FIGURE 150.1 Wretland timeline of critical care and nutrition. AA, amino acids; LCT, long-chain triglyceride; PN, parenteral nutrition; TPN, total parenteral nutrition; MCT, medium-chain triglyceride; GLN-ALA, glutamine–alanine; PUFA, polyunsaturated fatty acids; EN, enteral nutrition; EPaNIC (Casaer MP), early parenteral nutrition in intensive care; SPN (Heidegger CP), supplemental parenteral nutrition. (Adapted from Berger MM. The Arvid Wretlind lecture: evolving concepts in parenteral nutrition. Clin Nutr. 2014;33(4):563–570.)
The ebb phase of injury is the immediate response to tissue injury with hemodynamic disturbances and reperfusion that occurs in patients with severe traumatic injury, burns, brain injury, major complicated surgical procedures, and severe sepsis. It is characterized by a pronounced acute phase reaction. The flow phase follows and the metabolic environment changes with increased levels of catecholamines and cortisol that promote the hypermetabolic state of increased energy expenditure and the hypercatabolic state of protein turnover. This can be viewed as an adaptive response that provides the brain and injured tissues with substrate to promote healing.
A well-nourished average male has significant stores of calories in the form of adipose (141,000 kcal) and protein (24,000 kcal) with minimal stores in the form of carbohydrates (900 kcal). While adipose tissue is expendable and can be utilized as fat calories, this is not so for protein, as all proteins are used for either structure or function (Table 150.1). Wasting of protein stores results in weakness and debilitation with poor outcomes associated with prolonged ventilator dependence, recurrent infections, and organ system dysfunction (1).
During the adaptive flow phase, resultant insulin resistance is responsible for the decreased peripheral use of glucose and the increased rates of lipolysis and proteolysis for the provision of amino acids and fatty acids as fuel substrates (Fig. 150.2). In contrast to the state of stable starvation, the conversion of peripherally mobilized amino acids (primarily alanine), lactate, and pyruvate to glucose by gluconeogenesis is not suppressed by hyperglycemia or the infusion of glucose solutions in this catabolic state. Branched-chain amino acids are used preferentially as fuel in skeletal muscle. There are some amino acids that are taken up selectively by tissues for specific purposes. For example, glutamine, a conditionally essential amino acid is taken up by the proximal nephron to sustain ammoniagenesis and to counteract acidosis, by fibroblasts and enterocytes to promote healing and by immune cells for replication (10).
Decreased protein synthesis in skeletal muscle and the gastrointestinal tract is accompanied by increased protein breakdown, with the shuttling of amino acids to lung, cardiac, liver, and splenic tissue, where protein synthesis is better maintained. As this catabolic process is reinforced by pro-inflammatory cytokines, glucocorticoids, and oxidative stress, the critically ill and injured patient remains catabolic and consumes skeletal and visceral muscle and fat reserves rapidly. At the same time, autophagy occurs. This is a well-recognized physiologic process where cells can eliminate large protein aggregates. It has been suggested that autophagy plays an important adaptive role in the critical care setting to aid in immune function and prevent organ failure. Recently, it has been suggested that early feeding interferes with autophagy and thus is detrimental; however, this has not been adequately substantiated to justify withholding of nutritional support (11).
| TABLE 150.1 Functions of Proteins (10) |
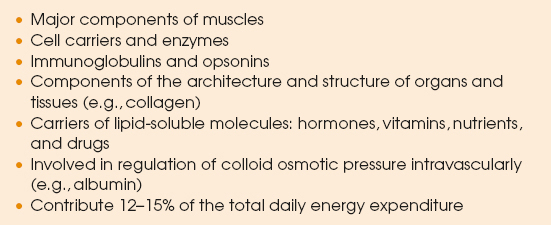 |

FIGURE 150.2 Catabolic metabolism. HBCC, high branched–chain amino acids; AA, amino acids; ACP, acute-phase reactants; FA, fatty acids; TGA, triglycerides.
