. Propofol has gained widespread use in emergency medicine procedural sedation because of its rapid onset, titratable sedation effect, and quick recovery period. It also has the added advantage of antiemetic properties, which in theory would reduce the risk of aspiration during sedation. Ketamine provides distinct advantages for sedation in certain circumstances and is used commonly in children. It is effectively administered in both intravenous and intramuscular routes. It provides excellent sedation without as much risk of oversedation and hypoventilation. An alternative is the combination of agents such as midazolam and fentanyl. Be aware that a potential side effect of fentanyl is chest wall rigidity (at higher doses or with rapid boluses), which may prohibit bag-mask ventilation and may necessitate paralyzation and intubation. It is important to remember that with the use of any sedative, airway support through airway maneuvers or assisted ventilation may be needed. Adequate documentation by trained nursing staff is necessary, and sedated patients should be monitored until they can ambulate and tolerate fluids by mouth.
Unfortunately, child abuse remains a major problem in our society, with physical abuse affecting 2–5% of children in the United States. Skeletal injuries sometimes occur with abuse and may represent significant morbidity to the patient. Certain fracture patterns are commonly seen in abuse, particularly multiple fractures in varying stages of healing. Clinical suspicion of abuse should remain high whenever injured children receive treatment, particularly if fractures are found in very young patients, especially less than 3 years of age.
The approach to diagnosis should be the same as for all trauma patients. Keys to potential abuse may be evident in the history, such as history inconsistent with the injuries seen or delays in seeking care (may be evidenced by callus formation at a fracture site seen on X-rays). Physical findings may include pattern injuries, old bruises, and multiple fractures in various stages of healing.
Remember that significant force is required to produce fractures in the spine, scapula, and sternum. Rib fractures are uncommon in children except in the setting of abuse, and chest radiographs should be examined carefully to identify these injuries. Spiral fractures have long been identified as red flags to alert the emergency physician of possible abuse. This is particularly true of humeral and femoral fractures in the very young; however, spiral fractures of the tibia (Toddler’s fracture) may be seen with accidental injuries. Another common injury pattern in abuse is a chip fracture of the metaphysis. Pulling and twisting forces may also result in a tearing of the periosteum and cartilage at the growth plate of long bones, scapulae, and clavicles.
Treatment of specific injuries is described below. Careful documentation is encouraged.
Obtain appropriate pediatric, orthopedic, and social services consultations while the patient is still in the emergency department. If the patient’s safety is in question, he or she should be admitted to the hospital or taken in to protective custody by social services until all questions have been answered and the safety of the home environment is assured. All physicians are required to report suspected child abuse.
Management of Specific Orthopedic Injuries
- Chest wall deformity
- Sternoclavicular tenderness
- Sternal X-rays or computed tomography (CT) aids in diagnosis
- May be associated with mediastinal injuries
Dislocations of the sternoclavicular joint (SCJ) are the least commonly dislocated major joint and are associated with motor vehicle collisions or sports injuries. Anterior dislocations are most common and occur secondary to anterolateral force applied to the shoulder with a rolling movement. Posterior dislocations are associated with crushing forces applied to the chest, and 25% of posterior dislocations are associated with injuries to the superior mediastinal structures. The severity of the injury may be graded as follows:
- Grade I—Mild sprain of the sternoclavicular and costoclavicular ligaments.
- Grade II—Subluxation of the SCJ, may be anterior or posterior; associated with rupture of the sternoclavicular ligament with the costoclavicular ligament remaining intact.
- Grade III—Complete dislocation.
The diagnosis can often be made clinically. Tenderness, swelling, and deformity to the SCJ will be present. Patients typically use the unaffected arm to support the affected arm across the chest. Posterior dislocations can also present with dysphagia, dyspnea, dysphonia, or upper extremity weakness.
Plain radiographs, including anteroposterior, oblique, and 40° cephalic tilt views aid in the diagnosis. A CT scan may be necessary and is indicated in all cases of posterior dislocations to evaluate for mediastinal injuries.
Obtain orthopedic consultation for both anterior and posterior dislocations. Anterior dislocations may be reduced in the emergency department using procedural sedation by placing a rolled towel or sheet between the scapulae and applying traction to the affected arm. A posterior dislocation may need operative repair, and early orthopedic or trauma surgery consultation is appropriate because compression of critical upper mediastinal structures such as the great vessels and trachea may occur.