If the stress state is prolonged, the amino acid pool will become depleted of essential amino acids and protein synthesis cannot match the increased rate of muscle protein breakdown. Thus, malnutrition may be manifested as a functional deterioration in organ system function along with poor wound healing or wound breakdown. Respiratory muscle weakness can predispose to atelectasis, pneumonia, and prolonged ventilator dependence. All aspects of the immune response may be impaired by malnutrition. Host barrier function may be compromised together with cell-mediated and humoral immunity as cell growth and turnover are diminished. This, in turn, prolongs the stress state and results in poor outcomes and long-term functional disability (12). This has been substantiated in septic patients with a prolonged ICU stay, where altered plasma aminograms have been associated with increased mortality (13).
The catabolic state is exacerbated by the development of anabolic resistance, where a patient is resistant to the normal anabolic effect of amino acids on muscle protein synthesis (10). This is seen in the newly recognized syndrome of persistent inflammatory catabolic syndrome (PICS) that appears to be more pronounced in older patients (14). Three factors have been described that contribute to anabolic resistance. One is splanchnic sequestration of amino acids following feeding, another is insulin resistance, and the third is the blunted response to the anabolic properties of leucine (10). Exogenous protein sources may stimulate protein synthesis to offset this accelerated rate of proteolysis and amino acid oxidation, but there are no studies that have determined the route or dose (15).
DIAGNOSIS OF MALNUTRITION IN THE CRITICALLY ILL
Malnutrition can be a difficult diagnosis in the critically ill patient and often goes unnoticed as attention is drawn to the therapy of shock, respiratory failure, and sepsis. It can develop rapidly, even in patients with adequate nutritional stores at baseline. Thus, it is more meaningful and prognostic to diagnose nutritional risk in these patients. It has been demonstrated that those with the highest risk have the worst outcomes with nutritional deficits and benefit the most from interventions (16–18). In fact, some of the controversial issues in the current literature are a consequence of the entry of patients with low nutritional risk into large clinical trials.
When a patient is challenged with a critical illness, several factors contribute to nutritional risk. The patient may enter this illness malnourished, adequately nourished, or obese. The pre-existing state of health and comorbidities also contributes significantly. In addition, the magnitude of the illness itself is a major contributor to nutritional risk. Many scores have been developed to identify nutritional risk and many of them take into account baseline nutritional status, inflammation, and severity of illness. The two scores that have been recommended by the most recent guidelines include the Nutritional Risk Score (NRS) 2002 and the NUTRIC Score (16–18).
| TABLE 150.2 The Nutritional Risk Score (NRS 2002) | ||
 | ||
The NRS is widely accepted and used in Europe (Table 150.2). It assesses risk with the evaluation of undernutrition and the assumption that increased disease severity increases nutritional requirements. It is easier to calculate, than the NUTRIC Score, but in the ICU where historic dietary information may not be available, it may not be universally applicable. A score higher than 3 signifies risk, and a score of 5 or higher signifies high risk.
A more recent scoring system that has been validated in critically ill patients is the NUTRIC Score (Table 150.3) (18). Initially, this score utilized inflammatory markers such as IL-6, but due to the difficulty in obtaining these results, the score has been validated without them. A score of 5 or more without IL-6 defines a high-risk patient. An assessment of nutritional risk should be performed on all patients upon entering the ICU. Additionally, those patients initially with a low risk score should be reassessed frequently as a change in condition could render them high risk.
| TABLE 150.3 The NUTRIC Score (without IL-6) | ||
 | ||
Just as patients may enter into a septic episode or critical illness with different macronutrient stores, they also may have their own set of micronutrient deficiencies. These micronutrient deficiencies may exist due to choices in food ingestion, medications, and surgical malabsorptive procedures. Catabolic critically ill patients with severe burns, major trauma, septic shock, massive gastrointestinal losses, and continuous renal replacement therapy are at risk of micronutrient deficiencies due to increased utilization, compartment shifts, and losses. Vitamins and minerals are important in cellular processes; their deficiencies may be associated with end-organ dysfunction, and may affect the response to sepsis and nutritional support (19–21). Testing for serum levels of these micronutrients currently is the only available tool to evaluate for their deficiency.