Patients with anterior dislocations may be discharged in a sling and swathe. Even if the reduction is successful, the joint is often unstable and the clavicular head may dislocate again. However, because the purpose of the reduction is often more cosmetic than functional, even if reduction is unsuccessful the patient may be discharged with immobilization in a sling and orthopedic follow-up. Posterior dislocations may be reduced with traction and adduction; however, patients should be managed in consultation with a specialist and most likely will require admission.
- Clavicle deformity
- X-rays confirm diagnosis
- Most heal with conservative management
The most common mechanism causing a clavicle fracture is a direct blow to the shoulder. Often the clavicle is deformed, and some swelling, tenderness, and occasionally crepitus are present.
Most clavicle fractures are easily seen with a clavicle series.
Treat open fractures with antibiotics and orthopedic consultation. For closed clavicle fractures, treatment typically involves pain control, immobilization with a sling, or sling and swathe.
Most clavicle fractures heal uneventfully. Factors associated with nonunion include marked initial displacement or shortening. Patients with closed fractures may be discharged with orthopedic follow-up. Patients with open fractures require hospitalization for further management.
- Deformed and tender acromioclavicular joint (ACJ)
- May be confused with clavicle injury
- X-ray may confirm diagnosis
Acromioclavicular joint injuries most commonly result from a direct fall onto the shoulder and account for 25% of all dislocations of the shoulder girdle. These injuries are graded according to severity:
- Type I—Sprain, minimal tear of the acromioclavicular (AC) ligament.
- Type II—small tear of AC ligament, widened joint space, coracoclavicular distance maintained.
- Type III–VI—Complete disruption of AC ligament, coracoclavicular ligament, and muscle attachments. In type III injuries, the clavicle is displaced upward, in type IV the clavicle displaces posteriorly into the trapezius, and in type V the clavicle is displaced superiorly. Type VI is rare and the clavicle displaces inferiorly.
Patients should be examined in the sitting position. Often a deformity at the ACJ will be present, with swelling, tenderness, and occasionally crepitus.
X-rays should include anteroposterior, axillary, and 15° cephalic tilt views. Stress views are no longer recommended. Classically, separation between the acromion and the clavicle is seen in grade II and grade III injuries. Additionally, since the coracoclavicular ligament is disrupted in a grade III injury, the distal clavicle is elevated in relation to the acromion.
Types I and II injuries are treated conservatively with a sling. Type III injuries have traditionally been treated with surgical repair; however, conservative management has been used more recently with good results.
Most patients may be discharged home. All patients should receive orthopedic referral for follow-up examination.
- Pain and tenderness over scapula
- May be associated with more severe intrathoracic injuries
- X-ray (with axillary views) confirms diagnosis
Fractures of the scapula are uncommon, accounting for approximately 1% of all fractures. Fractures usually are secondary to direct blows or to crush injuries. Because the scapula is well protected by muscle, the presence of a fracture indicates a significant mechanism of injury and warrants evaluation for other potential injuries to the lung, chest wall, humerus, and clavicle. Acromion process and coracoid process fractures have been associated with brachial plexus injury. Scapula fractures can be classified as follows:
- Type I—Fracture of coracoid process, acromion process, or scapular spine.
- Type II—Fracture of the scapular neck.
- Type III—Intra-articular fracture involving the glenoid fossa.
- Type IV—Fracture of the body of the scapula (most common).
The patient will present with pain and tenderness over the scapula. A hematoma and crepitus may also be appreciated. The patient will usually hold the affected arm close to the body.
Fractures may be subtle on plain radiographs. Always obtain an axillary view to help identify fractures involving the glenoid, acromion, and coracoid processes. In some instances, CT scanning may be necessary to identify subtle or intra-articular fractures. In children, the physis of the acromion may be seen on X-rays. In approximately 3% of individuals, this structure remains unfused (os acromiale) and can be mistaken for a fracture.
The majority of isolated scapula fractures are managed conservatively with a sling and swath and pain management. Intra-articular fractures such as those involving the glenoid often require surgical stabilization.