NUTRITIONAL THERAPY
Timing and Calculating Dosages of Nutrients
How to determine the optimal dosing and timing of caloric, protein, and micronutrient administration is still not clearly understood. Fixed-weight formulas are incorrect in 70% of ICU patients. This issue has gained importance with the recent appreciation of the narrow range of optimal nutritional support needed to avoid underfeeding and overfeeding.
It seems evident that feeding during the ebb phase of injury during the critical period of resuscitation is not indicated in most patients. However, within 24 to 48 hours of admission, once hemodynamic stability and resuscitation have been completed, enteral feedings should be started for those patients with an assessment of high nutritional risk (see Tables 150.2 and 150.3). In select circumstances, enteral nutrition can be started in patients who are stabilizing and weaning from vasopressor support (16). Early enteral feedings can promote gut-mediated immunity, maintain microbial diversity, and attenuate the hyperdynamic stress response associated with the immune suppression seen with serious trauma, brain injury, severe illness, and major operative interventions (22,23). These benefits may be even more pronounced in burn patients where even earlier enteral feeding initiation has been found to attenuate the stress response. To accomplish this, a nutritional bundle should be implemented empowering bedside nurses to participate in feeding decisions and metabolic monitoring (Table 150.4) (16). Additionally, admitting and covering physicians will need to endorse this clinical approach. An aggressive approach for enteral access is needed, and should be placed operatively for surgical patients, and postpylorically whenever gastric ileus may inhibit goals of therapy. A model for early patient selection has been developed for trauma patients, taking into account feeding difficulties with multiple radiologic and operative procedures (Fig. 150.3) (24).
| TABLE 150.4 ICU Enteral Feeding Bundle |
 |
Management becomes more challenging when full enteral feeding is not possible or successful. If full enteral feeding volumes cannot be met, protein modules can be added to meet protein requirements. Calories added from intravenous fluids and lipid-based medications may add sufficient supplemental calories to meet at least 60% to 80% of calculated goals. The question is then raised whether parenteral support should be initiated early on in the course of illness, as total support or supplemental support when 60% of calculated goals cannot be met utilizing the above strategies. For patients at high risk, or dependent on parenteral nutrition at baseline, early support by day 3 should be considered when enteral feedings are not feasible or successful (25). For supplemental parenteral nutrition, calories and protein from enteral support that are tolerated should be included with supplemental parenteral calories and protein given to reach 80% of goals. It would be unusual for a standard parenteral formula to be appropriate in this circumstance without resulting in caloric overfeeding. Customized hypocaloric, high-protein formulas are most appropriate in this setting, attempting to achieve between 1.3 and 2.0 g/kg of protein daily.
Indirect calorimetry yields the most accurate information regarding an individual patient’s energy utilization, but it still requires interpretation regarding therapeutic goals. Ventilator support, renal replacement therapy, and pain issues can interfere with results. In the early stages of a patient’s critical care, a conservative interpretation would seem to be the best. The Harris–Benedict equations can also be used to set at basal to 1.3 times the requirements when indirect calorimetry values are not available (Table 150.5). It is important to realize that these equations are most often incorrect in underweight and overweight patients. Also, simple weight-based equations may be used with 25 to 30 kcal/kg/d, but these do not take into considerations the changes in requirements associated with age and gender.

FIGURE 150.3 Trauma care nutritional support algorithm. ISS, injury severity score. (Adapted from Byers P, Block E, Albornoz J, et al. The need for nutritional intervention in the injured patient: the development of a predictive model. J Trauma. 1995;39:1103–1109.)
| TABLE 150.5 Harris–Benedict Equations |
 |
In addition to calculating caloric requirements, the composition of the macronutrients must be considered. Excess carbohydrates can cause problems with blood sugar and carbon dioxide production, which can be associated with increased complications and ventilator days. Carbohydrate calories should not be increased until blood sugar is under adequate control. If there are concerns regarding carbon dioxide production, carbohydrates should be limited to 4 mg/kg/min. It is also important that all dextrose-containing intravenous fluids administered be quantified and their calories added to the support be received. Fat calories should be limited to 20% to 30% of total calories, with more severe restriction during the first week of a critical illness and in septic patients. This includes calories inadvertently administered while infusing medications in lipid emulsions.
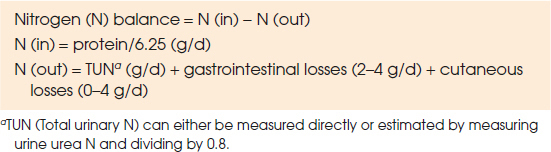
Recent studies that focused on protein administration have suggested that protein support may be paramount early on in critical illness and may require a separate analysis (26). Daily protein requirements are in the range of 1.3 to 2.0 g/kg/d in critically ill patients, and can be measured using nitrogen balance studies (Table 150.6) (27). Obese patients and those with high-volume protein losses may require as much as 2.5 g/kg/d of ideal body weight to reach adequate support. Achieving both protein and caloric goals has been demonstrated to decrease mortality in ICU patients (1).
Critical illness in the morbidly obese as a consequence of surgical complications or other acute illnesses is an especially challenging situation. Surgical complications present the problem of maintaining lean body mass and promoting wound healing, without overfeeding and attempting to achieve some ongoing weight loss. Guidelines from the American Society of Enteral and Parenteral Nutrition and the Society of Critical Care Medicine have advocated hypocaloric, high protein nutritional support in these patients (16). Caloric support of only 50% to 70% of predicted energy needs from standard equations or less than 14 kcal/kg of actual body weight has been proposed. Protein support is recommended at 1.2 g/kg of actual weight or up to 2.5 g/kg of ideal body weight (28). If this strategy is used, monitoring of nutritional status and response to the support, such as wound healing, is of paramount importance.
| TABLE 150.6 Nitrogen Balance Equations |
 |
It is also important to be mindful that as critical illness progresses, caloric requirements may increase as deficits are created. After 7 to 10 days, as patients progress to a more “chronic” critically ill phase, they will require increased caloric support at 1.5 times the resting measurement or basal calculation to reduce caloric deficits and diminish adverse outcomes. Patients with special needs such as those with acute kidney injury on continuous or intermittent renal replacement therapy actually need more protein (≤2.5 g/kg) due to losses associated with this acutely catabolic state and the therapy itself (16). Protein support should not be withheld in patients with this condition. Renal replacement therapy can be used to allow adequate protein support as needed.
Metabolic Monitoring
Regardless of the form of nutritional support, it has been demonstrated that careful metabolic monitoring of the patient results in more effective therapy. An aggressive approach to feeding patients with high nutritional risk requires careful monitoring for refeeding syndrome during the early stages. In all patients, routine electrolytes should be monitored and replaced, with a focus on magnesium and phosphorus. While hypomagnesemia may be associated with cardiac dysrhythmias, hypophosphatemia is very common in malnourished patients with refeeding and is associated with decreased respiratory muscle function and weaning failure.
As critical illness is dynamic, caloric and protein requirements can change during its course. In addition, as the illness progresses, a patient can transition from a status of low risk to one of high risk. For this reason, it is recommended to perform metabolic monitoring, with full assessment either once or twice per week to determine if caloric and/or protein deficits have developed. Calorie requirements based on resting energy expenditure should be rechecked weekly. Formula-based calorie requirements are less likely to change, but liberalizing caloric support with prolonged illnesses is probably indicated. Changes in protein turnover can be monitored with nitrogen balance studies in those patients that maintain a urine output and have adequate kidney function. Measurement of serum protein markers is is no longer indicated in the early phases of critical illness, as they reflect the inflammatory milieu more than the state of nutritional adequacy (16).
The most important monitoring to ensure the best practice is to have a daily assessment of the nutrition support that was actually received by the patient with reasonable attempts to minimize calorie and protein deficits. Patients on parenteral nutrition should be monitored for return of gastrointestinal function and their ability to transition to enteral support. An additional useful parameter to follow is adequate wound healing, with the assumption that inadequate wound healing could be due to insufficiency of macronutrients and micronutrients.