Significantly displaced fractures rarely may require surgical repair; patients with such fractures should be admitted. Patients with isolated scapular fractures may be discharged with close follow-up.
- Pain and decreased motion of shoulder
- Positive drop-arm test
- Plain X-ray of little value
- Arthrogram or magnetic resonance imaging (MRI) will confirm diagnosis
The rotator cuff comprises four muscles: the subscapularis (internal rotation), the infraspinatus and teres minor (external rotation), and the supraspinatus (adduction). Acute tears are commonly seen with falls, either directly onto the shoulder or on an outstretched hand, but may also occur in the setting of lifting heavy objects although most tears are chronic. Rotator cuff tears occur more commonly in middle-aged to elderly males and usually involve the dominant arm.
The patient complains of pain and decreased motion. Point tenderness over the greater tuberosity or a palpable defect may be seen. Rotator cuff tears may be evaluated by the drop arm test by passively abducting the arm to 90° and then applying pressure to the distal forearm. With significant acute tears, this will cause the patient to drop his or her arm.
Plain radiographs are usually of little use but should be obtained to rule out occult fractures. Superior displacement of the humeral head may be seen in complete tears but is not diagnostic.
Provide adequate analgesia and a sling for comfort.
Outpatient follow-up with scheduling of an arthrogram or MRI scan may be necessary to confirm the diagnosis. Patients may be discharged with orthopedic follow-up.
- Shoulder deformity, pain, and decreased movement
- Majority are anterior dislocations
- Anteroposterior, Y and axillary view X-rays confirm diagnosis
- Perform thorough nerve examination
The shoulder is the most commonly dislocated major joint in the body. Most (approximately 95%) of these injuries are anterior dislocations and are often easily diagnosed clinically; however, in muscular individuals the clinical presentation may be less obvious. Posterior dislocations are much less common and are usually associated with violent muscle contractions as seen with seizures and electrocutions but may also occur with falls on a flexed, internally rotated arm. Posterior dislocations are often missed clinically and may also be difficult to identify on standard anteroposterior X-rays. Inferior dislocations (Luxatio erecta) have been described as a type of anterior dislocation and are rare. This occurs when the humeral head is forced below the inferior rim of the glenoid fossa.
The patient usually holds the arm in adduction and the elbow flexed close to the body. Pain occurs with the least amount of movement. The glenoid fossa may be palpable. A complete neurologic and vascular examination of the extremity is of paramount importance. Axillary nerve function should be assessed by checking the sensation in the lateral aspect of the shoulder and testing deltoid motor function. Examine radial, ulnar, and median nerve distributions thoroughly prior to sedation and reduction. Document brachial and radial pulses. In inferior dislocations, clinically the patient will hold the arm locked overhead and abducted with the elbow flexed. This type of dislocation may also be associated with injury to the axillary artery and neuropraxis of the brachial plexus.
In posterior dislocations, the patient usually holds the affected arm against the chest in adduction and internal rotation. Abduction and external rotation are severely limited. The posterior shoulder may be prominent when viewed from above; however, this finding may be difficult to recognize, particularly in muscular individuals.
Obtain a shoulder series, including a scapular Y-view (Figure 28–3), which can help diagnose the direction of dislocation. Axillary views are often the most helpful if any doubt exists about the diagnosis. X-rays will also help identify associated fractures. A Hill-Sachs deformity (impaction of the posterolateral humeral head) may occur with dislocation. A fracture of the anteroinferior glenoid rim (Bankart fracture) may be seen with anterior dislocations. Bankart fractures may be subtle and identified only on CT scans.
Figure 28–3.