SELECTING THE ROUTE OF ADMINISTRATION
Enteral Feedings
Whenever possible, patients with a functional gastrointestinal tract should have the enteral route utilized for nutrition support. It must be recognized, however, that it is more difficult to achieve adequate nutrition using this method, and ongoing caloric deficits have been associated with poor outcomes. Adequate support via the enteral route in the ICU requires a “therapy bundle” designed to overcome the usual barriers of late initiation and loss of support due to frequent interruptions (see Table 150.4) (16,29). The most common causes of interrupted enteral nutrition have been identified as extubation, fasting for procedures, loss of enteral access, and elevated gastric residual volumes (30,31). To overcome these barriers, it is necessary to carefully monitor the volume of enteral nutrition actually delivered. Volume-based rather than a rate-based ordering systems have demonstrated more effective delivery of calories and protein during the first week of illness, with only a slight increase in diarrhea (32). The volume of feedings required can be given over a cyclic period after feedings are resumed so that the prescribed nutrition is delivered. Calorie and protein deficits should be assessed on a daily basis to limit the underfeeding that is often present.
Access Considerations
In patients with adequate gastric emptying, bolus feeding into the stomach can be accomplished easily and may be associated with the release of important enterohormones (33). In addition, this technique makes volume-based nutritional support easier so that feedings missed due to procedures can be given when the infusions are resumed (34). The difficulty with this approach is that it may be associated with a higher incidence of aspiration. Patients must be carefully selected and monitored closely for tolerance in an attempt to avoid this serious complication (16). For this reason, most recent recommendations are to feed continuously or cyclically in critical care patients. In cases of gastric ileus or partial obstruction or in those patients with a high risk of aspiration, postpyloric feeding access is recommended (16). This route can deliver adequate enteral nutrition more effectively and has been shown to be associated with a 30% decrease in the rate of pneumonia in enterally fed patients (35). This type of access is technically difficult, but with expertise can be achieved at bedside; fluoroscopy or endoscopy may be required in some cases. Those patients with high nutritional risk who have abdominal surgery should have enteral access placed at the time of surgery whenever possible.
Choosing a Formula
Whey-based protein formulations are higher in leucine and thus have a theoretical anabolic advantage of increased insulin release and protein synthesis than soy- or casein-based formulas (33). Enteral formulas come in varying concentrations varying from 1 to 2 kcal/mL of formula. It has been demonstrated that utilization of a more calorically dense formula with 1.5 kcal/mL resulted in significantly more calories being delivered in critically ill, enterally fed patients, without the adverse effects of increased gastric residual volumes or diarrhea (36). Some of these calorically dense formulas, however, may not have adequate protein so that protein modules are necessary to meet nitrogen requirements. These can be given even before caloric goals are met in order to reach protein goals earlier. Because most formulas only contain 65% water, it may be necessary to administer hypotonic enteral fluid boluses in patients without intravenous maintenance fluid to avoid dehydration.
The formula selected should conform to the patient’s nutritional needs, accounting for any fluid restrictions and organ system dysfunction. The amount of carbohydrate and fat calories delivered in an enteral prescription must be assessed. Concentrated formulas with more than 1 kcal/mL usually accomplish this goal by increasing fat calories. Although it is not recommended to routinely use formulas with 2 kcal/mL, as these formulas have a high fat content and may promote an inflammatory response, they may be useful in stable patients with volume overload (16). Patients with intestinal mucosal atrophy may be unable to absorb these calories and might require semi-elemental or peptide formulations. In addition, very low–fat elemental formulas may be needed in patients with severe malabsorption or pancreatitis.