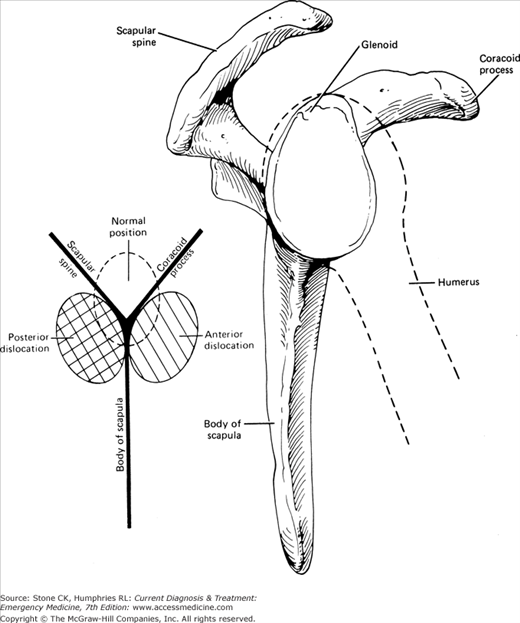
Sketch of view on tangential lateral X-ray shows the body of the scapula in its narrowest aspect. If the patient is poorly positioned, the medial and lateral borders are not superimposed. Normally, the humeral head shadow lies directly over that of the glenoid, which may be hard to see. The position of the glenoid is indicated by the confluence of the scapular spine, the body of the scapula, and the coracoid process. A dislocated humeral head lies anterior or posterior to this point.
Some controversy exists over the need to obtain X-rays prior to reduction of shoulder dislocations. We do not generally recommend bypassing X-rays at this time unless vascular compromise is present. In patients with chronic recurrent dislocations, the dislocations may occur without significant trauma; in this setting, consider reducing the shoulder before obtaining radiographs.
Emergency physicians should be comfortable with numerous reduction methods. The patient will often require sedation prior to the procedure and good muscle relaxation is key to successfully reductions. We prefer the external rotation–adduction technique for reduction. With the patient in an upright position, the extremity is externally rotated while gentle traction and adduction are applied at the elbow. This technique is associated with a low risk of injury and does not require a great deal of force, as do the other methods. The traction–countertraction method—in which an assistant applies countertraction with a sheet and in-line traction of the upper extremity—requires some physical strength (Figure 28–4). Do not try to pull the humerus into place. Instead place traction on the arm until the muscles fatigue and the humeral head slides in. The Stimson method achieves reduction by attaching weight to the wrist with the dislocated arm hanging over the bed to provide traction, but this method requires about 20–30 minutes. In scapular manipulation, reduction is performed by repositioning the glenoid fossa rather than the humeral head by rotating the inferior tip of the scapula medially while stabilizing the superior and medial edges. After reduction, reevaluate neurovascular status and immobilize the shoulder with a sling and swath. Obtain postreduction X-rays.
Discharge patients with adequate analgesia such as nonsteroidal anti-inflammatory drugs or opiates and orthopedic follow-up in 2–3 days. If any neurologic findings are present, such as a wrist drop, obtain orthopedic consultation while the patient is still in the emergency department. Most of these neurologic findings are caused by a neuropraxia and usually improve over time.
Upper Extremity Injuries
- Frequent in elderly patients
- Pain, deformity, and decreased mobility at shoulder
- X-ray confirms diagnosis
- Conservative management
Humerus fractures frequently occur in elderly women with a history of osteoporosis and the classic mechanism of injury involves a fall on an outstretched hand. In the Neer classification system, categories include two, three, and four part fractures.
The patient usually presents with deformity at the shoulder and commonly holds the affected arm close to the body. It is important to assess vascular status because the brachial artery lies in proximity to the distal humeral shaft and associated arterial injury may be present. Assess for radial nerve injury and wrist drop, particularly with humeral shaft fractures.
X-rays show these injuries clearly. Proximal humerus fractures with some impaction are the most common type.
In younger patients, look for signs of a unicameral cyst or other pathologic causes of fracture.
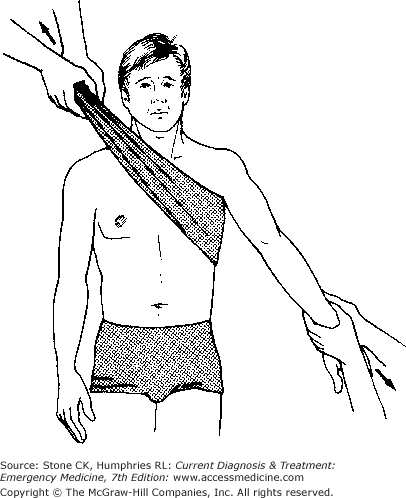
Conservative management is generally the rule, especially in the elderly. Minimally displaced fractures constitute the majority of injuries. These patients do well with a splint, sling, and swathe (Figure 28–5), or sling and swathe alone, and adequate analgesia.