There are many specialized formulations of enteral products. Use of immune-modulating formulas with arginine, glutamine, and nucleic acids has been controversial; however, they may be considered early on in surgical patients at high risk, such as the severely injured trauma patients, patients with severe burns, and in patients with traumatic brain injury (16). There are also commercial products that have increased fiber and fat calories for diabetics, formulas that have adjusted electrolyte composition and concentrated calories for renal failure, and those with amino acid and protein adjustments for hepatic insufficiency. These products are far more expensive than the standard enteral products and should have clear indications for their use. For example, the diabetic formulas should only be used if blood sugars cannot be adequately controlled with aggressive insulin regimens. In patients with kidney failure, a standard concentrated formula can administered, unless electrolyte abnormalities cannot be managed with the prescribed hemodialysis regimen. Patients undergoing renal replacement therapy actually have high protein requirements and these formulas often fall short in protein content. There is almost no circumstance where specialized hepatic formulas are needed, as encephalopathy is usually adequately controlled with standard enteral medical therapies. In addition, protein support in these patients should be aggressive and hepatic formulations do not contain adequate amounts of protein.
In addition to a standard enteral formula of 1 or 1.5 kcal/mL, it is also recommended to administer a soluble fiber product, such as apple pectin, routinely to all patients with a colon in continuity. Soluble fiber is fermented to short-chain fatty acids in the colon and is a source of nutrition for the colonocytes and helps to maintain gut barrier function. In addition, soluble fiber helps to modulate and maintain a healthy colonic microbiome, and thus helps to decrease the number of pathogens that may be found in the colons of critically ill patients. The recommended dose is up to 2.5 to 5.0 g every 6 hours (16).
Complications
The most common complication associated with the enteral route of feeding is malnutrition due to serious underfeeding as a consequence of poor protocols and nursing techniques (37). This risk can be minimized by employing aggressive nutritional protocols coupled with vigilantly monitoring the nutritional status and support of each patient, with caloric and protein deficits calculated daily.
Aspiration is another serious complication of enteral feeding. The risk can be mitigated by keeping the head of the bed elevated at 30 degrees whenever possible. In patients demonstrating poor gastric emptying, postpyloric access should be considered. However, when there is abdominal distention and ileus, tube feeding should be immediately decreased or discontinued and investigation into the possibility of nonocclusive intestinal necrosis should be undertaken. With prompt recognition and surgical intervention for source control, an improvement in survival rate can be accomplished with this devastating and highly lethal complication (38).
There are multiple complications that can occur with enteral access. Nasoenteral tubes can be incorrectly placed into the airway or become dislodged. This can be seen or suspected as symptoms develop or when reviewing radiographs and scans. New technology in tube design is being developed so that this complication can be avoided or recognized in a more timely fashion without radiographs. Dislodgement of percutaneous tubes with gastrointestinal contents or tube feeding leaking into the peritoneal cavity is another complication that can occur. Finally, tube occlusion contributes greatly to underfeeding and should not occur with frequent flushing and appropriate nursing care of feeding access tubes.
Parenteral Nutritional Support
Parenteral nutrition is life saving for patients unable to absorb or tolerate adequate amounts of enteral formulas. There is a general consensus that parenteral support should be started in high-risk patients unable to receive adequate enteral nutrition by day 3 of illness or injury (39).
Access Considerations
Central parenteral formulations require central venous access in the form of central venous catheters or PICC lines. Whatever access is selected, there should be a port preserved for parenteral nutrition infusion only. Although PICC lines may be placed with fewer complications, they may not be possible in all patients, so that central venous catheters will be necessary in some cases. Midlines and peripheral intravenous lines can be used for peripheral parenteral formulas; however, these solutions are usually not adequate for full caloric and protein support without utilizing a high percentage of fat calories along with large fluid volumes.
Calculating the Correct Formula
Standard parenteral nutrition formulations are rarely appropriate in critically ill patients. When developing a custom parenteral formulation for a patient in the ICU, dextrose should be the major caloric form, but should not exceed a carbohydrate dose greater than 4 to 5 mg/kg/min, as this has been shown to be the maximal oxidation capacity in adults and children. How the formula is ordered will depend on whether the pharmacy has an order form with total grams of dextrose and amino acids prescribed or still uses order forms with percentage concentrations. The grams of protein support to be administered should be determined, and then the caloric contribution is calculated, as above, at 3.4 kcal/g of parenteral protein. The protein calories are then subtracted from the total caloric prescription to determine the nonprotein calories needed to be administered.