Figure 28–5.
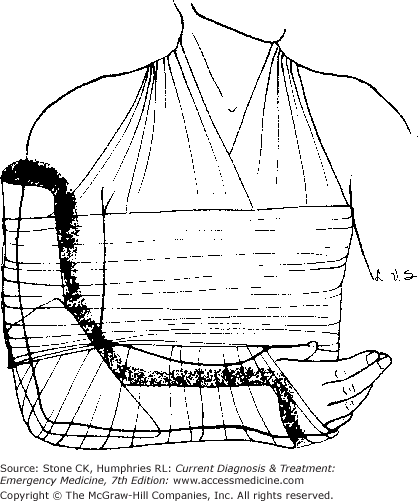
Posterior plaster splint with sling and swathe for immobilization of elbow or forearm injuries. Abundant cast padding is first wrapped around the arm. The posterior plaster must be reinforced medially and laterally to the elbow, but neither padding nor plaster should constrict the antecubital fossa.
Patients should have orthopedic follow-up in 3–4 days. We recommend obtaining orthopedic consultation for any young person with humeral or humeral shaft fractures while the patient is still in the emergency department. If there is displacement of a humeral shaft fracture, a hanging or gravity splint may be applied. Occasionally these patients may undergo open reduction and internal fixation (ORIF). The most common complication of proximal humerus fractures is a “frozen shoulder,” or adhesive capsulitis, which can be prevented with early rehabilitation.
- Occurs after FOOSH
- Elbow deformity, pain, and decreased mobility
- Posterior fat pad on lateral X-ray is highly suggestive
- May have high morbidity
- Mandatory orthopedic consultation
Supracondylar fractures are of the distal humerus and classically occur in children, usually age 5–10, who fall on an outstretched hand with hyperextension at the elbow. If not managed properly, supracondylar fractures may predispose to serious morbidity, including complications such as Volkmann ischemic contracture.
Patients usually present complaining of elbow pain and arm swelling. A neurologic and vascular examination is important and must include notation of the function of the anterior interosseous nerve, which is a purely motor nerve serving the flexor pollicis longus, flexor digitorum profundus, and the pronator quadratus. With anterior interosseous nerve dysfunction, a patient may be unable to make an “OK sign” with the thumb and index finger and may be unable to make a fist or flex the wrist.
Supracondylar fractures may be subtle and at times may be suspected only by the presence of a posterior fat pad sign on a lateral elbow X-ray. Comparison views of the uninjured elbow may be of benefit if a fracture is suspected but not immediately apparent.
All supracondylar fractures require orthopedic consultation and generally these fractures should not be reduced by emergency physicians.
Disposition is as per orthopedic consultation. Open reduction is often required and admission is recommended for displaced fractures.
- Deformity, pain, and decreased range of motion
- Assess for ulnar nerve injury
- Anteroposterior and lateral X-rays are confirmatory
- Consider fracture if posterior fat pad is present
- No X-ray needed for a simple nursemaid’s elbow
Elbow injuries usually occur from a direct blow to the elbow, causing immobility at the elbow joint. The patient generally holds the arm in flexion, and a moderate amount of swelling is present. Both fractures and dislocations may occur. Neurovascular status and range of motion testing are important, as patients who cannot fully extend their elbow have a higher possibility of having a fracture. It is important to assess ulnar nerve function by testing sensation of palmar aspect of the fifth digit and motor function of interossei muscles of the hand because of its proximity to the elbow.
X-rays should include anteroposterior and lateral views. Always look for the presence of fat pads. A small anterior fat pad can sometimes be normal; however, the presence of a posterior fat pad is abnormal and should alert the clinician to a fracture, such as a radial head fracture in adults or a supracondylar fracture in children. Even if a fracture is not visualized on X-ray, treat the injury as though an occult fracture is present.
Olecranon fractures may occur by direct trauma or less commonly by contraction of the triceps while the elbow is flexed.
Pain, limited range of motion, a palpable defect or crepitus may be present. Another physical finding includes inability to extend the elbow against force.
Plain X-rays should be sufficient to confirm the diagnosis.
Most fractures may be treated with a long arm posterior splint with the elbow flexed at 90°, sling, and orthopedic follow-up. Displaced fractures (greater than 2-mm separation) or the presence of an ulnar nerve injury mandates acute orthopedic consultation.
Patients who do not meet criteria for surgery may be discharged home as long as orthopedic follow-up can be obtained in 1–2 days.
Radial head fractures may occur by either direct trauma or more commonly by an indirect mechanism such as a fall on an outstretched hand. Damage to the articular surface of the capitellum and collateral ligament can also occur.
The patient presents with pain, particularly on supination or pronation, and with limited range of motion. Elbow extension may be limited by joint effusion.
It is often difficult to see a definitive fracture on plain X-rays. As mentioned previously, the presence of a fat pad (especially posterior) should raise suspicion for an occult fracture.
Simple radial head fractures are treated conservatively with analgesics and a simple sling. We recommend contacting an orthopedist for comminuted radial head fractures.
Patients may be discharged with immobilization, pain control, and orthopedic follow-up.
The elbow is the second most commonly dislocated major joint. Generally, the radius and ulna are displaced together and the dislocation is described as the relationship of the ulna to the humerus, such as posterior (which is most common), anterior, medial, or lateral. The most common mechanism is a fall, and associated fractures occur frequently.
The patient often holds the elbow in 45° of flexion, and a deformity at the olecranon is usually visible. Because of the location of the brachial artery and median nerve, the patient’s neurovascular status should be assessed and documented initially and reassessed frequently.
Examine plain radiographs for the presence of associated fractures.
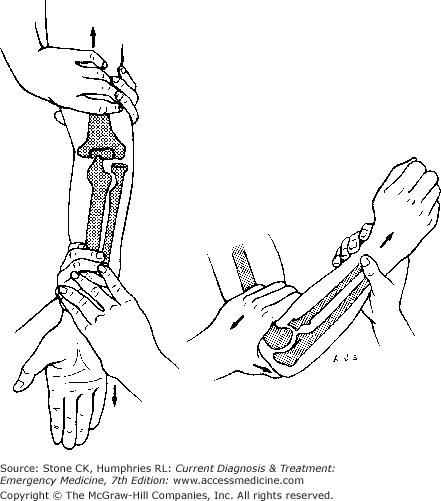
If neurovascular compromise is present, perform reduction as soon as possible. Reduction can be achieved by applying traction to the wrist distally, while the humerus is stabilized (Figure 28–6). Another technique involves applying traction at the wrist while the patient lies on his or her abdomen with the affected limb hanging off the bed. After appropriate analgesia and sedation, most dislocations can be reduced in a few minutes. These injuries should be reassessed for neurovascular injury and then placed in a long arm splint with the elbow in flexion and sling (see Figure 28–5).
Most patients may be discharged with adequate analgesia and orthopedic follow-up, as well as instructions to watch for signs of vascular impairment.
Radial head subluxation (nursemaid’s elbow) is a common injury, accounting for as many as 25% of elbow injuries in children. This injury usually occurs in the 1–3-year-old age group but may be seen up to school age and rarely in early teenagers. Subluxation occurs secondary to longitudinal traction on the arm while the elbow is extended and the arm pronated. This allows fibers of the annular ligament to slip between the radial head and the capitellum.
Generally no deformity is seen, but the child will hold the arm in passive pronation with slight flexion at the elbow. Some tenderness is present over the radial head, and the child characteristically refuses to use the arm. Although subluxation of the radial head is a common injury, obtain a thorough history to allay concerns about potential child abuse.
Some authors suggest that if the clinician is confident with the mechanism of injury and the physical examination, radiographs need not be obtained prior to reduction; however, others assert that X-rays should always be obtained to rule out other potential injuries. X-rays should be obtained if the child does not resume use of the arm after reduction.
Once the diagnosis is made, reduction is usually easily performed by stabilizing the elbow with one hand and, while applying gentle pressure on the radial head, supinating the forearm and flexing the elbow. Often a click or snap will be heard. The majority of patients regain normal use of the arm within minutes. Immobilization with a sling has been suggested; however, most patients will not comply, and if the reduction is successful, the sling likely will not make much difference.
Related posts:






Full access? Get Clinical Tree