Next the fat calorie requirement is calculated to be 20% to 30% of the total caloric prescription. As lipid emulsions are most commonly 20%, they contain 2 kcal/mL, so that the volume of the emulsion is easily calculated from the caloric requirement. Note that fat emulsions can be given daily in smaller quantities or in 250-mL doses intermittently throughout the week, depending upon the pharmacy’s admixture capabilities. The contribution of caloric support from fat is then subtracted from the nonprotein calories to determine the calories to be supplied from dextrose, calculated at 3.4 kcal/g. The total number of grams of dextrose and amino acids may be ordered separately from the volume of the formula or calculated as a percentage solution, depending on the order form used. The volume of parenteral support ordered should be determined based on the patient’s fluid restrictions and the osmolarity of the solution. Most patients can be fully supported on 1.5 to 2 L of a custom formula.
The parenteral nutrition prescription may also contain micronutrients and compatible medications. Repletion of the trace minerals, copper, zinc, and selenium, in critically ill patients with major losses and risk of deficiencies has resulted in improved immunity and wound healing, fewer infectious complications, and shortened length of ICU stay (21,40). Edema of the gastrointestinal tract and competition of absorption between copper and zinc make the intravenous route of repletion most reliable when severe deficiencies exist. Table 150.7 covers daily requirements of vitamins and minerals. In addition, water-soluble vitamins and histamine-2 antagonists can be added to the parenteral nutrition prescription.
The formula calculated should be dynamic and reassessed based on the patient’s ongoing needs and ability to tolerate enteral nutrition. Enteral feedings should be initiated as early as safely feasible; however, parenteral nutrition support should be continued as an adjunct until at least 60% to 80% of calories are tolerated and being consistently administered via the enteral route.
Complications
While underfeeding is the most common complication of enteral support, overfeeding is often a complication of parenteral nutrition and may predispose to adverse outcomes. Overfeeding is associated with increased levels of metabolic stress and is permissive of hepatic steatosis. Increased levels of cortisol, epinephrine, and glucagon have also been recognized.
In the early days of parenteral nutritional support, permissive hyperglycemia was felt to be acceptable; however, more aggressive blood sugar control is now an important component of nutritional and ICU therapy. The hyperglycemia that often accompanies or occurs with overfeeding is associated with glycosuria, electrolyte derangements, hyperosmolarity, and an increased incidence of infections. This metabolic derangement should be treated aggressively by adjusting carbohydrate calories and regulating insulin infusions to maintain a blood sugar level below 180 mg/dL (41). When subcutaneous dosing of insulin is used, Humalog insulin should be considered due to its faster onset of action and quicker rebound of blood sugars (42). In patients with poor control, continuous insulin infusions may be necessary. Although insulin may be added to the parenteral nutrition formula at 50% to 60% of the previous day’s requirements, this should only be done in stable patients who are not in flux with insulin resistance.
Hypercarbic respiratory failure may be induced by carbon dioxide production from excessive carbohydrate caloric loads. This complication can be diagnosed and avoided with the utilization of indirect calorimetry and maintaining the respiratory quotient below 1. When indirect calorimetry is not available, keeping the carbohydrate load to no more than 4 mg/kg/min should attenuate carbon dioxide production.
The requirement of central venous access introduces the risk of catheter-related sepsis in patients requiring parenteral nutrition. A dedicated port on the central venous catheter should be used for the parenteral nutritional products with protection from mixed use. In addition, protocols using alcohol and antibiotic locks have been introduced as measures to prevent infection. The diagnosis of a line infection has become more difficult, but optimally should be done via a quantitative technique of line culture. Blood cultures obtained from central lines and peripheral veins can be performed when line sepsis is suspected, and under normal circumstances, lines should be changed and antibiotic therapy initiated.
| TABLE 150.7 Vitamins and Mineral Requirements | ||
 | ||







Full access? Get Clinical Tree


